Hyperurecemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hyperuricemia"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the material needed for a comprehensive answer. Let me compile the full response.
Hyperuricemia
Definition
Hyperuricemia is defined as a serum urate concentration exceeding its solubility threshold at normal pH and body temperature - generally > 6.8 mg/dL. It is the necessary precondition for gout but is not itself sufficient to cause it. The treatment target for urate-lowering therapy is < 6 mg/dL (or < 5 mg/dL in severe/tophaceous gout).
- Rheumatology, 2-Volume Set (2022, Elsevier), p. 1768
- Biochemistry, 8th ed - Lippincott Illustrated Reviews, p. 843
Why Humans Are Predisposed
Three species-wide "conditioning factors" make all humans vulnerable to hyperuricemia:
- Absence of uricase - humans lost this enzyme ~18 million years ago. Other mammals convert uric acid to the far more soluble allantoin; humans cannot.
- Net renal reabsorption of ~90% of filtered urate - via the proximal tubule URAT1 transporter and the "transportasome."
- Limited solubility of urate and monosodium urate (MSU) in body fluids.
Despite this, most people maintain urate below the saturation threshold. Hyperuricemia emerges when production or excretion falls out of balance.
- Goldman-Cecil Medicine, p. 172; Rheumatology, 2-Volume Set, p. 1767
Classification / Causes
Hyperuricemia is broadly classified as primary (idiopathic) or secondary (identifiable cause), and by mechanism as underexcretion or overproduction.
| Mechanism | Proportion | Key Examples |
|---|---|---|
| Renal underexcretion | > 90% of gout cases | Reduced GFR, hypertension, obesity, lead nephropathy |
| Overproduction | < 10% | Myeloproliferative diseases, tumor lysis, psoriasis, Lesch-Nyhan syndrome, PRPP synthetase overactivity, von Gierke disease |
| Mixed | Minority | Both mechanisms co-exist |
Drugs causing underexcretion:
- Thiazide diuretics
- Ethanol
- Low-dose salicylates (0.06-3.0 g/day)
- Cyclosporine, tacrolimus
- Levodopa
- Angiotensin II receptor blockers (some)
Secondary overproduction causes:
- Acute leukemias, lymphomas, tumor lysis syndrome
- Hemolytic states
- Psoriasis
- Chemotherapy/irradiation (high cell turnover)
The purine degradation pathway below illustrates how genetic defects lead to uric acid accumulation:
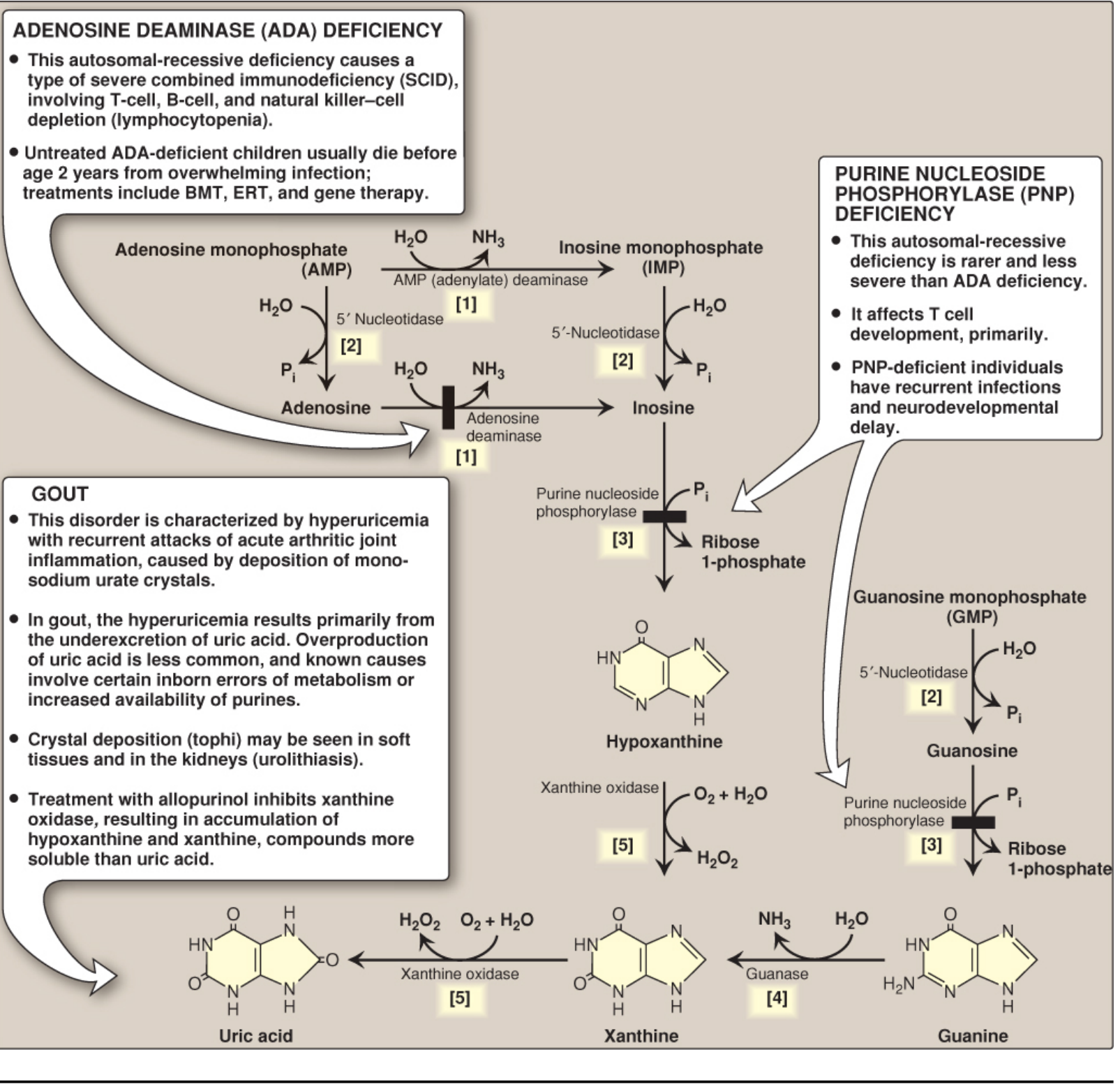
- Goldman-Cecil Medicine, p. 176-203; Lippincott Biochemistry 8th ed, p. 843-844
Pathophysiology of MSU Crystal Formation and Inflammation
When serum urate remains supersaturated, monosodium urate (MSU) crystals precipitate, particularly in:
- First metatarsophalangeal joint (podagra)
- Midfoot, Achilles tendon
- Periarticular soft tissues (tophi)
Crystal formation is promoted by: seed nuclei (cartilage debris, collagen), low temperature, low pH, dehydration, and elevated cation concentrations. Osteoarthritis co-localizes with MSU deposits, likely due to chondroitin sulfate lowering urate solubility.
Inflammatory cascade:
- MSU crystals are recognized by resident macrophages/monocytes in the synovium
- NLRP3 inflammasome is activated (two-signal system: toll-like receptor priming + MSU crystal assembly signal)
- Caspase-1 activated → cleavage and release of IL-1β and IL-18
- Massive neutrophil migration → acute gouty flare
- IL-1 antagonists (anakinra, canakinumab) have proven efficacy in both treating and preventing flares
- Rheumatology, 2-Volume Set, pp. 1768-1770

Asymptomatic Hyperuricemia
-
Not a disease by itself
-
Most patients with hyperuricemia never develop gout
-
Risk of acute gout increases with SU level: ~50% of patients with SU > 10 mg/dL develop clinical gout
-
Comorbidities: metabolic syndrome, obesity, dyslipidemia, hypertension, diabetes mellitus, CKD, heart failure
-
Using DECT and ultrasound, synovial microtophi are detectable even before the first clinical gout flare
-
Recent meta-analysis (2025): hyperuricemia is independently associated with metabolic syndrome (PMID 40068943) and increased risk of contrast-induced AKI (OR 1.68, 95% CI 1.38-2.04)
-
Rheumatology, 2-Volume Set, p. 1773
Clinical Consequences
| Stage | Features |
|---|---|
| Asymptomatic hyperuricemia | Elevated SU, no symptoms |
| Acute gout flare | Sudden severe joint pain, max inflammation in 12-24 h, erythema, warmth; classic podagra |
| Intercritical gout | Asymptomatic intervals between flares |
| Chronic tophaceous gout | Persistent joint disease, tophi in soft tissue, bone erosion |
| Uric acid nephrolithiasis | Urolithiasis; uric acid stones precipitate in acidic urine |
| Urate nephropathy | CKD, contrast-induced AKI risk |
Definitive diagnosis requires polarized light microscopy of synovial fluid to confirm needle-shaped, negatively birefringent MSU crystals.
Treatment
Acute Gout Flare
| Drug | Mechanism | Notes |
|---|---|---|
| NSAIDs (e.g., indomethacin) | COX inhibition, anti-inflammatory | Classic first-line; all NSAIDs likely effective |
| Colchicine | Binds tubulin → depolymerization → inhibits neutrophil migration; blocks NLRP3 | Must be given within 36 h of onset; no effect on uric acid levels |
| Corticosteroids | Anti-inflammatory | Intra-articular (1-2 joints) or systemic (polyarticular) |
| IL-1 antagonists (anakinra, canakinumab) | Block IL-1β | Refractory/contraindicated cases |
Urate-Lowering Therapy (ULT) - Chronic Management
Indications for ULT:
- ≥ 2 gouty attacks per year
- Tophi
- CKD or kidney stones
- Severe/refractory disease
Target: SU < 6 mg/dL (< 5 mg/dL in tophaceous/severe gout)
| Drug | Class | Mechanism | Notes |
|---|---|---|---|
| Allopurinol | Xanthine oxidase inhibitor (XOI) | Inhibits XO; oxidized to long-lived oxypurinol | First-line for most patients; start low, titrate; works in both over- and underexcretors |
| Febuxostat | Non-purine XOI | Selective inhibition of XO | Alternative if allopurinol not tolerated/insufficient; at least equally effective; renoprotective |
| Probenecid | Uricosuric | Blocks URAT1 in proximal tubule → increases uric acid excretion | For underexcretors intolerant to XOIs; not if urolithiasis |
| Pegloticase | Recombinant uricase (IV) | Converts urate → allantoin | Refractory severe tophaceous gout; every 2 weeks IV; monitor SU to prevent infusion reactions |
Key principle: Starting ULT can precipitate an acute flare due to rapid SU shifts - co-prescribe anti-inflammatory prophylaxis (low-dose colchicine or NSAIDs) for at least 6 months when initiating ULT. Patients on dialysis generally do not need ULT (dialysis removes uric acid efficiently).
- Lippincott Pharmacology, 7th ed, p. 1376-1377; Firestein & Kelley's Textbook of Rheumatology, p. 6119-6151; Goldman-Cecil Medicine, p. 592; Lippincott Biochemistry, 8th ed, p. 846
Dietary and Lifestyle Factors
- Increase risk: meat, shellfish, ethanol, sugary drinks (fructose drives PRPP synthesis), high-purine foods
- Decrease risk: low-fat dairy products
- Weight loss in obesity reduces SU and gout flare frequency
- Avoid thiazides where possible; consider losartan (uricosuric ARB) in hypertensive gout patients
Recent Evidence (2024-2026)
Recent meta-analyses confirm important associations:
- Hyperuricemia and metabolic syndrome show strong bidirectional correlation (Fan J et al., Am J Hypertens 2025, PMID 40068943)
- In type 2 diabetes, hyperuricemia and gout prevalence are significantly elevated (Gao L et al., Front Endocrinol 2026, PMID 42422434)
- Psoriasis/psoriatic arthritis carry increased risk of gout and hyperuricemia (Liu Z et al., Am J Med Sci 2025, PMID 39961457)
This is a shared conversation. Sign in to Orris to start your own chat.