Jvp final year mbbs harrison ref
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a complete, exam-focused answer. Here is the full Harrison's-referenced JVP guide for final year MBBS:
Jugular Venous Pulse (JVP) - Harrison's 22E Reference
What is JVP?
The JVP is the single most important bedside measurement from which to estimate volume status. It reflects right atrial pressure and provides a non-invasive window into the right heart.
- Use internal jugular vein (IJV) - preferred because the external jugular vein is valved and not directly in line with the SVC and right atrium
- The external jugular can still discriminate high vs. low CVP but is less reliable
How to Measure JVP
- Patient positioned at 30-45° incline
- Identify the top of the jugular venous pulsation column
- Measure vertical distance from the sternal angle (angle of Louis)
- Normal: <4.5 cm above the sternal angle at 30°
- Abnormal: >4.5 cm at 30°
Key point from Harrison's: The sternal angle method systematically underestimates CVP. Use it to distinguish normal from elevated - not for precise quantification. The clavicle is an easier reference: venous pulsations above the clavicle in the sitting position are clearly abnormal (the clavicle-to-right atrium distance is at least 10 cm).
Convert cmH₂O to mmHg: 1.36 cmH₂O = 1.0 mmHg
The JVP Waveform
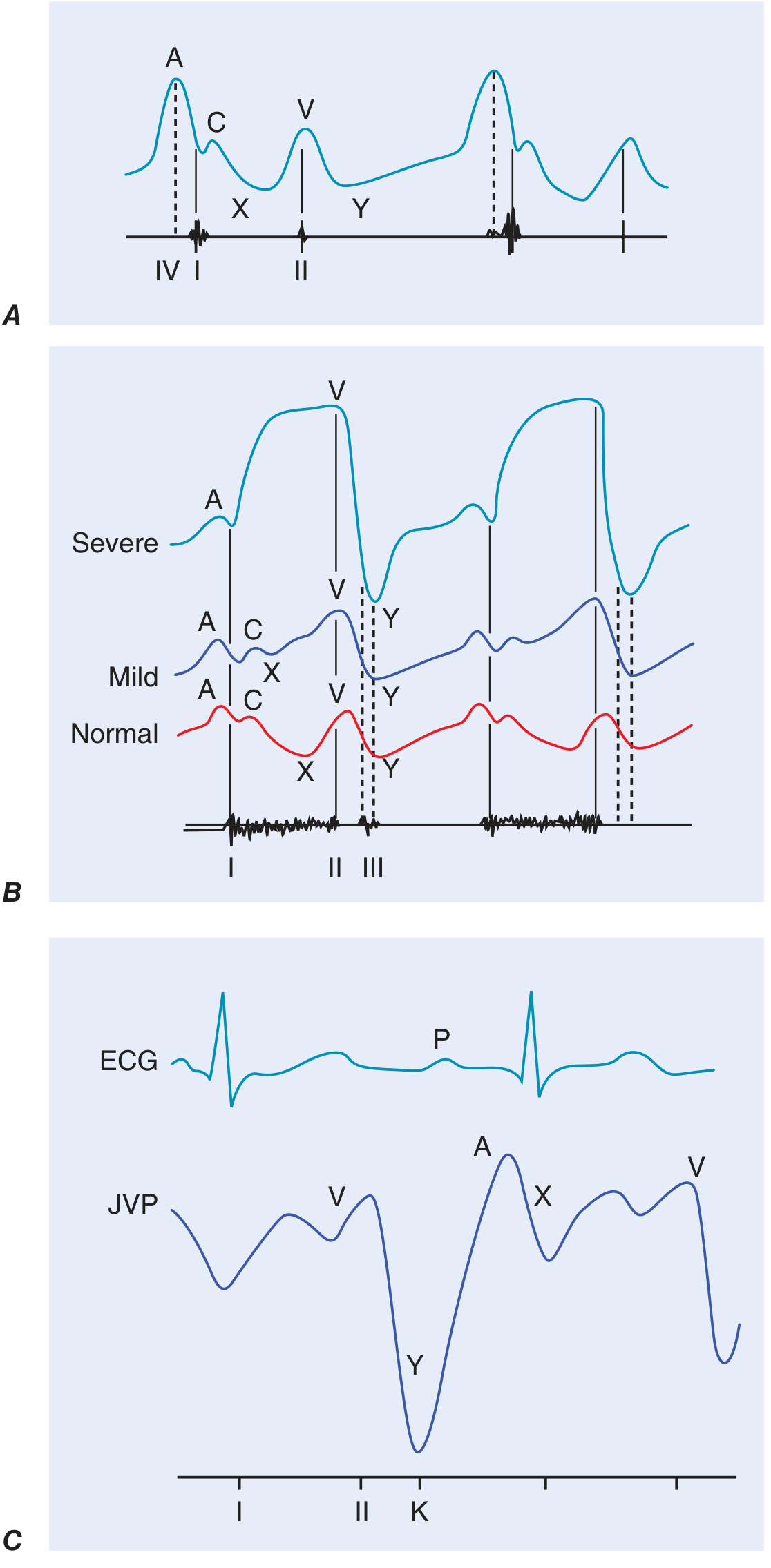
Panel A: Normal JVP with prominent A wave (reduced RV compliance). Panel B: Progression of TR from normal → mild → severe (ventricularized waveform). Panel C: JVP in constrictive pericarditis showing rapid Y descent (K descent).
Waves and Their Meanings
| Component | Physiological Basis | Timing | Key Point |
|---|---|---|---|
| a wave | Right atrial presystolic contraction | After P wave on ECG, just before S1 | Due to RA contraction |
| c wave | Closed tricuspid valve pushed into RA during early ventricular systole | Between a and v | Interrupts the x descent |
| x descent | Fall in RA pressure after tricuspid valve opens | After a wave | Atrial relaxation + tricuspid opening |
| v wave | Atrial filling (atrial diastole) during ventricular systole | During ventricular systole | Represents passive filling of RA |
| y descent | Opening of tricuspid valve, blood flows into RV | After v wave peak | Rapid fall when TR severe |
JVP vs. Carotid Pulse: How to Distinguish
| Feature | JVP | Carotid Pulse |
|---|---|---|
| Waveform | Biphasic (in sinus rhythm) | Monophasic |
| Palpability | Not easily palpable | Easily palpable |
| Obliteration | Obliterated with light pressure | Cannot be obliterated |
| Posture/Inspiration | Changes (falls on inspiration normally) | No change |
Abnormal JVP Waveforms - High-Yield Table
| Finding | Cause | Mechanism |
|---|---|---|
| Prominent / Large a wave | Reduced RV compliance, pulmonary stenosis, pulmonary hypertension, tricuspid stenosis | RA must contract harder against resistance |
| Cannon a wave | AV dissociation (VT, complete heart block, ventricular pacing) | RA contracts against a closed tricuspid valve |
| Absent a wave | Atrial fibrillation | No organized atrial contraction |
| Large v wave | Tricuspid regurgitation (TR) | Retrograde flow from RV into RA during systole |
| "Ventricularized" waveform | Severe TR | c and v waves merge; waveform resembles RV pressure curve |
| Blunted / slow y descent | Tricuspid stenosis, cardiac tamponade | Obstruction to RV inflow; slow emptying of RA |
| Rapid y descent | Constrictive pericarditis, severe TR, ASD | Rapid early diastolic filling |
Special Signs
Kussmaul's Sign
- Definition: Rise (or failure to fall) in JVP with inspiration (opposite of normal)
- Normal response: JVP falls with inspiration (due to reduced intrathoracic pressure)
- Classically associated with: Constrictive pericarditis
- Also seen in: Restrictive cardiomyopathy, massive pulmonary embolism, RV infarction, advanced LV systolic heart failure, post-cardiac surgery
Abdominojugular (Hepatojugular) Reflux
- Technique: Firm continuous pressure over right upper quadrant for >15 seconds
- Positive result: Sustained rise of >3 cm in JVP during abdominal compression
- Wait 10 seconds before assessing (allows respiratory artifacts and abdominal tensing to subside)
- Patients must NOT hold their breath (Valsalva-like maneuver invalidates the test)
- Clinical significance: Predicts pulmonary artery wedge pressure >15 mmHg in heart failure
Clinical Correlations (Exam Favorites)
| Condition | JVP Finding |
|---|---|
| Heart failure (right-sided) | Elevated JVP + peripheral edema |
| Cardiac tamponade | Elevated JVP + blunted y descent (x descent prominent) |
| Constrictive pericarditis | Elevated JVP + Kussmaul's sign + rapid/prominent y descent |
| Tricuspid regurgitation | Large cv wave (ventricularized) |
| Tricuspid stenosis | Large a wave + slow y descent |
| Pulmonary hypertension | Large a wave (from RV hypertrophy/reduced compliance) |
| VT (vs. SVT) | Cannon a waves → identifies AV dissociation → VT origin |
| Atrial fibrillation | Absent a wave |
| RV infarction | Elevated JVP + clear lungs + hypotension (triad) |
| Nephrotic/hypoalbuminemia | Peripheral edema without elevated JVP |
Quick Memory Aid: "acvxy"
a - Atrial contraction (presystolic)
c - Closure of tricuspid (early systole)
v - Venous filling (late systole)
x - fall after a (atrial relaxation)
y - fall after v (tricuspid opens, RV filling)
c - Closure of tricuspid (early systole)
v - Venous filling (late systole)
x - fall after a (atrial relaxation)
y - fall after v (tricuspid opens, RV filling)
Descents go down: x descent = fall after a; y descent = fall after v.
Summary: Most Testable Points
- IJV preferred over EJV for JVP assessment
- Measurement reference: sternal angle; >4.5 cm at 30° = abnormal
- Cannon a wave = AV dissociation (VT marker at bedside)
- No a wave = AF
- Large v wave = TR; severe TR → ventricularized waveform
- Slow y descent = Tamponade or TS; Rapid y = Constrictive pericarditis
- Kussmaul's sign: JVP rises on inspiration - classic for constrictive pericarditis
- Abdominojugular reflux: positive if JVP rises >3 cm; predicts PAWP >15 mmHg
- Elevated JVP + edema = volume overload (HF, constrictive pericarditis)
- Edema without elevated JVP = hypoalbuminemia, venous/lymphatic obstruction
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 246: Cardiovascular Examination, p. 1904
This is a shared conversation. Sign in to Orris to start your own chat.