What is Fistula in ano
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fistula in ano" classification treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Let me compile it.
Fistula-in-Ano (Anal Fistula)
Definition
A fistula-in-ano is a chronic abnormal communication extending from the anorectal lumen (the internal opening, almost always at the dentate line) to an external opening on the perianal skin or perineum. It is lined by granulation tissue and represents the chronic sequela of a perianal abscess that fails to heal completely.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Sabiston Textbook of Surgery
Aetiology / Pathogenesis
The cryptoglandular theory is the dominant explanation: 8-10 anal glands located at the dentate line open into the intersphincteric space. When their ducts become obstructed, bacteria cause suppuration that tracks along the path of least resistance, forming a perianal abscess. If the tract fails to heal after drainage, it epithelializes into a chronic fistula.
- Approximately 50% of perianal abscesses ultimately lead to fistula formation.
- Other causes include: Crohn's disease, tuberculosis, lymphogranuloma venereum, actinomycosis, rectal duplication, foreign body, malignancy (and rarely, carcinoma arising within a longstanding fistula).
- Current Surgical Therapy, 14th Ed.
Clinical Features
Symptoms:
- Chronic, intermittent purulent or bloody discharge from the external opening
- Cyclical pattern - pain and swelling followed by spontaneous drainage and relief
- History of a previous perianal abscess (surgical or spontaneous drainage)
- Passage of flatus or faeces through the external opening suggests a rectal (rather than anal) internal opening
Signs on examination:
- One or more chronic wounds / pyogenic granuloma at the perianal skin
- A palpable "cordlike" subcutaneous tract
- Bilateral external openings suggest involvement of the deep postanal space (horseshoe fistula)
- Multiple external openings ("watering-can perineum") raises suspicion for perianal Crohn's disease
- Sabiston Textbook of Surgery; Bailey and Love's
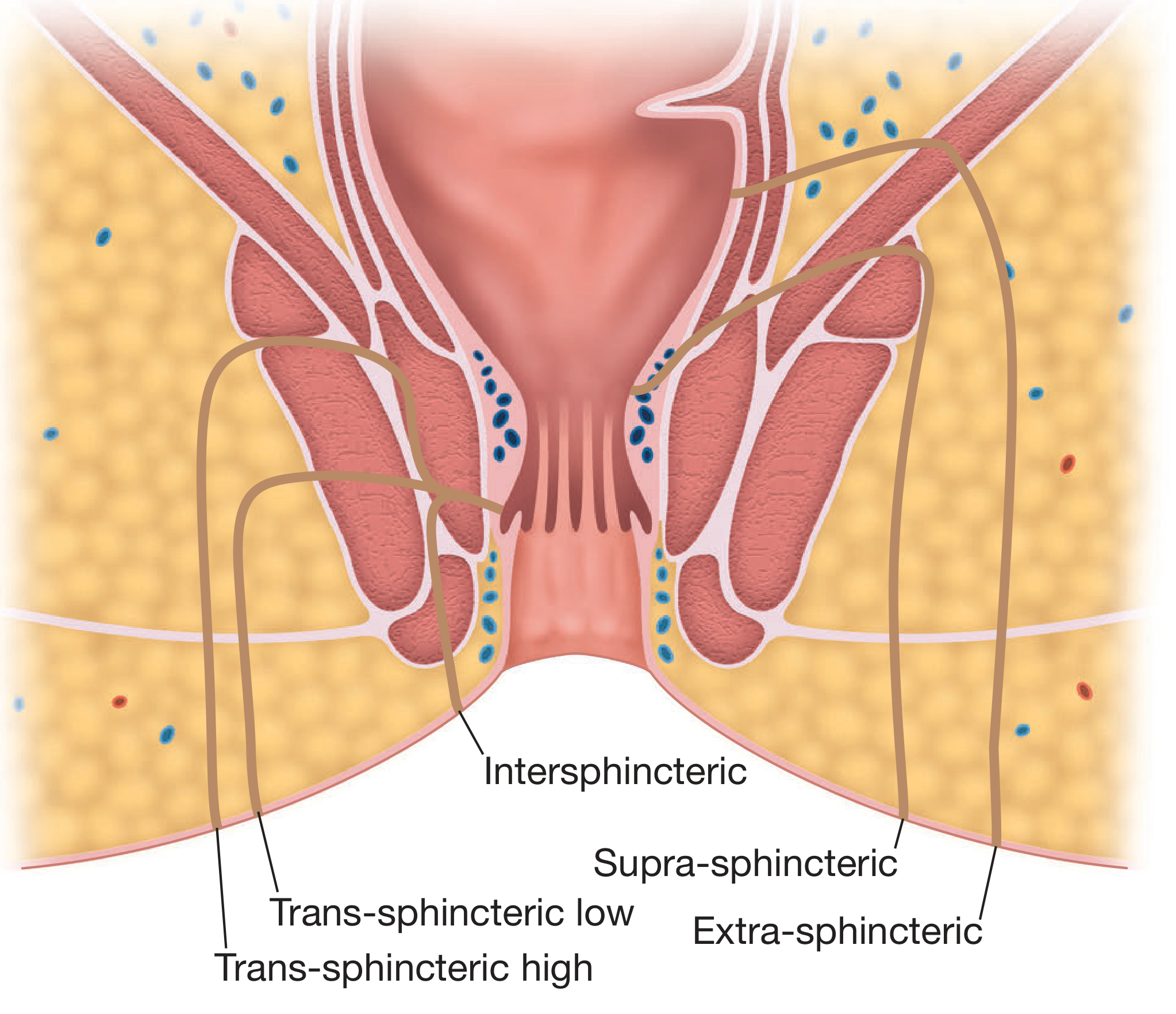
Parks' Classification
The most widely used system classifies fistulae by the relationship of the primary tract to the external anal sphincter:
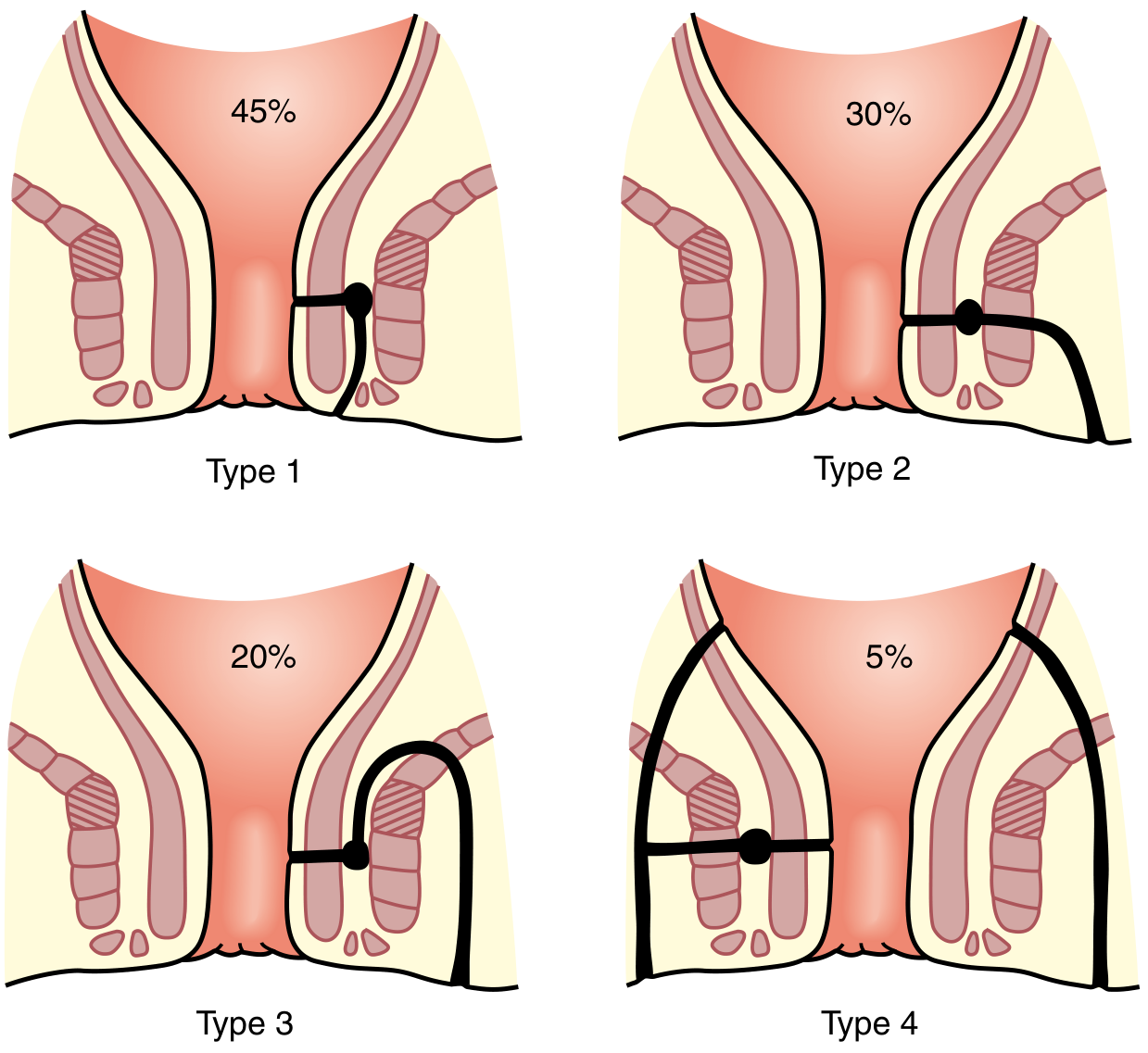
| Type | Description | Frequency |
|---|---|---|
| Type 1 - Intersphincteric | Tract stays within the intersphincteric plane and opens at the perianal skin | ~45% |
| Type 2 - Transsphincteric | Tract passes through the external sphincter into the ischiorectal fossa | ~30% |
| Type 3 - Suprasphincteric | Upward extension in the intersphincteric plane, loops over puborectalis and tracks down through the ischiorectal fossa | ~20% |
| Type 4 - Extrasphincteric | Tract passes from perineal skin through the ischiorectal fossa and levator ani into the rectal wall, bypassing the sphincters entirely | ~5% |
Also recognized: Superficial/subcutaneous fistulae that do not involve the sphincter complex at all.
- Sabiston Textbook of Surgery; Current Surgical Therapy, 14th Ed.
AGA Simple vs. Complex Classification
The American Gastroenterology Association condenses Parks' system for clinical decision-making:
| Category | Features |
|---|---|
| Simple | Low tract (superficial, low inter- or low transsphincteric); single external opening; no abscess; no risk factors |
| Complex | High tract; extra- or suprasphincteric; associated abscess; anovaginal fistula; anal stricture; Crohn's disease; prior incontinence; anterior fistula in women; radiation history; multiple openings |
- Bailey and Love's Short Practice of Surgery
Goodsall's Rule
This rule predicts the path of the fistula tract and the location of the internal opening:
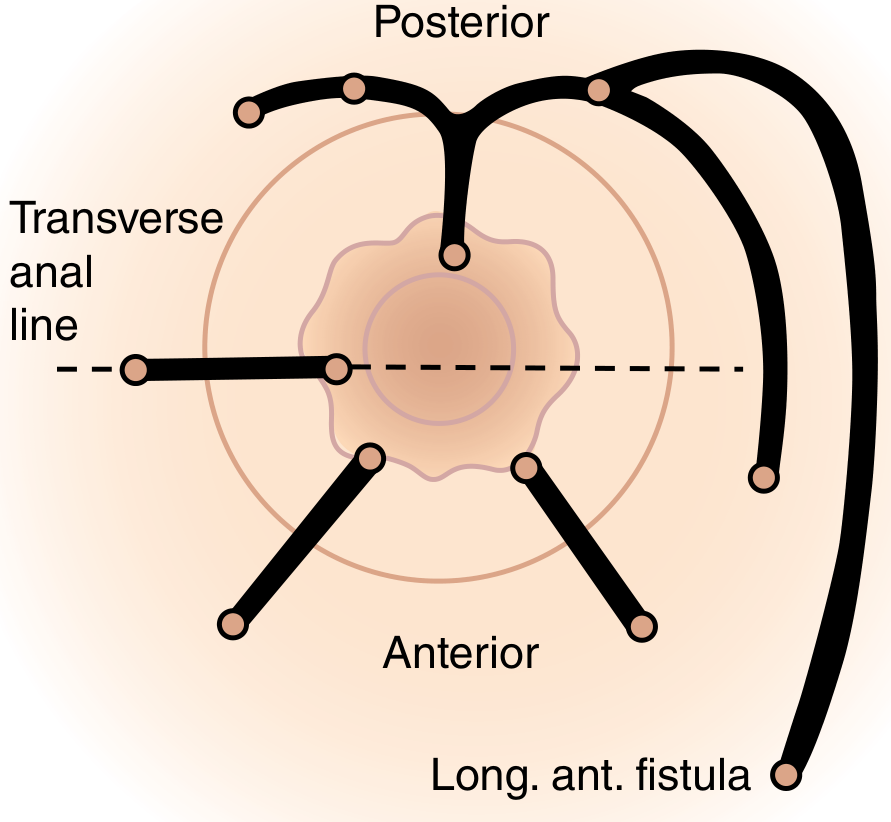
- Anterior external openings (anterior to the transverse anal line): tract runs radially in a straight line to the internal opening. Exception: an opening >3 cm from the anal verge may represent an anterior extension of a horseshoe fistula originating posteriorly.
- Posterior external openings (posterior to the transverse anal line): tract curves in a horseshoe fashion to a posterior midline internal opening.
- Sabiston Textbook of Surgery
Investigations
Clinical assessment:
- Digital rectal examination - may palpate the internal opening as a nodule/pit at the dentate line
- Anoscopy - direct visualization of the internal opening; gentle pressure over the tract may produce drainage from the offending crypt
- Fistula probe - gentle passage from external to internal opening in the operating room to define anatomy (care must be taken to avoid creating a false passage)
- Injection of hydrogen peroxide, methylene blue, or milk can help identify the internal opening
Imaging (for complex/recurrent cases):
- MRI with anal fistula protocol - best for defining tract anatomy relative to sphincters and levators; the reference standard for complex fistulae
- Endoanal ultrasound (EAUS) - useful for preoperative sphincter assessment; comparable accuracy to MRI
- Transperineal ultrasound - lower cost, less invasive alternative
- CT scan - inadequate resolution to define sphincter relationships; not recommended for fistula assessment
- Sabiston; Current Surgical Therapy
Treatment
The four guiding principles of fistula surgery are:
- Define fistula anatomy
- Ensure resolution of sepsis
- Assess and preserve anal sphincter function
- Minimize recurrence risk
Simple / Low Fistulae (intersphincteric or low transsphincteric involving <1/3 of external sphincter)
Fistulotomy (lay-open technique)
- The tract is unroofed and laid open to heal by secondary intention
- Clinically significant fecal incontinence occurs in <5% of patients with normal preoperative sphincter function
- Recurrence rate: 2%-8%
Complex / High Fistulae
Seton placement
- A silastic vessel loop or rubber band is passed through the tract
- Draining seton: controls sepsis, keeps the external opening patent, allows a narrow tract to form; prevents cyclical symptoms; a partial fistulotomy through soft tissue up to the external sphincter can be performed simultaneously
- Cutting seton: progressively tightened to slowly divide the sphincter in a controlled manner, allowing fibrosis to develop and prevent incontinence
Sphincter-preserving techniques (preferred for complex fistulae to avoid incontinence):
- Advancement flap - endorectal or anodermal flap used to close the internal opening; healing rates ~50-75%
- Ligation of Intersphincteric Fistula Tract (LIFT procedure) - the intersphincteric plane is dissected and the tract is ligated and divided; sphincter-sparing with reported healing rates of 40-80%
- Video-Assisted Anal Fistula Treatment (VAAFT) - endoscopic identification and closure of the internal opening with destruction of the epithelialized tract
- Fibrin glue / fistula plug - biological closure with lower success rates (~50%) but minimal risk of incontinence; may be repeated
- Laser fistula closure (FiLaC) - laser obliteration of the tract
Crohn's-associated fistulae require a separate approach including:
- Biological therapy (anti-TNF agents such as infliximab)
- Avoidance of aggressive surgery that risks incontinence or poor wound healing
- Long-term seton drainage as a bridge to biological therapy
- Sabiston Textbook of Surgery; Current Surgical Therapy, 14th Ed.; Bailey and Love's
Key Points Summary
| Feature | Detail |
|---|---|
| Internal opening | Almost always at the dentate line (cryptoglandular origin) |
| External opening | Perianal skin, perineum, rarely vagina |
| Most common types | Intersphincteric (45%) and transsphincteric (30%) |
| Most feared complication of surgery | Fecal incontinence |
| Investigation of choice (complex) | MRI with anal fistula protocol |
| Treatment for low fistula | Fistulotomy |
| Treatment for high/complex fistula | Seton + sphincter-preserving procedure |
| Red flag - multiple openings | Consider Crohn's disease or TB |
This is a shared conversation. Sign in to Orris to start your own chat.