what is the use of magnesium oxide in super refectory status epilepticus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"magnesium" AND "super-refractory status epilepticus"
Searching the Web
magnesium oxide super refractory status epilepticus mechanism use
Reading Article
PMID: 39216051
Reading Article
PMID: 36979664
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC8219503
I now have comprehensive information to provide a thorough answer. Note that the question asks specifically about magnesium oxide, but all clinical evidence and protocols use magnesium sulfate (MgSO4) - let me address this distinction clearly.
Magnesium in Super-Refractory Status Epilepticus (SRSE)
Important clarification first: In clinical practice, magnesium sulfate (MgSO4) - not magnesium oxide - is the form used intravenously for super-refractory status epilepticus. Magnesium oxide is an oral/enteral formulation with poor bioavailability and is not used IV. The discussion below applies to the clinically relevant form (MgSO4), though oral magnesium oxide is occasionally used for electrolyte repletion in ICU patients.
What is Super-Refractory Status Epilepticus?
SRSE is defined as status epilepticus that persists 24 hours or more after initiation of general anesthesia, or recurs on reduction of anesthesia. It carries significant mortality (~3%) and long-term morbidity including cognitive decline and recurrent seizures.
Mechanism of Action
Magnesium acts primarily as an NMDA (N-methyl-D-aspartate) receptor antagonist. This is highly relevant to SRSE because of the "Receptor Trafficking Hypothesis":
- In prolonged seizures, GABA-A receptors are downregulated and internalized from the synapse
- Simultaneously, NMDA and AMPA (glutamate) receptors are upregulated
- This shift explains why benzodiazepines (which act on GABA-A) lose efficacy, while NMDA antagonists become particularly relevant
- Magnesium blocks the NMDA receptor channel pore in a voltage-dependent manner, reducing excitatory glutamatergic transmission
- This complements the mechanism of ketamine (another NMDA antagonist also used in SRSE)
A 2023 review in Biomedicines (PMID 36979664) specifically classifies magnesium sulfate among NMDA antagonists that are "reasonable optional adjuvant therapies" in SRSE, alongside ketamine, with the caveat that randomized prospective data are still lacking.
Clinical Use and Dosing Protocol
Magnesium is used as an adjuvant (add-on) agent in SRSE after failure of first-, second-, and third-line agents. It is listed in major institutional protocols including the MGH Status Epilepticus Protocol.
| Parameter | Detail |
|---|---|
| Loading dose | 4 g IV bolus |
| Maintenance infusion | 2-6 g/hour |
| Target plasma level | 3.5 mmol/L (some case reports titrated up to 3.8-6.5 mg/dL) |
| Route | Intravenous (MgSO4) |
| Monitoring | Continuous cardiovascular monitoring, deep tendon reflexes, serum levels |
A 2024 case report in Neurology India (PMID 39216051) describes the longest reported successful use of magnesium sulfate infusion for SRSE - in a patient with probable anti-GABA-B autoimmune encephalitis, seizure control was achieved after 11 days of infusion, with serum levels titrated to 3.8-6.5 mg/dL.
Why it is Used in SRSE Specifically
- Complementary mechanism - targets glutamate excitotoxicity, which is dominant in prolonged SE when GABAergic drugs have lost efficacy
- Relative safety - compared to deep anesthetic agents (propofol, pentobarbital), magnesium carries lower risk of hemodynamic compromise at standard doses
- Adjuvant to anesthetics - can be combined with ongoing anesthetic infusions to allow dose reduction
- Potential neuroprotection - NMDA blockade may reduce excitotoxic neuronal injury in prolonged seizures
- Specific utility in autoimmune SRSE - case series document benefit in NORSE (New Onset Refractory SE) and FIRES (Febrile Infection-Related Epilepsy Syndrome)
Adverse Effects / Contraindications
| Adverse Effect | Note |
|---|---|
| Hypotension | Especially at high infusion rates |
| Cardiac arrhythmia | Monitor continuously |
| Neuromuscular blockade / respiratory depression | Check deep tendon reflexes as a clinical proxy |
| Hypermagnesemia | Requires serum level monitoring |
| Contraindicated in severe renal failure (CrCl <30 mL/min) | Magnesium is renally excreted |
Place in the Therapeutic Algorithm
Magnesium is a 4th-line (or later) agent in SRSE, used alongside or after:
- Repeat burst suppression
- Additional non-anesthetic AEDs (e.g., topiramate, carbamazepine)
- Ketamine (another NMDA antagonist, often preferred as first NMDA agent)
- Pyridoxine (for pyridoxine-dependent SE)
- Immunomodulation (steroids, IVIG, plasma exchange) for autoimmune causes
- Ketogenic diet
- Hypothermia, neurosurgery, or deep brain stimulation in extreme cases
Bottom line: Magnesium sulfate (as an NMDA receptor antagonist) is a recommended adjuvant option in SRSE - particularly when GABAergic agents have failed, in autoimmune encephalitis-associated SRSE, and in settings where its relative cardiovascular safety is advantageous. Evidence remains limited to case reports and case series, but it is included in major institutional protocols. The oral form (magnesium oxide) has no role in acute SRSE management but may be used for ongoing electrolyte repletion in ICU patients.
Treatment for the hsv encephalitis
Finding Sources
Searching PubMed
"herpes simplex encephalitis" AND treatment
Searching the Web
HSV encephalitis treatment guidelines 2024 acyclovir duration management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive, textbook-based summary of HSV encephalitis treatment:
Treatment of HSV Encephalitis
The Golden Rule: Start Empirically - Don't Wait
HSV encephalitis is fatal if untreated (mortality >70%). Acyclovir must be started empirically at the first clinical suspicion - before CSF PCR results return, before MRI confirmation. Even if the first LP is done within 24 hours and CSF is normal, do not stop acyclovir - false-negative PCR is possible early in the illness.
- Harrison's Principles of Internal Medicine 22E, p.1506
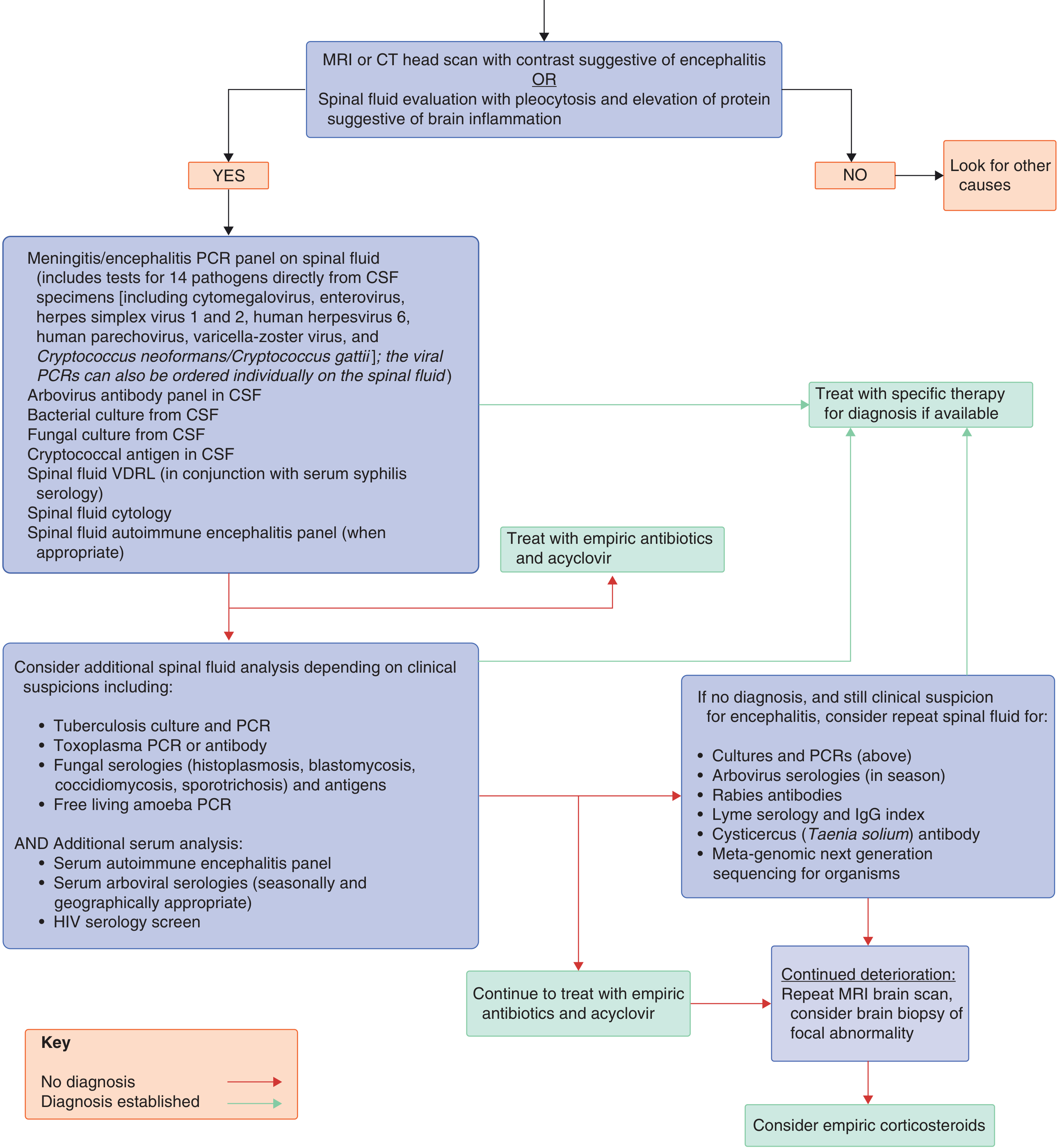
Diagnostic Approach (Flowchart)
The flowchart below from Goldman-Cecil Medicine guides the approach: treat empirically with antibiotics + acyclovir while investigations are pending, and continue until diagnosis is confirmed or excluded.
1. Specific Antiviral Therapy
| Parameter | Detail |
|---|---|
| Drug of choice | IV Acyclovir |
| Dose | 10 mg/kg every 8 hours (= 30 mg/kg/day) |
| Duration | 14-21 days |
| Route | Intravenous only (inadequate CNS penetration with oral formulations at standard doses) |
| Renal impairment | Dose must be reduced; monitor serum creatinine |
| Obese patients | Dose based on ideal body weight |
After completing IV therapy in neonates specifically, oral acyclovir suppression (300 mg/m²/dose every 8 hours) is continued for 6 months to improve neurodevelopmental outcomes.
- Goldman-Cecil Medicine, p.3299
- Adams and Victor's Principles of Neurology 12e, p.451
- Katzung's Basic and Clinical Pharmacology 16e
2. When to Stop or Continue Acyclovir
- If CSF HSV PCR is positive: complete full 14-21 day IV course, then perform repeat LP to confirm PCR negativity before stopping
- If CSF is still PCR-positive at end of treatment: continue IV acyclovir with weekly PCR until negative
- If PCR is negative but clinical suspicion remains high (e.g., normal early CSF in first 24 hours, classic MRI pattern): continue acyclovir and repeat LP after 24-48 hours
- If PCR is negative and alternative diagnosis is established: acyclovir can be discontinued
- Immunocompromised patients: treat for at least 21 days; consider long-term oral suppression until CD4 >200
3. Mechanism of Acyclovir
Acyclovir works because HSV, VZV, and EBV all encode viral thymidine kinase, which phosphorylates acyclovir to acyclovir-5'-monophosphate. Host cell enzymes then convert it to the triphosphate form, which acts as a competitive inhibitor of viral DNA polymerase and causes chain termination. Uninfected cells lack viral thymidine kinase, giving the drug its selective toxicity.
- Harrison's Principles of Internal Medicine 22E, p.1506
4. Supportive Management
| Issue | Management |
|---|---|
| ICP elevation | Fluid restriction, avoid hypotonic IV solutions, careful ICP monitoring; all standard measures for cerebral edema apply |
| Seizures | Treat with standard anticonvulsant regimens; prophylactic antiepileptics are reasonable given high seizure frequency in severe encephalitis |
| Fever | Active suppression |
| Respiratory/BP | Continuous monitoring; ICU care in severe/early stages |
| Complications | Aspiration pneumonia prevention, DVT prophylaxis, pressure ulcer care, catheter infection vigilance |
| Mass effect / hemorrhagic necrosis | Large-volume temporal lobe involvement can behave like an expanding lesion; coma + pupillary changes may indicate brainstem compression or direct spread - assess with imaging |
5. Corticosteroids - Controversial
The concern that steroids aggravate HSV infection has not been borne out clinically, but their value is also unproven and no randomized trials exist. They may be considered for:
- Significant cerebral edema with mass effect
- Post-HSE autoimmune encephalitis (see below): methylprednisolone 1 g IV daily for 5 days
Current guidelines do not recommend routine corticosteroids for acute HSV encephalitis.
6. Post-HSE Autoimmune Encephalitis - An Important Complication
Up to 25% of patients develop anti-NMDA receptor antibodies following HSV encephalitis, typically 1-7 weeks after the initial episode. This presents as:
- Relapse of symptoms (behavioral changes, movement disorders, seizures in children; delirium in adults)
- Worsening MRI findings
- Positive CSF/serum NMDA-receptor antibodies
Treatment: High-dose corticosteroids (methylprednisolone 1 g IV daily x 5 days), IVIG, or plasma exchange. Crucially, the presence of NMDA receptor antibodies should not lead to stopping acyclovir - always complete HSV treatment first.
- Goldman-Cecil Medicine, p.3306
- Adams and Victor's Principles of Neurology 12e, p.457
7. Relapses After Acyclovir
Relapse is rare in adults but more common in children. The most common cause is inadequate dose or insufficient duration. A second course of acyclovir is usually successful.
8. Acyclovir Side Effects to Monitor
| Side Effect | Notes |
|---|---|
| Renal dysfunction (transient) | Most important - ensure adequate hydration during infusion |
| Local vein irritation / phlebitis | Common with peripheral IV |
| Elevated hepatic enzymes (mild) | Usually transient |
| Nausea, vomiting, tremor | Uncommon |
| Encephalopathy | Rare; difficult to distinguish from the encephalitis itself |
- Adams and Victor's Principles of Neurology 12e, p.451
Prognosis
With prompt IV acyclovir, mortality has fallen from ~70% to ~10%. However, outcomes remain poor overall:
-
Less than 20% return to work
-
~50% are classified as moderately to severely disabled
-
Early treatment (before coma) is the strongest predictor of a good outcome - the level of consciousness at initiation of treatment is critical
-
Goldman-Cecil Medicine, p.3304
How do we manage the vancomycin and ceftrixone resistance in the bacterial meningities and what about the treatment
Finding Sources
Finding Sources
Searching PubMed
"bacterial meningitis" AND "antibiotic resistance" AND treatment
Searching the Web
vancomycin ceftriaxone resistant pneumococcal meningitis management treatment options 2024
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple major textbooks and current guidelines. Here is the full answer:
Bacterial Meningitis: Management of Vancomycin + Ceftriaxone Resistance
Understanding the Problem
The key organism driving vancomycin + ceftriaxone resistance concerns is drug-resistant Streptococcus pneumoniae (DRSP). Resistance mechanisms include:
- Penicillin/cephalosporin resistance: alteration of penicillin-binding proteins (PBPs) by transformation and horizontal DNA transfer from related streptococci. Altered PBPs have lower affinity for beta-lactams, causing resistance ranging from intermediate to high level.
- Vancomycin penetration problem: even when S. pneumoniae is "susceptible" to vancomycin in vitro, dexamethasone (used adjunctively) reduces blood-brain barrier inflammation and thereby reduces CSF vancomycin penetration, potentially creating a pharmacokinetic failure even with a susceptible organism.
MIC breakpoints for meningitis (stricter than non-meningitis):
-
Penicillin susceptible: MIC ≤0.06 μg/mL; resistant: ≥0.12 μg/mL
-
Ceftriaxone/cefotaxime: MIC ≥1.0 μg/mL = high-level resistance
-
Harrison's Principles of Internal Medicine 22E, p.1713
Step 1: Empirical Therapy (Before Culture/Sensitivities)
In all community-acquired bacterial meningitis in areas with DRSP prevalence >2%, start:
| Drug | Adult Dose | Purpose |
|---|---|---|
| Ceftriaxone | 2 g IV every 12 h | Covers susceptible pneumococcus, N. meningitidis, H. influenzae |
| OR Cefotaxime | 2-3 g IV every 6-8 h | Alternative cephalosporin |
| + Vancomycin | 15-20 mg/kg IV every 8 h (adults: 30-60 mg/kg/day) | Covers cephalosporin-resistant pneumococcus |
| + Dexamethasone | 0.15 mg/kg IV every 6 h x 4 days | Given before or with first antibiotic dose |
| + Acyclovir | 10 mg/kg every 8 h | Covers HSV encephalitis (leading differential) |
| + Ampicillin (if age >50 or immunocompromised) | 2 g IV every 4 h | Covers Listeria monocytogenes |
Do NOT reduce antibiotic doses as the patient improves - normalisation of the blood-brain barrier during recovery reduces achievable CSF levels.
- Harrison's Principles of Internal Medicine 22E, p.1762
- Rosen's Emergency Medicine, p.4407
Step 2: Targeted Therapy by Susceptibility Results
Once culture and MIC data return, tailor treatment as follows:
For S. pneumoniae:
| Susceptibility Pattern | Recommended Therapy | Alternative |
|---|---|---|
| Penicillin MIC ≤0.06 μg/mL (susceptible) | Penicillin G or Ampicillin | Ceftriaxone, cefotaxime, chloramphenicol |
| Penicillin MIC ≥0.12 μg/mL but ceftriaxone MIC ≤1.0 μg/mL | Ceftriaxone or Cefotaxime alone | Cefepime, meropenem |
| Ceftriaxone MIC ≥1.0 μg/mL (high-level resistance) | Vancomycin + Ceftriaxone/Cefotaxime | Vancomycin + moxifloxacin |
| Resistant to BOTH cephalosporins AND vancomycin, or cephalosporin allergy | Vancomycin + Rifampicin | Linezolid + vancomycin; moxifloxacin + vancomycin; chloramphenicol |
- Goldman-Cecil Medicine, Table 381-6
- Rosen's Emergency Medicine, p.4411
Step 3: When Vancomycin + Ceftriaxone Fails - The Real Resistance Scenario
When both vancomycin AND ceftriaxone fail (true dual resistance or pharmacokinetic failure from dexamethasone), the options are:
A. Add or Switch to Rifampicin
- Rifampicin (rifampin) penetrates the CSF excellently (unlike most antibiotics, it crosses even the uninflamed blood-brain barrier)
- Used as combination therapy - never monotherapy (rapid resistance emerges)
- Dose: 600 mg IV/PO every 24 h (up to 900 mg/day; 15 mg/kg/day in children)
- Combination: Vancomycin + Rifampicin is the standard salvage regimen for highly resistant pneumococcus
- Particularly important when dexamethasone is being used (rifampicin compensates for reduced vancomycin CSF levels)
B. Meropenem
- Carbapenem with excellent activity against penicillin-resistant S. pneumoniae, L. monocytogenes, H. influenzae, P. aeruginosa
- As effective as cefotaxime for pneumococcal, meningococcal, and H. influenzae meningitis
- Preferred over ceftriaxone for nosocomial/post-neurosurgical meningitis and for P. aeruginosa coverage
- Experimental data: meropenem was inferior to vancomycin but comparable to ceftriaxone in clearing pneumococcal CSF cultures
- Dose: 2 g IV every 8 h
C. Linezolid
- Dose: 600 mg IV every 12 h
- Used for cephalosporin-resistant pneumococcus in combination with vancomycin
- Also effective for MRSA meningitis (nosocomial/post-neurosurgical cases)
- Advantage: excellent CNS penetration; useful when beta-lactam allergy and vancomycin is needed
D. Moxifloxacin / Fluoroquinolones
- Moxifloxacin 400 mg IV/PO once daily
- Used with vancomycin for cephalosporin-resistant strains
- Levofloxacin is an alternative
- Caution: increasing fluoroquinolone resistance in some regions
E. Chloramphenicol
-
Historical alternative; still useful in resource-limited settings or severe beta-lactam allergy
-
Good CNS penetration
-
Limitations: bacteriostatic (not bactericidal for pneumococcus at achievable CSF concentrations), bone marrow toxicity
-
Goldman-Cecil Medicine, p.1916-1917
-
Rosen's Emergency Medicine, p.4407-4411
-
Adams and Victor's Principles of Neurology 12e, p.1881
Step 4: Pathogen-Specific Resistance Situations
N. meningitidis (Meningococcus)
- In the US, remains highly susceptible to penicillin and ampicillin
- Penicillin G or ampicillin is definitive therapy for susceptible strains
- Third-generation cephalosporins are used empirically and are effective
H. influenzae
- ~30% of isolates produce beta-lactamase (resistant to ampicillin/penicillin)
- Nearly all remain sensitive to third-generation cephalosporins
- For beta-lactamase-negative strains: ampicillin
- For resistant strains: ceftriaxone/cefotaxime (first-line), alternatives = chloramphenicol, cefepime, meropenem, fluoroquinolone, aztreonam
Nosocomial / Post-Neurosurgical Meningitis (MRSA, Coagulase-negative Staph, P. aeruginosa)
- Empirical: Vancomycin + Cefepime or Ceftazidime or Meropenem
- If beta-lactam contraindicated: linezolid (gram-positive) + aztreonam or ciprofloxacin (gram-negative coverage)
Listeria monocytogenes (cell-mediated immunity deficiency)
- Ampicillin ± gentamicin
- Trimethoprim-sulfamethoxazole if penicillin-allergic
- Cephalosporins have NO activity against Listeria - a critical point
- Stop dexamethasone if Listeria is confirmed (increased adverse outcomes shown in a prospective study)
The Dexamethasone Dilemma
Dexamethasone reduces mortality and hearing loss in pneumococcal/H. influenzae meningitis, but it reduces blood-brain barrier inflammation - which paradoxically decreases vancomycin CSF penetration.
Practical implications:
-
If using dexamethasone + vancomycin: consider adding rifampicin to ensure adequate CSF levels against resistant pneumococcus
-
Discontinue dexamethasone if: organism is not S. pneumoniae or H. influenzae, or if Listeria is confirmed
-
Dexamethasone benefit is only demonstrated in high-income countries - not shown in low-income settings
-
Goldman-Cecil Medicine, p.1915
Key Principles of Antibiotic Use in Meningitis
- IV route throughout - do not switch to oral; do not reduce doses as patient improves (BBB recovery reduces CSF levels)
- CSF bactericidal levels should be 10-20x the minimal bactericidal concentration (MBC)
- Rifampicin and chloramphenicol are the exceptions - they cross the uninflamed BBB; others require inflamed meninges for adequate penetration
- Culture and sensitivity-guided de-escalation is mandatory - vancomycin should be stopped once susceptibility data allow
- Antibiotic duration after organism identification: S. pneumoniae 10-14 days; N. meningitidis 7 days; H. influenzae 7 days; L. monocytogenes 21 days; gram-negative bacilli 21 days
- Goldman-Cecil Medicine, p.1902
This is a shared conversation. Sign in to Orris to start your own chat.