Help me build concepts of corticospinal tract
Reading File
Finding Sources
Finding Sources
Searching Images
corticospinal tract anatomy pathway diagram
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive textbook content and diagrams. Let me compose a thorough, well-structured answer.
Corticospinal Tract — Complete Conceptual Guide
1. Overview and Clinical Importance
The corticospinal tract (CST) — specifically its lateral division — is the most clinically important descending motor pathway in the human nervous system. It controls voluntary movement of the extremities, and lesions at any point along its course produce characteristic deficits that allow precise neurological localization.
"The corticospinal tract is sometimes referred to as the pyramidal tract" — though technically imprecise, since the medullary pyramids also contain reticulospinal and other fibres. — Neuroanatomy through Clinical Cases, 3e, p. 256
2. Cortical Origin (Upper Motor Neurons)
The CST fibres arise from pyramidal neurons in cortical layer V across multiple cortical areas:
| Cortical Area | Brodmann Area | Contribution |
|---|---|---|
| Primary motor cortex (M1), precentral gyrus | Area 4 | ~30–31% |
| Premotor cortex + Supplementary motor area | Area 6 | ~29–30% |
| Primary somatosensory + parietal cortex | Areas 3,1,2, 5, 7 | ~40% |
Key neurons:
- Most corticospinal neurons are ordinary layer V pyramidal cells
- ~3% are Betz cells — the largest neurons in the human nervous system (~60 µm diameter), found only in M1; their large axons (~16 µm diameter) conduct at ~70 m/s
- Total fibres per tract: >1 million
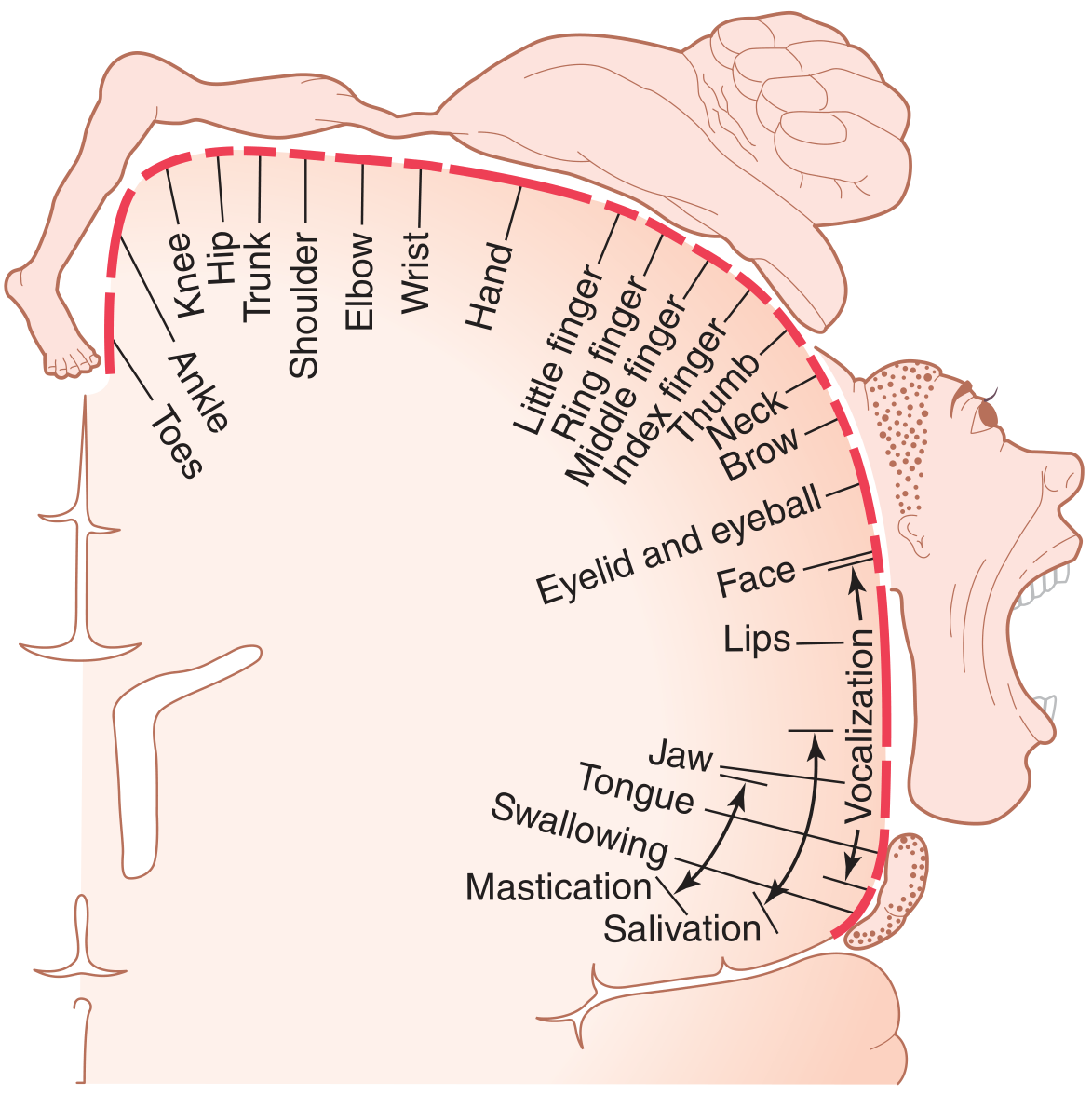
Somatotopy (motor homunculus):
- Face/mouth → near sylvian fissure (lateral)
- Hand/arm → midportion (disproportionately large — over half the primary motor cortex!)
- Trunk → near apex
- Leg/foot → dips into the interhemispheric (longitudinal) fissure (medial)
— Guyton & Hall Textbook of Medical Physiology, p. 687–689
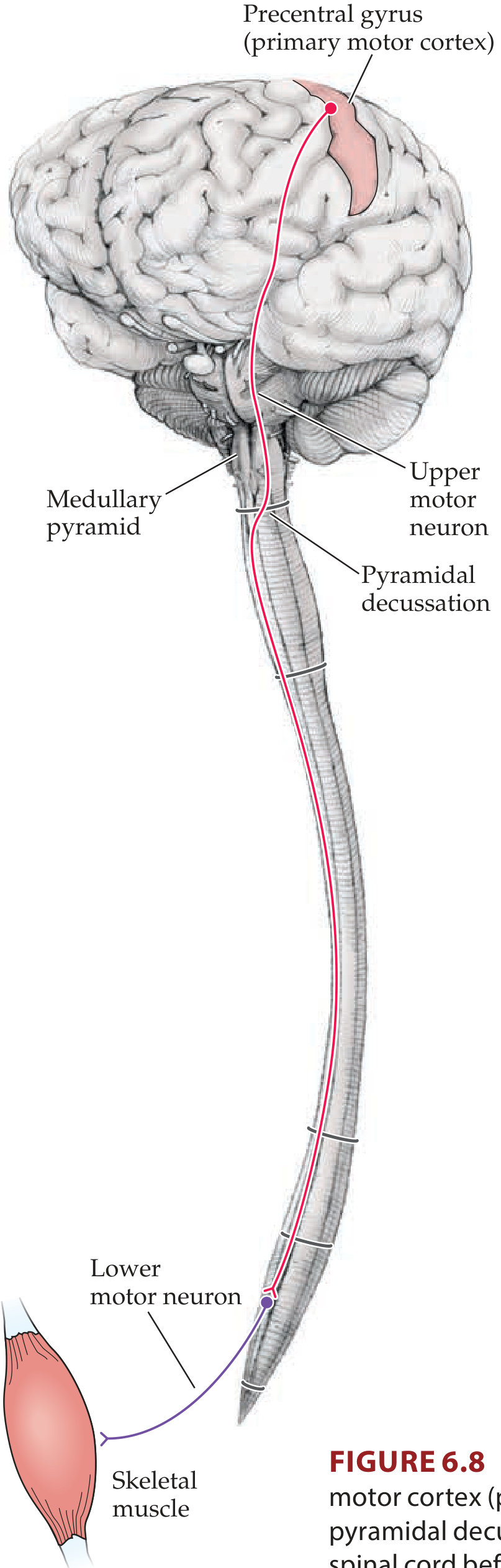
3. Course of the Tract — Step by Step
A. Corona Radiata
Axons leave cortex and enter the cerebral white matter (corona radiata) — a fan-shaped arrangement of fibres converging toward the internal capsule.
B. Internal Capsule
The fibres condense into the posterior limb of the internal capsule (between the caudate nucleus/putamen and the thalamus).
- Corticobulbar fibres (heading to cranial nerve nuclei) pass through the genu
- Corticospinal fibres (heading to spinal cord) pass through the posterior limb
C. Cerebral Peduncles (Midbrain)
The tract runs through the basis pedunculi (ventral midbrain). The middle three-fifths carry corticospinal fibres; medial fibres carry corticobulbar projections.
D. Basilar Pons
Fibres are scattered among transverse pontine fibres and pontine nuclei as they descend.
E. Medullary Pyramids
The fibres re-converge to form the pyramids on the ventral surface of the medulla — two prominent bulges visible from below.
F. Pyramidal Decussation (Caudal Medulla)
At the junction of the medulla and spinal cord, ~85–90% of fibres cross (decussate) in an interdigitated manner → forming the lateral corticospinal tract (LCST) in the contralateral dorsolateral funiculus.
The remaining 10–15% do not cross → continue ipsilaterally as the anterior (ventral) corticospinal tract (ACST) in the ventral funiculus.
— Localization in Clinical Neurology, 8e, p. 246–247
4. The Two Divisions in the Spinal Cord
| Feature | Lateral CST | Anterior CST |
|---|---|---|
| Location | Dorsolateral funiculus | Ventral funiculus |
| Side | Contralateral to origin | Ipsilateral (crosses later in ventral white commissure) |
| % of fibres | ~85–90% | ~10–15% |
| Termination | Laminae IV–IX, all cord levels | Lamina III, cervical + upper thoracic only |
| Function | Skilled limb/digit movements (distal) | Bilateral postural & axial movements (proximal) |
The ACST fibres eventually cross in the ventral white commissure at cervical/upper thoracic levels before synapsing.
5. Synaptic Targets in the Spinal Cord
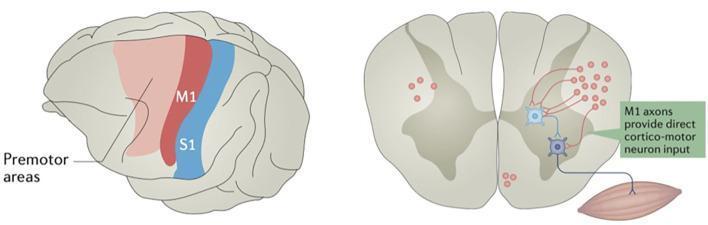
LCST fibres synapse on:
- Spinal interneurons (most common — indirect route, coordinates muscle groups)
- α-motor neurons in the ventral horn directly (monosynaptic; especially important for fine distal movements — fingers, toes)
- A few fibres reach sensory relay neurons in the dorsal horn (modulate sensory input)
Somatotopic organization in ventral horn (lamina IX):
- Axial musculature → extreme ventromedial sector
- Limb-girdle muscles → intermediate
- Intrinsic limb/distal muscles → dorsolateral sector
— Localization in Clinical Neurology, 8e, p. 247; Ganong's Review of Medical Physiology, 26e, p. 245
6. Upper Motor Neuron vs. Lower Motor Neuron Lesions
This is the most clinically critical concept derived from CST anatomy:
| Feature | UMN Lesion (CST damage) | LMN Lesion |
|---|---|---|
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Hyperreflexia | Hyporeflexia / areflexia |
| Weakness | Yes | Yes |
| Atrophy | Mild (disuse) | Severe (denervation) |
| Fasciculations | Absent | Present |
| Babinski sign | Present (extensor plantar) | Absent |
| Hoffmann sign | May be present | Absent |
Important nuance: With acute UMN lesions (e.g., acute stroke, acute SCI), patients initially show flaccid paralysis + hyporeflexia (spinal shock), which gradually converts to spasticity over hours to months.
Spasticity in UMN lesions is thought to arise not from corticospinal damage per se, but from loss of descending inhibitory pathways travelling alongside the CST (reticulospinal), leading to disinhibited anterior horn motor neuron excitability.
— Neuroanatomy through Clinical Cases, 3e, p. 261; Ganong's Review of Medical Physiology, 26e, p. 246
7. Topographic Localization — Where is the Lesion?
| Level of Lesion | Deficit Pattern |
|---|---|
| Motor cortex | Contralateral weakness; often focal (monoparesis, face-arm > leg if lateral cortex) |
| Internal capsule | Dense contralateral hemiplegia (face + arm + leg equally affected — fibres packed together) |
| Brainstem | Crossed syndromes: ipsilateral cranial nerve palsy + contralateral hemiplegia (e.g., Weber syndrome in midbrain) |
| Above pyramidal decussation | Contralateral weakness |
| Below pyramidal decussation (spinal cord) | Ipsilateral weakness (LCST already crossed) |
| Anterior CST lesion | Ipsilateral proximal weakness (axial) |
8. Corticobulbar Tract — The "Head and Neck CST"
The corticobulbar tract runs with the CST but diverges at the brainstem to control cranial nerve motor nuclei (V, VII, IX, X, XI, XII). Key points:
- Most cranial nerve nuclei receive bilateral cortical input → unilateral UMN lesions rarely cause lasting cranial nerve palsy
- Exception: Lower facial motor neurons (CN VII) receive predominantly contralateral input → unilateral hemispheric lesion causes contralateral lower face weakness while sparing forehead (bilateral innervation of forehead)
- Exception: Hypoglossal nucleus (CN XII) — predominantly contralateral → tongue deviates toward weak side (toward lesion side) in UMN lesions
9. Summary — The 3-Neuron Concept
UPPER MOTOR NEURON (UMN)
Layer V, Motor Cortex (Area 4, 6, 3,1,2)
↓ (Corona Radiata)
↓ (Posterior limb, Internal Capsule)
↓ (Cerebral Peduncle, Basilar Pons)
↓ (Medullary Pyramid)
↓ PYRAMIDAL DECUSSATION (caudal medulla)
↙ 85–90% ↘ 10–15%
Lateral CST Anterior CST
(contralateral cord) (ipsilateral cord)
↓ ↓ (crosses in ventral commissure)
LOWER MOTOR NEURON (LMN)
α-motor neuron, Anterior Horn (Lamina IX)
↓
Skeletal Muscle
10. Key Numbers to Remember
| Fact | Value |
|---|---|
| Total CST fibres (each side) | >1,000,000 |
| Betz cells | ~34,000 per tract (3%) |
| Betz cell axon diameter | ~16 µm |
| Betz cell conduction velocity | ~70 m/s |
| Fibres crossing at decussation | ~85–90% |
| Contribution from M1 (area 4) | ~30–31% |
| Contribution from parietal/sensory cortex | ~40% |
Sources:
- Neuroanatomy through Clinical Cases, 3e (Blumenfeld), pp. 255–263
- Guyton & Hall Textbook of Medical Physiology, pp. 687–691
- Ganong's Review of Medical Physiology, 26e, pp. 244–246
- Localization in Clinical Neurology, 8e, pp. 246–248
This is a shared conversation. Sign in to Orris to start your own chat.