Placental development. The role of the chorion in the formation of the placenta. The structure and role of the hematoplacental barrier
Placental Development, the Role of the Chorion, and the Hematoplacental Barrier
1. Overview: The Placenta as a Fetomaternal Organ
- Fetal part — derived from the villous chorion (chorion frondosum)
- Maternal part — derived from the decidua basalis (endometrium)
2. The Decidua
| Region | Location | Role |
|---|---|---|
| Decidua basalis | Deep to the conceptus | Forms the maternal part of the placenta |
| Decidua capsularis | Superficial layer overlying the conceptus | Compresses and eventually fuses with decidua parietalis |
| Decidua parietalis | Remaining endometrium | Lines the remainder of the uterine cavity |
3. Development of the Placenta
3.1 Trophoblast Differentiation and Early Uteroplacental Circulation
- Syncytiotrophoblast: multinucleated, invasive, actively erodes the decidua; forms trophoblastic lacunae filled with maternal blood
- Cytotrophoblast (Langhans cells): mitotically active inner layer that supplies new cells to the syncytiotrophoblast
3.2 Formation of Chorionic Villi
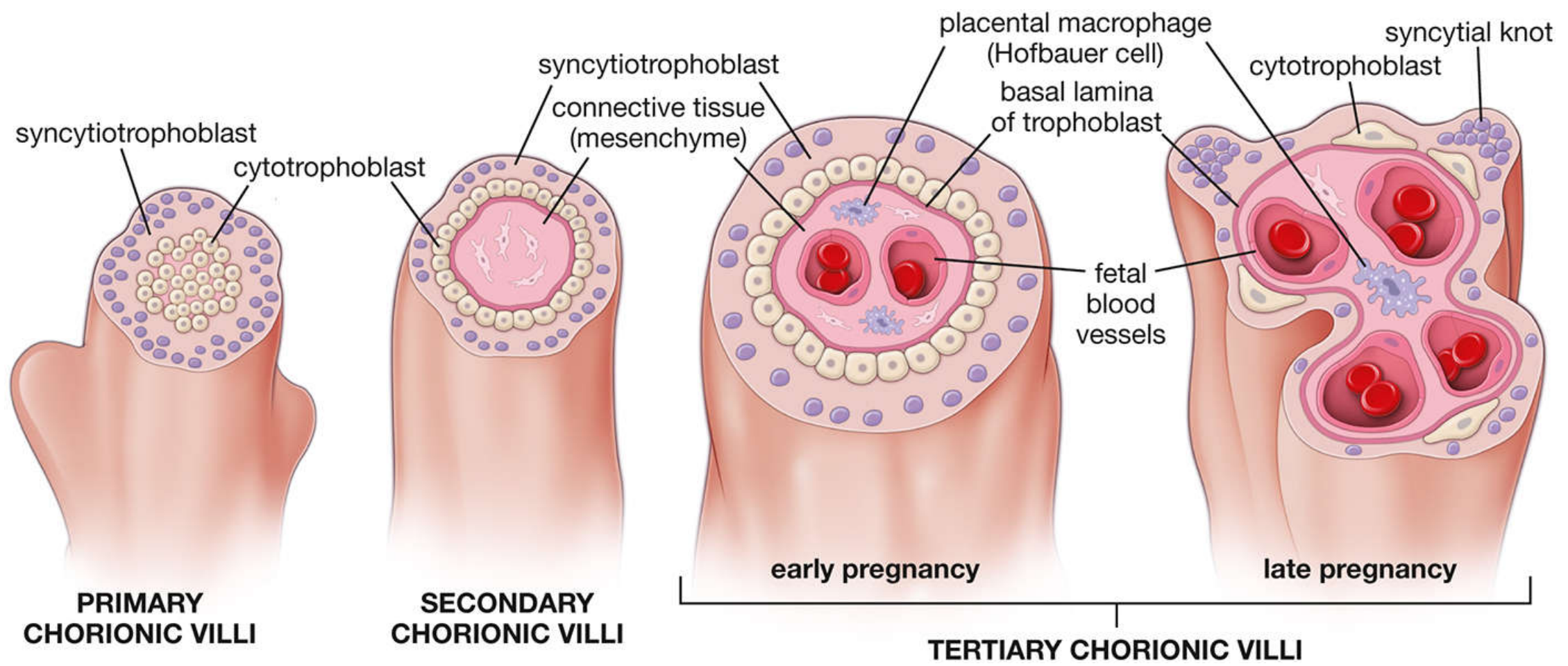
4. The Role of the Chorion in Placental Formation
4.1 Smooth Chorion vs. Villous Chorion
- Chorion laeve (smooth chorion): Villi on the side of the decidua capsularis are compressed and their blood supply reduced → they degenerate → a relatively avascular, smooth surface results
- Chorion frondosum (villous chorion): Villi on the side of the decidua basalis proliferate vigorously, branch profusely, and enlarge → this forms the fetal part of the placenta
4.2 Cytotrophoblastic Shell and Attachment
4.3 Cotyledons and Placental Septa
4.4 Maternal Blood Supply
5. Structure of the Hematoplacental Barrier
5.1 Layers of the Barrier
- Syncytiotrophoblast — outer multinucleated layer with dense microvilli; the critical barrier layer
- Cytotrophoblast — inner continuous layer of mononuclear cells (Langhans cells)
- Connective tissue (mesenchyme) of the villus
- Endothelium of fetal capillaries
- Syncytiotrophoblast
- Basal lamina of the trophoblast
- Connective tissue of the villus
- Basal lamina of the endothelium
- Endothelium of fetal capillary
5.2 Electron-Microscopic Appearance
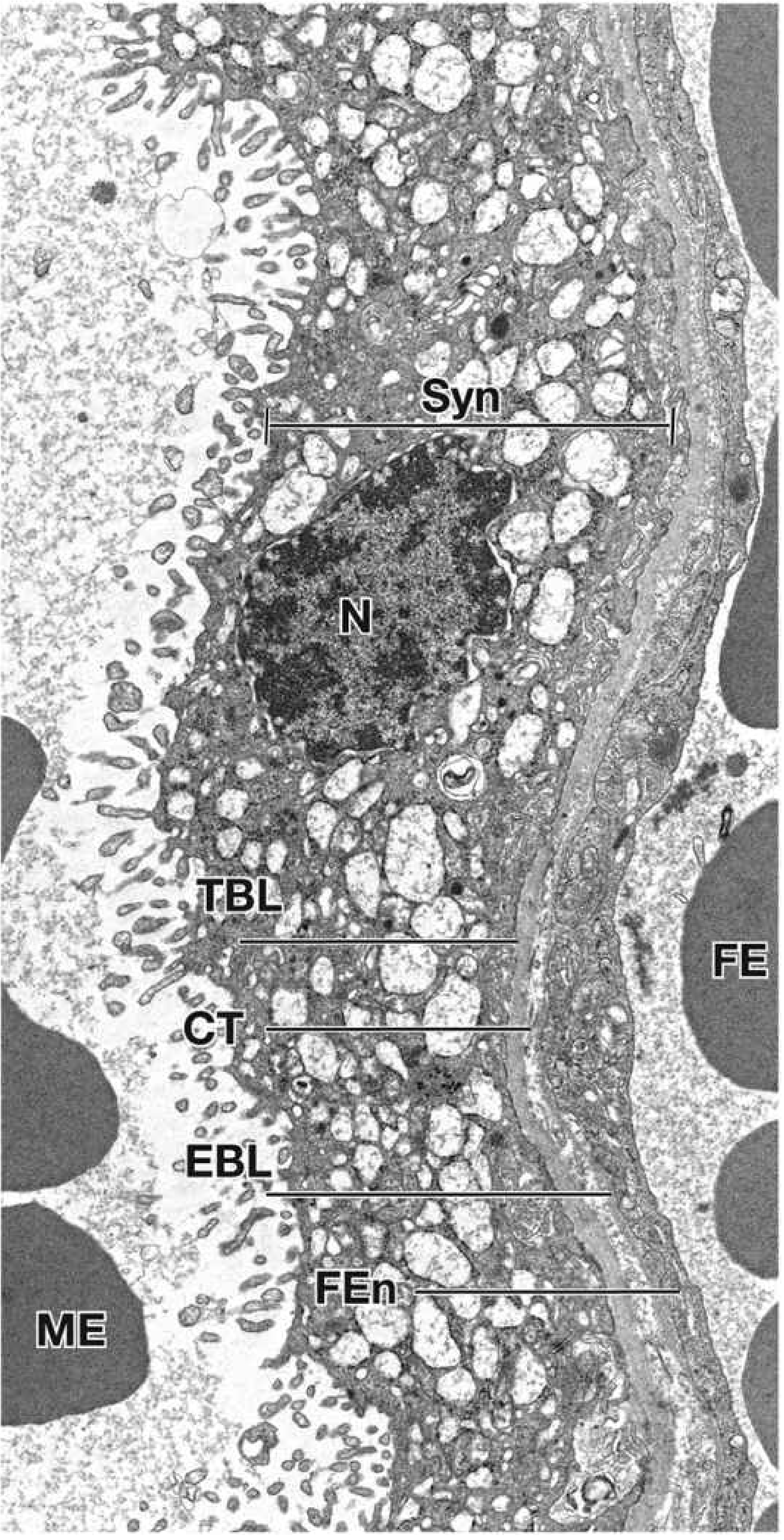
- Dense microvilli on the apical surface (increases surface area for exchange)
- Abundant transport vesicles, rER, sER, mitochondria
- No lateral intercellular gaps (tight barrier function)
5.3 Changes Through Pregnancy
| Feature | Early pregnancy | Late pregnancy |
|---|---|---|
| Cytotrophoblast layer | Continuous, thick | Thin or discontinuous |
| Syncytiotrophoblast | Thick, few nuclei | Thinner; forms syncytial knots |
| Fetal vessels | Sparse in stroma | Numerous, close to surface |
| Barrier thickness | Thick (4+ layers) | Markedly attenuated |
| Fibrinoid material | Absent | Accumulates on villus surfaces |
6. Functions of the Hematoplacental Barrier
6.1 Substances Transferred from Mother → Fetus
| Substance | Mechanism |
|---|---|
| O₂ | Simple diffusion |
| Glucose | Facilitated diffusion (GLUT-1) |
| Amino acids | Active transport (against gradient) |
| Water | Simple diffusion |
| Vitamins | Diffusion (water-soluble > fat-soluble) |
| IgG antibodies | Pinocytosis → passive immunity |
| Electrolytes, hormones | Various |
6.2 Substances Transferred from Fetus → Mother
6.3 Barrier Limitations
6.4 Endocrine Function
- Steroid hormones: chiefly progesterone (maintains pregnancy, inhibits uterine contractions)
- Protein hormones: hCG (maintains corpus luteum), human chorionic somatomammotropin (hCS), relaxin, leptin
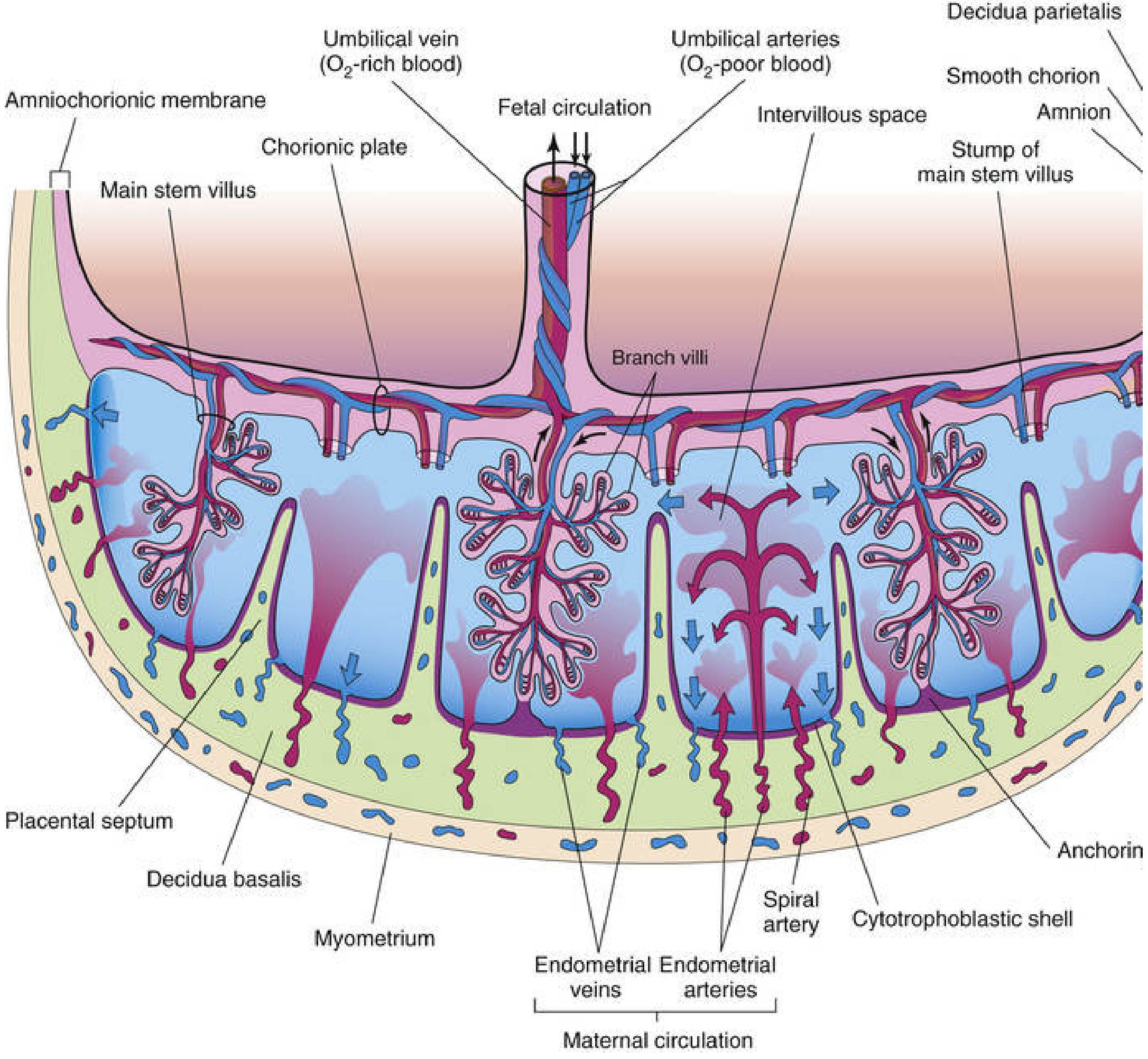
Summary Diagram of Placental Organisation
- Fetal side (chorionic plate): umbilical arteries divide radially → stem villi → branch villi with capillary networks
- Intervillous space: filled with ~150 mL maternal blood renewed 3–4×/min
- Maternal side (basal plate): decidua basalis + cytotrophoblastic shell; 80–100 spiral arteries pierce it
- Cotyledons: 15–30 units separated by placental septa, each with 2+ stem villi
- The Developing Human: Clinically Oriented Embryology (Moore, Persaud & Torchia)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina)
- Color Atlas of Human Anatomy, Vol. 2: Internal Organs (Schünke et al.)
Make ppt of on this topic in about 10-15 slides
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
mkdir -p /home/daytona/workspace/placenta-ppt && echo "created"
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/8c8b8cec58e5a18c6779f331d42b9cf73a2dea43ab1a2ec616d8a102b7cfe83e.png" \ "https://cdn.orris.care/cdss_images/2d2f73f1f3b06fa101b36af8be768232d7e6d7bfa05bccd1d473a3f524552d0b.png" \ "https://cdn.orris.care/cdss_images/cf95d6bd3489d76433b2efd015ea28fdcc52726adb283d5a02565701ca44b53b.png" \ "https://cdn.orris.care/cdss_images/15475989e4f3fd54a75e45c0ad3ccdeae59c66094f46de87f46f89d9847a1ec1.png" 2>&1 | head -5
Your input exceeds the context window of this model. Please adjust your input and try again.
We encountered an error while processing your request. Please try again or reach out to us for help.
Placental development. The role of the chorion in the formation of the placenta. The structure and role of the hematoplacental barrier ,for histology