Seminoma for xm
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Seminoma
Definition and Overview
Seminoma is the most common type of testicular germ cell tumor (GCT), accounting for approximately 50-56% of all testicular GCTs. It arises from germ cell neoplasia in situ (GCNIS) - undifferentiated germ cells located basally within the seminiferous tubules. It is considered the common precursor for all other NSGCT subtypes.
- Peak incidence: 4th-5th decade of life (older average age than NSGCT)
- Seldom occurs in childhood, young adults, or patients over 70
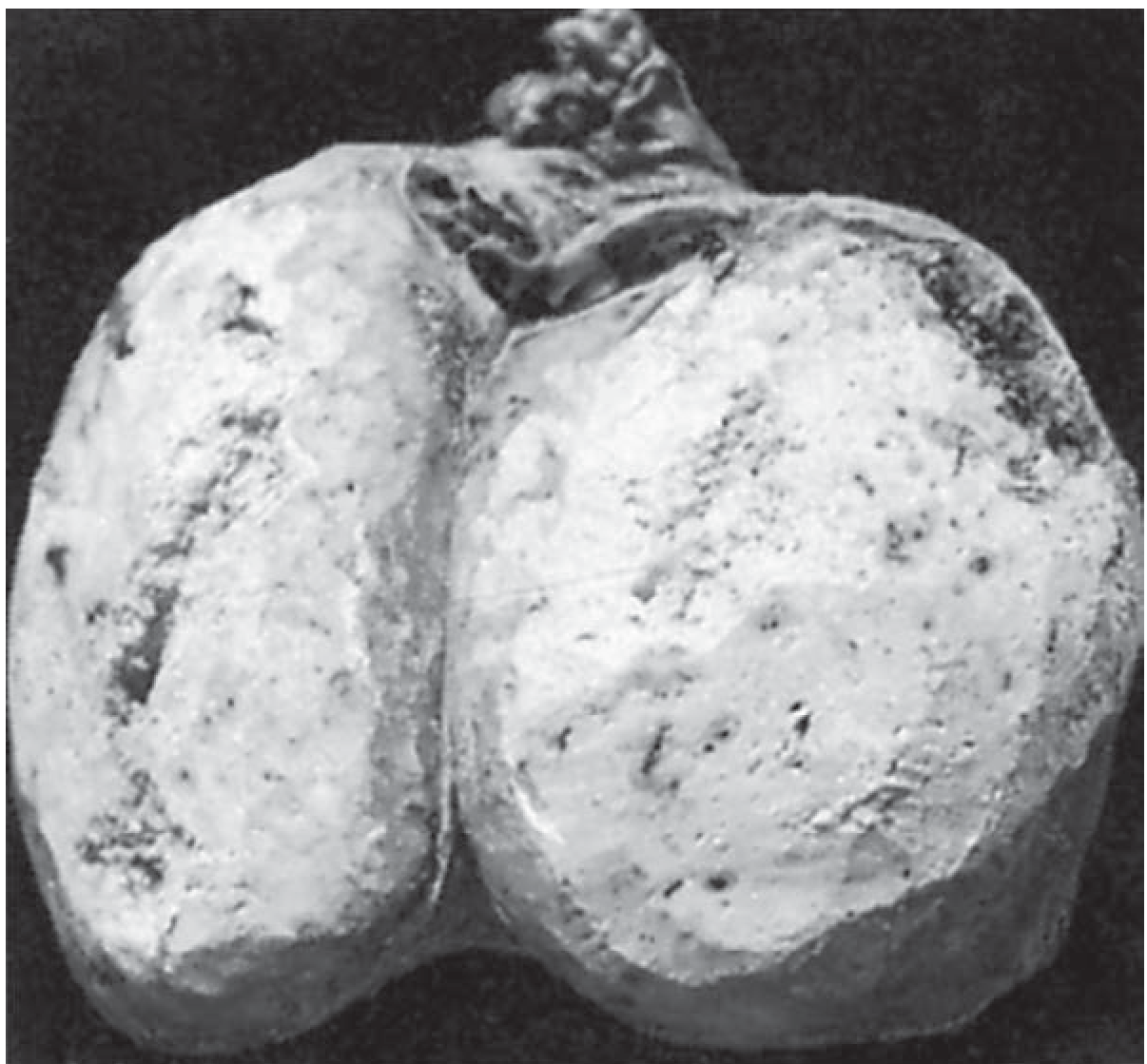
Gross & Histological Features
Gross appearance:
- Soft, tan-to-white, diffuse or multinodular mass
- Homogeneous, pinkish-cream cut surface
- Necrosis may be present but is usually focal (less prominent than other GCTs)
Histology:
- Sheets of polygonal cells with clear cytoplasm and large, rounded nuclei with prominent acidophilic nucleoli
- Cells divided into nests by fibrovascular septae containing lymphocytes
- Active lymphocytic infiltration suggests good host response and better prognosis
- Syncytiotrophoblasts (hCG-positive) present in ~15% of cases - no clear prognostic significance
- Lymphocytic infiltrates and granulomatous reactions are often seen; associated with increased incidence of sarcoidosis
Immunohistochemistry:
| Marker | Seminoma |
|---|---|
| CD30 | Negative |
| CD117 (c-kit) | Positive |
| PLAP (Placental Alkaline Phosphatase) | Strongly Positive |
| OCT 3/4 | Positive |
| AFP | Negative |
Subtypes
1. Classic Seminoma (85%)
- Most common subtype; 4th decade
- Coalescing gray nodules grossly
- Monotonous sheets of large cells with clear cytoplasm and densely staining nuclei
- ~15% have syncytiotrophoblastic elements (with corresponding mild hCG elevation)
2. Anaplastic Seminoma (5-10%)
- Requires ≥3 mitoses per high-power field
- Higher degree of nuclear pleomorphism
- Tends to present at a higher stage
- No worse prognosis when stage is controlled for - no longer considered a distinct biologic entity
3. Spermatocytic Seminoma / Spermatocytic Tumor (1%)
- Renamed "spermatocytic tumor" in 2016 WHO classification - now considered a distinct entity, NOT a true seminoma
- Does NOT arise from GCNIS; not associated with cryptorchidism or bilaterality; no i(12p)
- Peak incidence: 6th decade
- Three cell types: small lymphocyte-like cells, medium cells with dense eosinophilic cytoplasm, large mono/multinucleated cells
- Virtually benign - only 3 documented cases of metastasis; cured by orchiectomy alone
Tumor Markers
| Marker | Seminoma |
|---|---|
| AFP (alpha-fetoprotein) | Always negative - AFP elevation = NSGCT component present |
| hCG (beta) | Mildly elevated in ~15% (from syncytiotrophoblasts) |
| LDH | May be elevated; used in staging |
Key rule: An elevated AFP in a patient with apparent seminoma means the tumor must be treated as an NSGCT, regardless of histology.
Staging (TNM / AJCC)
Seminoma typically presents at an early stage:
- CS I: ~80-85% of cases
- CS II: ~10%
- CS III: ~5%
(Compare with NSGCT which presents as roughly 33/33/33.)
Metastatic Spread
- Spreads primarily via lymphatics to para-aortic lymph nodes near the origin of the gonadal vessels
- Contralateral para-aortic nodes may also be involved
- Inguinal nodes only affected if scrotal skin is involved
- Haematogenous spread is uncommon (vs. NSGCT)
- Lower incidence of occult retroperitoneal metastasis in CS I: 10-15% (vs. 25-35% for NSGCT)
Seminoma vs. NSGCT - Key Differences
| Feature | Seminoma | NSGCT |
|---|---|---|
| Peak age | 4th-5th decade | 3rd decade |
| Stage at diagnosis | Mostly CS I (85%) | Evenly distributed |
| Occult mets in CS I | 10-15% | 25-35% |
| AFP elevation | Never | Common |
| Radiosensitivity | Exquisitely sensitive | Not used (except brain mets) |
| Chemo sensitivity | Excellent | Excellent |
| IGCCCG poor risk | Does NOT exist | Exists (~10%) |
| Advanced disease good risk | >90% | ~56% |
| Post-chemo teratoma risk | Very low | High |
| Relapse after RT (systemic) | 1-4% | - |
Management
Initial Step - All Testicular Tumors
Radical inguinal orchiectomy (NOT scrotal approach - risk of altering lymphatic drainage)
Clinical Stage I Seminoma
Three accepted options (all have ~99% long-term survival):
1. Surveillance (preferred)
- ~80% are cured by orchiectomy alone
- Surveillance duration: up to 10 years (slow growth rate)
- Schedule: H&P + tumor markers every 3-6 months (year 1) → every 6-12 months (years 2-3) → annually to year 10
- Imaging: abdominal/pelvic CT each visit + CXR as indicated
- Preferred to avoid long-term toxicity of RT/chemo
2. Primary Radiotherapy
- Retroperitoneal ± ipsilateral pelvic ("dog-leg" configuration)
- Dose: 25-35 Gy in 15-20 fractions
- Long-term cancer-specific survival approaches 100%
- PFS 95-97%
- In-field recurrence <1%
- Most common relapse sites: thorax and left supraclavicular fossa
- Risks: SMN (secondary malignant neoplasm) risk ~18% at 25 years; late GI toxicity; oligospermia in 8%
3. Single-agent Carboplatin chemotherapy
- Less neurotoxicity, ototoxicity, and nephrotoxicity than cisplatin
- Long-term SMN and cardiovascular risk not fully characterized
- Non-inferior to radiotherapy in randomized trials for disease control
Clinical Stage IIA-IIB Seminoma
- Radiotherapy or chemotherapy
- Low-volume retroperitoneal disease: retroperitoneal irradiation, 5-year survival ~87%
High-Stage / Bulky Seminoma (CS IIC-III)
Chemotherapy is primary treatment:
- Good-risk: 3 cycles BEP (bleomycin + etoposide + cisplatin) or 4 cycles EP
- Intermediate-risk: 4 cycles BEP
- No "poor risk" IGCCCG category exists for seminoma - >90% of advanced seminoma is classified as good risk
Post-chemotherapy residual masses:
- Residual masses <3 cm → usually fibrosis (~90%); observation
- Residual masses >3 cm well-circumscribed → ~40% harbor residual seminoma → FDG-PET scan
- PET positive → consider PC-RPLND (post-chemotherapy retroperitoneal lymph node dissection)
- PET negative → observation
Relapsed Seminoma
- Chemo-naive relapse (after surveillance or primary RT): cisplatin-based chemotherapy; salvage approaches 100% for bulky/systemic relapse
- Post-chemotherapy relapse: VeIP x4 (vinblastine, ifosfamide, cisplatin) → 83% complete response; ~53% durable remission; high-dose chemotherapy (HDCT) also evaluated
Key Points Summary
- Seminoma = most common testicular GCT; arises from GCNIS; AFP always negative
- Histology: clear cytoplasm, fibrovascular septae with lymphocytes; PLAP+ / CD117+ / CD30-
- Three subtypes - classic (85%), anaplastic (5-10%), spermatocytic tumor (now distinct entity, benign)
- Spreads via lymphatics to para-aortic nodes; haematogenous spread uncommon
- Exquisitely radiosensitive; very chemosensitive (platin-based)
- CS I (85% at diagnosis) - surveillance preferred; RT and carboplatin are alternatives
- Advanced disease: BEP chemotherapy; post-chemo masses >3 cm need PET then consider PC-RPLND
- No IGCCCG poor-risk category; >90% of metastatic seminoma is good-risk
- Risk of NSGCT transformation (~10-15% at relapse sites) must always be considered
Sources: Campbell Walsh Wein Urology, p. 2254-2268 | Bailey & Love's Surgery, 28th ed., p. 1591 | Smith & Tanagho's General Urology, 19th ed., p. 392-395
This is a shared conversation. Sign in to Orris to start your own chat.