Teach albinism
Reading File
Finding Sources
Finding Sources
Searching PubMed
albinism
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need for a comprehensive teaching session on albinism. Let me compile the full answer.
Albinism - A Comprehensive Teaching Guide
1. Definition
Albinism is a genetically heterogeneous group of disorders of melanin synthesis characterized by a reduction or complete absence of melanin pigment in the skin, hair, and/or eyes. The core defect lies in melanocyte function - the cells are present in normal numbers but fail to produce adequate melanin.
- Kanski's Clinical Ophthalmology, 10th ed.
- Andrews' Diseases of the Skin
2. Biochemical Basis
The fundamental pathway involves the amino acid tyrosine:
Tyrosine →(Tyrosinase)→ DOPA →(Tyrosinase)→ Dopaquinone → Melanin
Tyrosinase is a copper-containing enzyme that catalyzes the first two steps. Any mutation disrupting this enzyme, its processing, or the melanosomal machinery where it operates leads to albinism. Melanin normally pigments skin, hair, the iris, retinal pigment epithelium (RPE), and the choroid.
- Lippincott Biochemistry, 8th ed.
3. Classification
Albinism is classified into two broad categories:
A. Oculocutaneous Albinism (OCA)
Eyes, skin, AND hair all affected. Autosomal recessive. Seven recognized subtypes:
| Type | Gene | Key Features |
|---|---|---|
| OCA1A | TYR (chromosome 11q14) | Complete absence of tyrosinase activity; white hair/skin throughout life; VA ~20/400; most severe |
| OCA1B | TYR | Reduced (not absent) tyrosinase; pigment may develop after age 1-3 years; can tan; "yellow mutant" albinism |
| OCA2 | OCA2 / P-gene (chromosome 15q12) | Most common globally (~50% of OCA); formerly "tyrosinase-positive"; broad phenotype; prevalent in Africa (1:4,000); associated with Prader-Willi/Angelman deletions |
| OCA3 | TYRP1 (chromosome 9p23) | "Rufous" or red OCA; seen especially in Black Africans; reddish-brown skin and red hair; mild visual defects |
| OCA4 | SLC45A2 / MATP | Phenotypically similar to OCA2; variable hypopigmentation; common in East Asia |
| OCA5 | 4q24 locus | Rare; described in a Pakistani family; golden hair, white skin |
| OCA6 | SLC24A5 | Diverse ethnicities; hair ranges from white to dark brown |
| OCA7 | C10orf11 | Rare; leucine-rich repeat protein |
B. Ocular Albinism (OA)
Eyes only affected. Skin and hair pigmentation is near-normal or only mildly reduced.
- OA1 (X-linked): Most common form of ocular albinism. Gene: GPR143 (chromosome Xp22.2). GPR143 encodes a G-protein-coupled receptor involved in melanosome biogenesis. Melanosomes are decreased in number but enlarged in size (macromelanosomes visible on electron microscopy). Prevalence: ~1:50,000-60,000.
Note: Because OA is X-linked, it primarily affects males. Female carriers show a mosaic "mud-splattered" appearance of the retinal pigment epithelium.
4. Ocular Findings (Core Pathology)
This is the clinically significant part of albinism. ALL forms - OCA and OA - share the same ocular phenotype because melanin is required for normal eye development:
Visual Acuity
- Reduced VA is universal, typically 20/100 to 20/400 in OCA1A
- Caused by foveal hypoplasia - the foveal pit fails to develop (requires melanin during embryogenesis)
- The macula shows absent perimacular vascular arcades
Nystagmus
- Pendular and horizontal
- Worsens in bright illumination
- Tends to lessen with age
Iris Translucency / "Pink Eye"
- The iris lacks melanin and is diaphanous
- Light passes straight through, giving the characteristic pink-red iris color (from the underlying blood vessels and choroidal circulation)

Figure: Patient with OCA showing white eyebrows/lashes and characteristic red irises - Lippincott Biochemistry
Fundus Appearance
- Severely hypopigmented fundus with prominent choroidal vessels visible through the RPE
- Foveal aplasia or hypoplasia
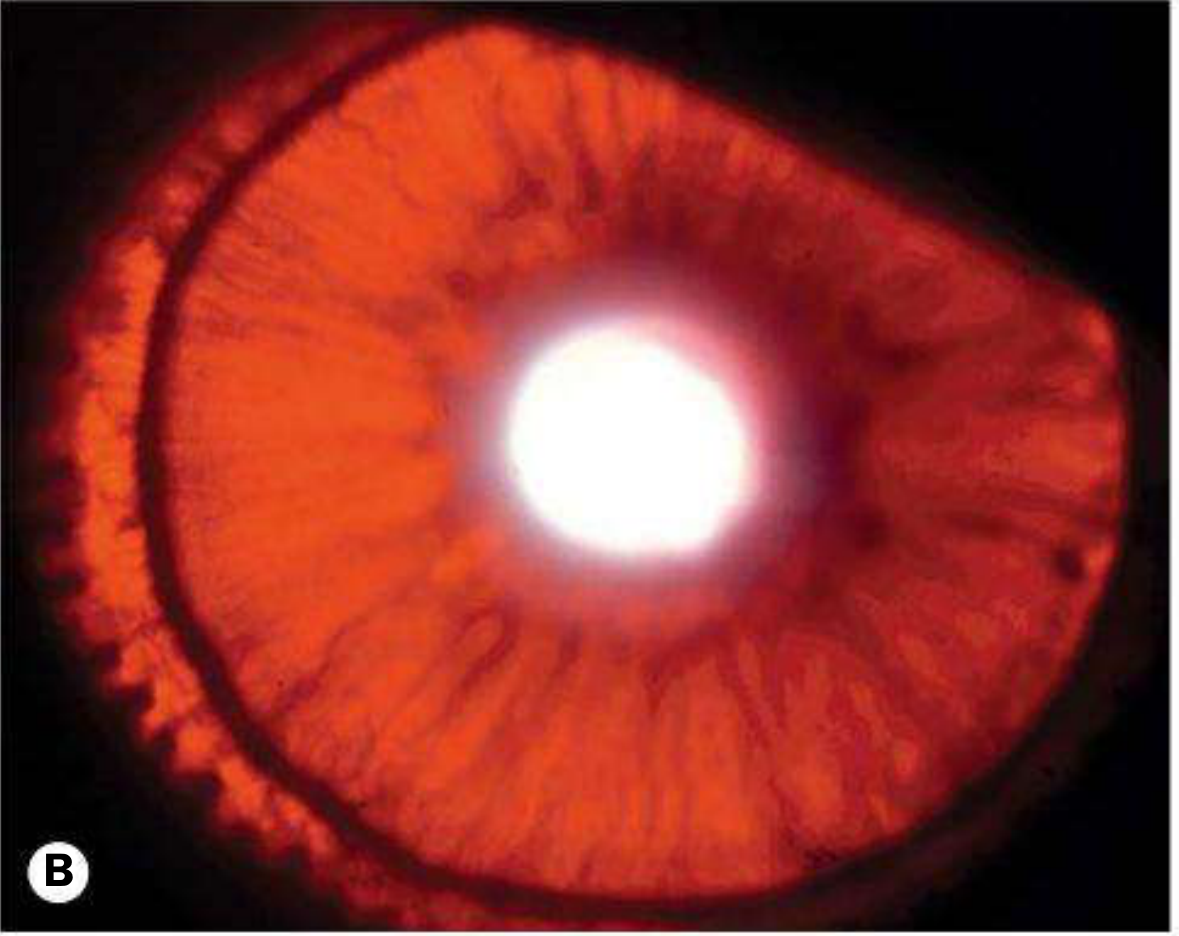
Figure: Marked iris translucency in OCA1 - Kanski's Clinical Ophthalmology
Optic Chiasm Misrouting
- Normally, about 60% of optic nerve fibers cross at the chiasm (nasal fibers)
- In albinism, an abnormally high proportion of fibers cross (sometimes >90%)
- This results in reduced uncrossed fibers and abnormal visual evoked potentials (VEP) with crossed asymmetry
- Clinically produces: strabismus, reduced stereoscopic vision, absence of normal binocular responses
Other Ocular Features
- High refractive errors (various types)
- Positive angle kappa
- Absent stereopsis
- Photophobia
5. Syndromic Forms (Albinism + Systemic Disease)
Some rare syndromes combine albinism with serious systemic features:
Hermansky-Pudlak Syndrome (HPS)
- Autosomal recessive
- Lysosomal storage disease affecting the biogenesis of lysosome-related organelles
- Triad: OCA + platelet dysfunction (bleeding) + ceroid lipofuscin storage
- Complications: pulmonary fibrosis (major cause of death), granulomatous colitis
- Multiple subtypes (HPS1-11); HPS1 common in Puerto Ricans and Japanese
Chediak-Higashi Syndrome
- Autosomal recessive; mutation in LYST (lysosomal trafficking regulator)
- Failure of phagolysosome formation
- Triad: OCA + recurrent pyogenic infections (especially Staphylococcus) + peripheral neuropathy
- Neutrophils have giant granules visible on blood smear
- Risk of accelerated hemophagocytic lymphohistiocytosis (HLH) phase
Waardenburg Syndrome
- Autosomal dominant
- PAX3, MITF, EDN3 gene mutations
- Features: white forelock, poliosis, synophrys ("monobrow"), sensorineural deafness, sometimes heterochromia irides
6. Genetics Summary
| Feature | OCA | OA1 |
|---|---|---|
| Inheritance | Autosomal recessive | X-linked recessive |
| Primary defect | Tyrosinase pathway / melanosome proteins | GPR143 melanosome receptor |
| Skin + hair | Hypopigmented to normal | Normal to mildly diluted |
| Eyes | Severely affected | Severely affected |
| Melanocyte number | Normal | Normal |
| Melanosome size | Normal | Enlarged (macromelanosomes) |
7. Clinical Consequences and Complications
Skin Cancer Risk
- All OCA patients lack UV-protective melanin
- Greatly increased risk of squamous cell carcinoma (SCC) and basal cell carcinoma (BCC)
- Melanoma risk also elevated but harder to detect clinically
- Dermoscopy is challenging due to lack of pigment; reflectance confocal microscopy may help
Visual Disability
- Most significant functional impairment
- Low vision aids, tinted lenses, and contact lenses can reduce photophobia
8. Management
Ophthalmological
- Regular ophthalmology review - early referral is critical
- Refractive correction (spectacles/contact lenses)
- Tinted lenses / sunglasses to reduce photophobia
- VA is often stable through life and may improve slightly into adulthood (especially OCA1B, OCA2)
- Strabismus surgery considered on case-by-case basis
Dermatological
- Sun protection is the cornerstone: broad-spectrum sunscreen, protective clothing, sun avoidance
- Annual skin examination for premalignant/malignant lesions
- Vitamin D supplementation - required because sun avoidance limits cutaneous synthesis
Genetic Counseling
- Genetic testing available for TYR, OCA2, TYRP1, SLC45A2, GPR143 and other loci
- Carrier testing and prenatal diagnosis possible
- Molecular genetics now allows precise subtyping (OCA1-7)
9. Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Piebaldism | Patchy depigmentation (not global); white forelock; normal eyes |
| Vitiligo | Acquired; patchy; normal eyes; autoimmune |
| Phenylketonuria (PKU) | Hypopigmentation + intellectual disability + elevated phenylalanine; no eye misrouting |
| Prader-Willi / Angelman | May have OCA2 gene deletion causing hypopigmentation; neurological features dominate |
| Ocular albinism carriers | Mosaic RPE "mud-splattered" fundus; normal systemic pigmentation |
10. Key Mnemonics
"FONS" = Fundus hypopigmentation, Optic chiasm misrouting, Nystagmus, Strabismus - the four cardinal ocular signs of albinism.
OCA types by gene: TYR (1), P-gene/OCA2 (2), TYRP1 (3), MATP/SLC45A2 (4), SLC24A5 (6) - "TPTMS"
Sources
- Kanski's Clinical Ophthalmology, 10th edition - pp. 662-664
- Andrews' Diseases of the Skin (Clinical Dermatology) - Chapter 36
- Lippincott Illustrated Reviews: Biochemistry, 8th ed. - p. 769
- Emery's Elements of Medical Genetics and Genomics
- Fitzpatrick's Dermatology, Volumes 1-2
- The Developing Human (Clinically Oriented Embryology)
This is a shared conversation. Sign in to Orris to start your own chat.