Difference between ebstein anomaly and esinmengerization
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from Braunwald's Heart Disease. Here is the detailed comparison:
Ebstein Anomaly vs. Eisenmenger Syndrome
These are fundamentally different entities - one is a primary structural defect present from birth, the other is an acquired hemodynamic consequence of any unrepaired left-to-right shunt.
1. Ebstein Anomaly
Definition and Anatomy
Ebstein anomaly is a congenital malformation of the tricuspid valve caused by failure of delamination (separation) of the tricuspid leaflets from the underlying RV endocardium during fetal development. This results in apical displacement of the septal (and often inferior) tricuspid leaflets down into the right ventricle.
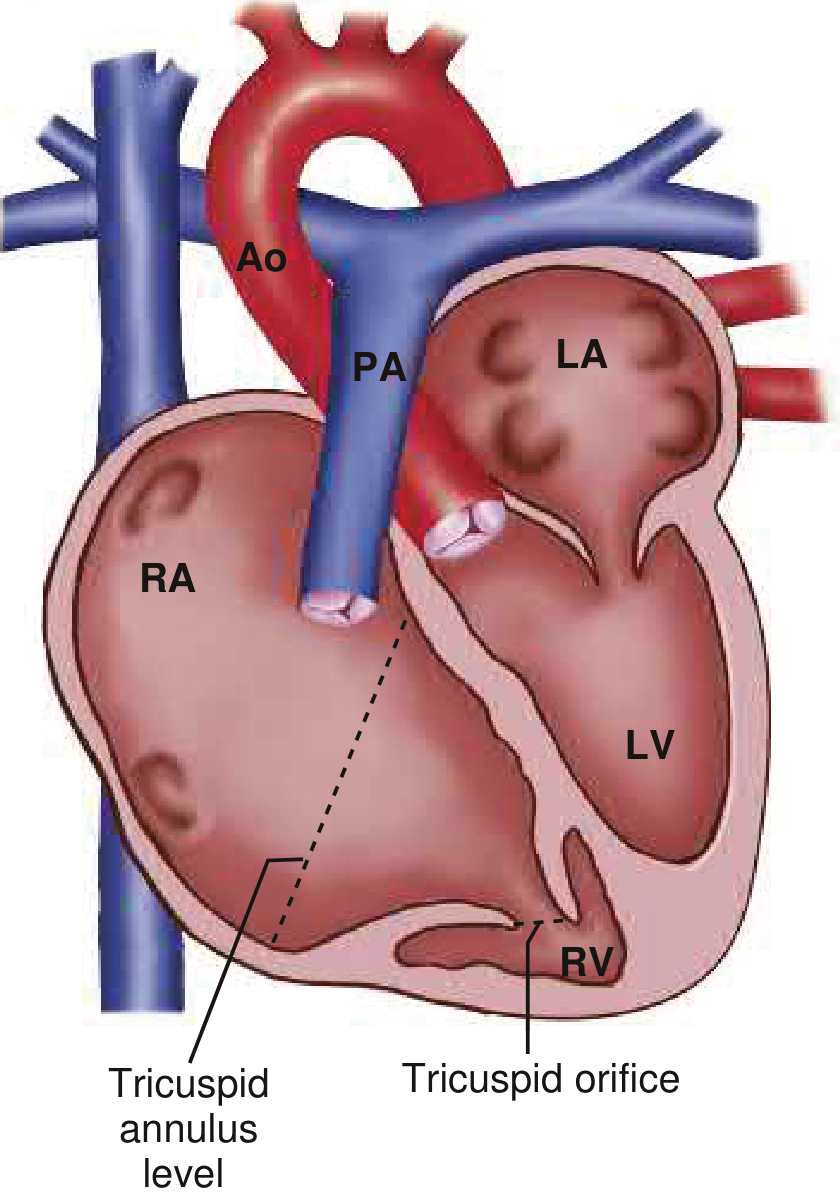
From Braunwald's Heart Disease - the dashed line shows the gap between the tricuspid annulus level and the actual tricuspid orifice, representing the "atrialized" RV
Diagnostic criteria: Displacement >8 mm/m² between the two AV valve insertion sites, or >20 mm in an adult.
Pathophysiology
- The RV is divided into two functional parts:
- "Atrialized" RV - the proximal portion between the AV groove and the displaced valve, which functions haemodynamically as part of the RA
- "Functional RV" - the remaining distal RV, which is often myopathic and thin-walled
- The anterior leaflet is elongated, fenestrated, "sail-like," and may be dysplastic or tethered
- Leads to tricuspid regurgitation (from poor valve coaptation), right heart dilation, and RV dysfunction
- The RA becomes massively dilated as it "incorporates" the atrialized RV
Shunt Direction
- No inherent shunt - but ~80% have an associated PFO or ASD
- If ASD/PFO is present + RV function is poor, a right-to-left shunt can occur (RA pressure rises above LA), causing cyanosis
- This is a passive/secondary mechanism, not the defining feature
Associated Anomalies
PFO/ASD, accessory pathways (Wolff-Parkinson-White - Mahaim-type), pulmonary stenosis, VSD, PDA, mitral valve disease, bicuspid aortic valve, coarctation of the aorta, L-loop TGA, LV non-compaction
Clinical Features
- Highly variable - spectrum from lethal in utero to asymptomatic adult
- Symptoms: exercise intolerance, fatigue, palpitations, paradoxical embolism, cyanosis (if R-to-L shunt via ASD)
- Arrhythmias are a dominant feature: AVRT is most common, atrial flutter/fibrillation, WPW, multiple accessory pathways (associated with sudden death)
ECG - Classic Features
| Finding | Significance |
|---|---|
| "Himalayan" P waves (>5 mm) | Massive right atrial enlargement |
| Short PR + delta wave | WPW/accessory pathway (in ~25%) |
| Prolonged PR | AV conduction delay |
| Complete/incomplete RBBB | Right conduction delay |
| Low voltage QRS | Myopathic RV |
CXR
- "Box-shaped" heart - massively enlarged RA/atrialized RV
- Decreased pulmonary vascular markings
- Small aorta and pulmonary trunk shadow
Treatment
- Arrhythmia ablation (preferably before surgery)
- Tricuspid valve repair (cone repair - Gold standard) or replacement
- Bidirectional cavopulmonary connection ("1.5-ventricle repair") if RV function poor
- Heart transplantation in end-stage disease
- Incidence: 1 per 200,000 live births
2. Eisenmenger Syndrome
Definition
Eisenmenger syndrome is not a single lesion - it is a pathophysiological process in which an uncorrected left-to-right shunt causes progressive pulmonary vascular injury, leading to irreversible pulmonary arterial hypertension (PAH). When pulmonary vascular resistance (PVR) surpasses systemic vascular resistance (SVR), the shunt reverses to right-to-left, causing cyanosis.
Underlying Lesions
| Shunt Type | Example Lesions | Onset |
|---|---|---|
| Post-tricuspid (large) | VSD, AVSD, PDA, truncus arteriosus | First years of life |
| Pre-tricuspid | ASD (minority, <10%) | Adulthood |
Post-tricuspid shunts transmit systemic pressure directly to the pulmonary circulation - they cause Eisenmenger syndrome much faster and more reliably than pre-tricuspid shunts.
Pathophysiology (Mechanism of "Eisenmengerization")
- Large L-to-R shunt → pulmonary over-circulation
- Pulmonary arterioles undergo irreversible medial hypertrophy, intimal proliferation, plexiform lesions (Heath-Edwards changes)
- PVR rises progressively
- When PVR ≥ SVR: shunt reverses (R-to-L)
- Deoxygenated blood enters systemic circulation → central cyanosis
- Secondary erythrocytosis develops (compensatory, due to chronic hypoxia)
Clinical Features
Central cyanosis + digital clubbing are the hallmarks.

Braunwald's Heart Disease - characteristic digital clubbing and cyanosis in Eisenmenger syndrome
Physical exam:
- Loud P2 (pulmonary hypertension)
- Right parasternal heave
- Prominent jugular venous a-wave
- High-pitched diastolic murmur of pulmonary regurgitation
- Systolic murmurs may be faint or absent (because shunt flow is now minimal/reversed)
Multi-organ Complications
| System | Complication |
|---|---|
| Hematologic | Erythrocytosis, iron deficiency, thrombocytopenia, leukopenia, hyperviscosity |
| Rheumatologic | Hyperuricemia, gout, arthritis, myalgias |
| Neurologic | Paradoxical embolism, cerebrovascular accidents, intracranial abscesses |
| Pulmonary | Hemoptysis (from pulmonary hypertension) |
| Infectious | Brain abscesses, endocarditis, pneumonia |
CXR
- Dilated central pulmonary arteries with peripheral "pruning"
- RA and RV enlargement
- (Contrast with Ebstein's box-shaped heart which has decreased pulmonary markings)
ECG
Right atrial enlargement, right axis deviation, biventricular hypertrophy (from PAH), ST-T changes
Management
- Irreversible - shunt closure is contraindicated once Eisenmenger syndrome is established (would remove the only "relief valve" for the overloaded RV)
- Pulmonary vasodilators: Bosentan (endothelin receptor antagonist) - approved; sildenafil, macitentan
- Avoid: volume depletion, extreme exercise, extreme heat, iron deficiency, air travel without supplemental O2
- Pregnancy is contraindicated (maternal mortality ~30-50%)
- Heart-lung transplantation (definitive but limited availability)
- Antibiotic prophylaxis for all patients
Prognosis
Better than other forms of severe PAH. Death becomes common from the 4th decade onward. Causes of death: sudden death, congestive heart failure, pulmonary hemorrhage. Risk factors for mortality: pre-tricuspid shunt type, older age, lower resting O2 saturations, non-sinus rhythm, pericardial effusion.
Side-by-Side Comparison
| Feature | Ebstein Anomaly | Eisenmenger Syndrome |
|---|---|---|
| Nature | Primary structural defect | Acquired hemodynamic syndrome |
| Valve involved | Tricuspid valve (displaced) | No valve malformation |
| Core pathology | Failure of TV delamination → apical displacement | L-to-R shunt → irreversible PAH → shunt reversal |
| Cyanosis | Secondary (if ASD/PFO + RV failure) | Primary, defining feature |
| Direction of cyanosis mechanism | R-to-L via ASD due to elevated RA pressure | R-to-L due to PVR > SVR |
| RV | Atrialized (dysfunctional from birth) | Hypertrophied (from PAH) |
| Pulmonary pressures | Normal to low (decreased pulmonary flow) | Severely elevated (defining PAH) |
| Shunt | No inherent shunt; ASD/PFO may co-exist | Pre-existing intracardiac/extracardiac shunt is required |
| ECG hallmark | "Himalayan" P waves + WPW/accessory pathway | Right axis deviation + biventricular hypertrophy |
| CXR hallmark | "Box-shaped" heart, decreased lung markings | Dilated pulmonary arteries, peripheral pruning |
| Arrhythmia | Prominent (AVRT, WPW, AF) | Less prominent |
| Treatment | Tricuspid valve repair/replacement; ablation | Pulmonary vasodilators; transplant; shunt closure contraindicated |
| Reversibility | Structural - surgical repair possible | Pulmonary vascular disease is irreversible |
| Incidence | 1/200,000 live births | Any unrepaired L-to-R CHD |
Key conceptual distinction: Ebstein anomaly is a tricuspid valve problem from birth - the heart is built wrong. Eisenmenger syndrome is a pulmonary vascular problem that develops over years because a shunt was left untreated. Both can cause cyanosis and right heart failure, but through completely different pathways.
Sources: Braunwald's Heart Disease, 12th Ed., Ch. 82 (Adult Congenital Heart Disease)
From homoeopathic paint of view drugs and its pathophysiology
Asking for Preferences
From a homoeopathic standpoint, treatment is based on totality of symptoms, miasm, and organ affinity - not on disease labels. Here is a detailed breakdown for both conditions:
Homoeopathic Approach to Ebstein Anomaly & Eisenmenger Syndrome
Understanding the Pathophysiology Through Homoeopathic Lens
Miasmatic Background
| Condition | Dominant Miasm | Reasoning |
|---|---|---|
| Ebstein Anomaly | Sycotic + Syphilitic | Structural malformation (sycosis = overgrowth/malformation of tissue); progressive RV failure and degeneration (syphilitic = destructive) |
| Eisenmenger Syndrome | Syphilitic (dominant) + Psoric base | Irreversible destruction of pulmonary vasculature, vascular degeneration, tissue necrosis - classic syphilitic obliteration; hypoxia-driven systemic suffering (psoric) |
EBSTEIN ANOMALY - Homoeopathic Drugs
The key symptoms to prescribe on: right-sided heart enlargement, tricuspid regurgitation, cyanosis (R-to-L via ASD), arrhythmias (WPW, AVRT, AF), RV dysfunction, fatigue, exercise intolerance, oedema, palpitations.
1. Digitalis purpurea (Most Indicated)
Organ affinity: Heart - valvular insufficiency, enlargement, weak heart muscle
Pathophysiological correlation:
- Digitalis covers the myopathic, failing right ventricle with severe tricuspid regurgitation
- Profound bradycardia with irregular pulse - covers arrhythmias of Ebstein
- Characteristic: Pulse is slow, irregular, intermittent - the patient fears the heart will stop
- Blueness of lips and fingernails (early cyanosis)
- Hepatic congestion, oedema of legs, ascites - all from right heart failure
- "Least motion aggravates" - exercise intolerance
Keynotes for Ebstein:
"Pulse slow, weak, irregular; least excitement aggravates. Blueness of surface. Dropsy from valvular disease."
Potency guidance: 3x-6x (low potencies support in organic disease); constitutional higher potencies under expert supervision
2. Crataegus oxyacantha (Cardiac Tonic/Supportive)
Organ affinity: Heart muscle, coronary and peripheral circulation
Pathophysiological correlation:
- Myopathic/weakened RV (the functional RV in Ebstein is thin-walled and myopathic)
- Acts as a "heart tonic" - improves myocardial contractility
- Indicated in cardiac dilation with weakness - exactly the atrialized/dilated RV
- Dyspnoea on least exertion, oedema, irregular pulse
- Valvular insufficiency where the heart is enlarged and dilated
Keynotes:
"Weakness of the heart muscle with dilated chambers. Cardiac dropsy. Dyspnea on the slightest exertion."
3. Laurocerasus (Right Heart + Cyanosis)
Organ affinity: Right side of heart, valvular disease, venous stasis, cyanosis
Pathophysiological correlation:
- Covers cyanosis from right-sided heart disease better than most remedies
- Tricuspid valve disease - regurgitation leading to venous backpressure
- Suffocative attacks - patient grasps for air; lips and nails blue
- Cold, clammy extremities, weak pulse
- Syncope and fainting - from reduced cardiac output
- Scratching in throat (reflective of venous congestion)
Keynotes for Ebstein:
"Cyanosis from right-sided valvular disease. Cold blue lips. Suffocation. Feeble pulse. Venous stasis."
4. Spigelia anthelmia (Palpitations + Right-sided Heart)
Organ affinity: Heart, pericardium; strongly right-sided
Pathophysiological correlation:
- Violent palpitations (from arrhythmias - AVRT, atrial flutter in Ebstein)
- Patient can hear and feel the heartbeat
- Palpitations worse on motion, on lying on the left side
- Precordial pain, visible pulsation over the praecordium (from dilated RA/atrialized RV)
Keynotes:
"Violent palpitations, visible through clothing. Heart beat heard in ears. Worse from motion."
5. Lachesis mutus (ASD + Right-to-Left Shunt, Cyanosis)
Organ affinity: Circulatory system, venous congestion, left-sided but crosses over
Pathophysiological correlation:
- Where there is venous backpressure and blueness - right-to-left shunting via ASD
- Palpitations, dyspnoea, worse after sleep (classically - wakes from sleep suffocating)
- Cannot bear tight clothing around chest or neck
- Purplish discolouration of skin
6. Naja tripudians (Organic Heart Disease + Arrhythmia)
Organ affinity: Heart (organic lesions), vagus nerve stimulation
Pathophysiological correlation:
- Organic valvular disease with arrhythmia - directly matches Ebstein
- Constant desire to be fanned, dyspnoea
- Threatened paralysis of heart - matches myopathic RV of Ebstein
- Post-valvular disease with cardiac dropsy
Keynote:
"Valvular disease with marked arrhythmia and threatening cardiac paralysis."
7. Kalmia latifolia (Right-sided + Slow Pulse)
- Slow, irregular pulse with valvular disease
- Palpitations worse on stooping and lying down
- Right-sided cardiac symptoms with pain radiating down arm
EISENMENGER SYNDROME - Homoeopathic Drugs
Key symptoms: central cyanosis, digital clubbing, severe dyspnoea, erythrocytosis, hyperviscosity, pulmonary hypertension, haemoptysis, fatigue, right heart failure, paradoxical embolism.
1. Strophanthus hispidus (Pulmonary Hypertension + Venous Overload)
Organ affinity: Heart, pulmonary circulation
Pathophysiological correlation:
- Covers pulmonary venous hypertension and pulmonary congestion
- Marked dyspnoea on exertion, can barely walk
- Oedema of lungs - wet rales, frothy sputum (haemoptysis in Eisenmenger)
- Cardiac enlargement from sustained pressure overload (RVH in Eisenmenger)
2. Digitalis purpurea (Shared with Ebstein - Right Heart Failure)
As above - covers the RV failure, venous congestion, cyanosis, and arrhythmia that develop in Eisenmenger in later stages.
3. Arsenicum album (Cyanosis + Restlessness + Dyspnoea)
Organ affinity: Lungs, heart, blood vessels, systemic
Pathophysiological correlation:
- Central cyanosis with intense restlessness and anxiety - hallmark of Eisenmenger's poor oxygenation
- Dyspnoea worse at midnight (1-3 AM), cannot lie down
- Haemoptysis - burning in chest
- Oedema of extremities, ascites
- Erythrocytosis correlation: Arsenicum has a well-known action on the blood - affects red blood cell production; the secondary polycythaemia of Eisenmenger finds its closest remedy analogy here
- Profound prostration yet anxious
Keynotes:
"Dyspnea, restlessness, burning in chest, cannot lie down. Dropsy. Haemoptysis."
4. Antimonium tartaricum (Pulmonary Congestion + Cyanosis)
Organ affinity: Lungs, respiratory mucosa
Pathophysiological correlation:
- Blueness of face, lips, nails with severe respiratory distress - covers Eisenmenger's cyanosis
- Rattling mucus in chest that cannot be expectorated (pulmonary congestion from pulmonary hypertension)
- Cold, clammy sweat, drowsy - low cardiac output state
- Oedema, hypoxia, patient wants to be fanned
5. Carbo vegetabilis (Severe Cyanosis + Collapse State)
Organ affinity: Venous system, impaired oxygenation
Pathophysiological correlation:
- "The corpse reviver" - covers extreme venous stasis and cyanosis
- Cold breath, cold extremities, cyanotic face - covers end-stage Eisenmenger
- Great desire to be fanned (needs oxygen - parallels Eisenmenger's hypoxemia)
- Capillary stasis, blue discolouration
- Haemorrhage tendency (covers haemoptysis)
- Patient is collapsed, cold, blue but wants fresh air
Keynote:
"Venous stasis, cyanosis, patient is cold and blue but craves to be fanned. Vital force nearly exhausted."
6. Phosphorus (Haemoptysis + Pulmonary Vascular Disease)
Organ affinity: Blood vessels, lungs, haemorrhagic tendency
Pathophysiological correlation:
- Haemoptysis - bright red blood (from pulmonary hypertension-induced vessel rupture in Eisenmenger)
- Erythrocytosis + bleeding tendency - Phosphorus acts on blood and blood vessels
- Congestion of lungs, dyspnoea, palpitations
- Paradoxical embolism / CVA risk - Phosphorus covers haemorrhagic and thromboembolic tendencies
- Digital clubbing (Phosphorus has affinity for bones and periosteum - hypertrophic osteoarthropathy)
7. Baryta carbonica (Vascular Sclerosis - Pulmonary Arterial Changes)
Organ affinity: Arteries, connective tissue, endothelium
Pathophysiological correlation:
- The irreversible obliterative changes in pulmonary arterioles (intimal fibrosis, plexiform lesions) represent a syphilitic-sycotic degenerative process
- Baryta carb covers sclerotic changes in blood vessels, hardening of arteries
- Suited to conditions where tissues have undergone degenerative/fibrotic change
- Dyspnoea on exertion in elderly/adults with long-standing disease
8. Aurum metallicum (Pulmonary Hypertension + Depression)
Organ affinity: Heart, arteries, veins; profound action on blood vessels
Pathophysiological correlation:
- Valvular disease with pulmonary hypertension - Aurum has profound affinity for elevated vascular pressure
- Palpitations with dyspnoea, visible heart pulsation
- Arterial hypertension - directly applicable to pulmonary arterial hypertension in Eisenmenger
- The despair and depression that accompanies chronic Eisenmenger (poor prognosis awareness) - Aurum's mental picture
Summary Comparison Table
| Symptom Cluster | Best Homoeopathic Remedy |
|---|---|
| Structural valve defect + RV dilation | Digitalis, Crataegus |
| Tricuspid regurgitation + right-sided failure | Laurocerasus, Digitalis |
| Arrhythmias (AVRT, WPW, palpitations) | Spigelia, Naja, Digitalis |
| Cyanosis from R-to-L shunt (both) | Laurocerasus, Lachesis, Carbo veg |
| Pulmonary hypertension | Aurum met, Strophanthus, Baryta carb |
| Central cyanosis + restlessness | Arsenicum album |
| Haemoptysis | Phosphorus, Carbo veg, Arsenicum |
| Erythrocytosis/blood disorders | Phosphorus, Arsenicum |
| Pulmonary vascular sclerosis (irreversible) | Baryta carb, Aurum met |
| Severe collapse/end-stage | Carbo veg, Antimonium tart |
| Oedema + dropsy | Digitalis, Crataegus, Arsenicum |
Important Homoeopathic Notes
-
Palliation vs. Cure: In Ebstein anomaly (structural defect), homoeopathy can palliate symptoms and improve quality of life but cannot physically reposition the tricuspid valve. Surgery remains the definitive treatment. Homoeopathy may be used as an adjunct.
-
In Eisenmenger syndrome: Since the pulmonary vascular disease is irreversible, homoeopathic treatment aims at managing symptoms, slowing deterioration, and improving functional capacity.
-
Individualisation is paramount: The remedy must match the totality of the patient - mental generals, physical generals, modalities, and particulars override any disease diagnosis.
-
Miasm-specific intercurrent remedies:
- Sycotic: Thuja occidentalis, Medorrhinum
- Syphilitic: Syphilinum (Lueticum), Aurum met, Mercurius
-
Potency selection: In severe organic/structural cardiac disease, low potencies (3x, 6x, 30c) given frequently are preferred. High potencies are used constitutionally with caution.
This is a shared conversation. Sign in to Orris to start your own chat.