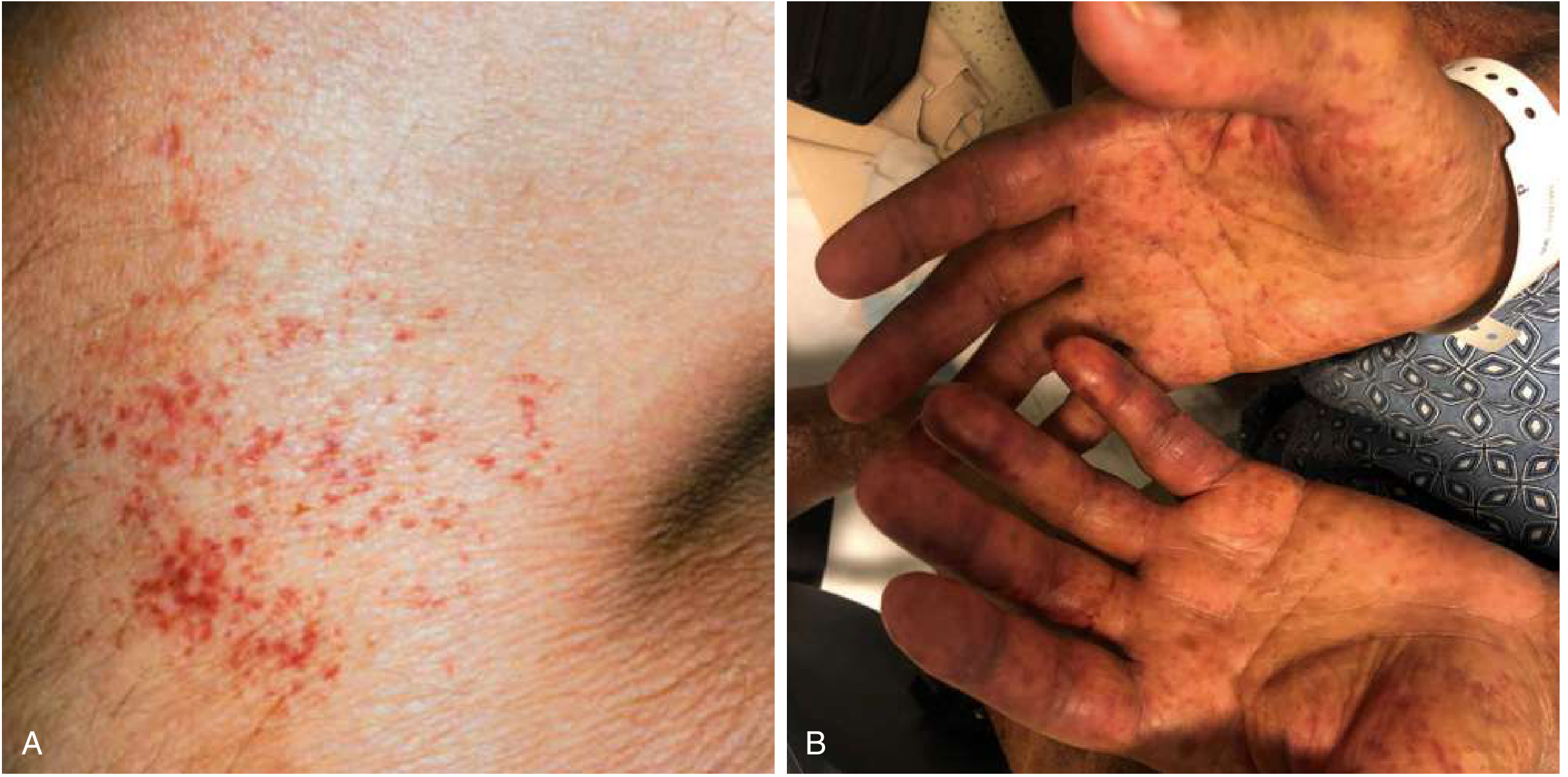
Petechiae
Reading File
Finding Sources
Finding Sources
Searching PubMed
petechiae causes diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I have enough comprehensive information. Here is the full, well-organized answer:
Petechiae
Definition and Morphology
Petechiae are capillary hemorrhages presenting as nonblanching, pinpoint (≤3-4 mm), red, blue, or purple spots resulting from extravasation of blood from small dermal capillaries. They are distinguished from purpura (5-9 mm) and ecchymoses (≥1 cm) by size. The key clinical test is diascopy (glass pressure): petechiae do not blanch, confirming true hemorrhage rather than vascular dilation.
- Shape: round to oval, occasionally targetoid
- Distribution: most often dependent body parts (lower extremities), but may be widespread
- Texture: flat (nonpalpable), unless associated with inflammation
Pathophysiology
Petechiae form by three mechanisms:
- Thrombocytopenia / platelet dysfunction - inadequate platelet plug formation allows capillary bleeding (most common cause)
- Increased intravascular pressure - venous obstruction, Valsalva, violent coughing, or vomiting forces RBCs through capillary walls
- Vascular wall damage - infection, vasculitis, or nutritional deficiency weakens the capillary endothelium
Differential Diagnosis
Causes of Macular Petechiae (≤4 mm)
| Category | Cause |
|---|---|
| Platelet disorder | Thrombocytopenia (platelets <50,000/µL) - ITP, drug-induced, hematologic malignancy |
| Platelet dysfunction | Renal or hepatic insufficiency, von Willebrand disease |
| Increased venous pressure | Tourniquet, retching, violent coughing (confined above nipple line) |
| Nutritional | Vitamin C deficiency (scurvy) |
| Vascular/pigmented | Schamberg disease (pigmented purpuric dermatitis) - idiopathic capillaritis; cayenne-pepper petechiae on lower legs |
| Dysproteinemia | Waldenström macroglobulinemia |
| Infectious | Meningococcemia, Rocky Mountain spotted fever, pneumococcal bacteremia, parvovirus |
The Critical "Fever + Petechiae" Scenario
This combination demands urgent evaluation. The differential includes:
- Neisseria meningitidis (meningococcemia) - most feared; incidence ~7-11% in hospitalized patients with fever + petechiae
- Disseminated intravascular coagulation (DIC)
- Rocky Mountain spotted fever (RMSF)
- Streptococcus pyogenes bacteremia
- Pneumococcal bacteremia
- Henoch-Schönlein purpura (IgA vasculitis) - notably WITHOUT thrombocytopenia
- Leukemia
- Various viral infections
Mechanical petechiae from vomiting/coughing are limited to the skin above the nipple line. Petechiae from serious bacterial infection (SBI) have any distribution.
Palpable vs. Nonpalpable: A Key Distinction
| Feature | Nonpalpable | Palpable |
|---|---|---|
| Mechanism | Simple capillary extravasation (thrombocytopenia, platelet dysfunction, pressure) | Inflammatory vessel wall damage (vasculitis) |
| Key causes | ITP, Schamberg, scurvy, mechanical | Leukocytoclastic vasculitis, IgA vasculitis, meningococcemia, RMSF, DIC |
| Urgency | Variable | Potentially life-threatening |
Palpable purpura/petechiae always require evaluation for vasculitis and, in the right context, infectious causes - Goldman-Cecil Medicine
Specific Conditions
Schamberg Disease
The most common cause of isolated petechiae in adults. Idiopathic capillaritis causing cayenne-pepper-colored petechiae on lower legs with yellow-brown hyperpigmented patches. Benign, but new crops appear over time. Treated with topical steroids, ascorbic acid 500 mg twice daily ± rutoside 50 mg twice daily.
ITP (Immune Thrombocytopenic Purpura)
Typically presents as mild mucocutaneous bleeding and petechiae or incidental thrombocytopenia. Bleeding risk highest when platelets <30 × 10⁹/L.
Meningococcemia
Classic petechial/purpuric rash in a febrile, ill-appearing patient. The lesions may rapidly evolve into confluent purpura fulminans. This is a medical emergency.
RMSF
Petechiae typically appear after 3-5 days of fever; may start on wrists/ankles and spread centrally, including palms and soles.
Forensic context
Petechial hemorrhages in conjunctivae/sclerae are classical in asphyxial deaths from strangulation (also called Tardieu spots on visceral surfaces), though they are nonspecific and may be seen in many non-fatal conditions.
Diagnostic Workup
- CBC with differential - platelet count (thrombocytopenia is the most common cause)
- Peripheral blood smear - platelet morphology, blast cells, schistocytes (TTP/HUS)
- Coagulation studies - PT, PTT, fibrinogen, D-dimer (DIC)
- Blood culture if febrile (bacteremia, meningococcemia)
- CRP - elevated in SBI
- Skin biopsy - determines vessel size involved, degree of inflammation, type of damage (leukocytoclastic vs. granulomatous), presence of organisms or occlusions
- Direct immunofluorescence - identifies IgA deposits (IgA vasculitis), immune complexes on vessel walls
In children with fever + petechiae: abnormal WBC (<5,000 or >15,000/mm³) or abnormal coagulation are predictive of invasive bacteremia - admit and treat empirically until cultures result. Well-appearing children with normal WBC, CRP, and coagulation can be discharged with close follow-up. - Rosen's Emergency Medicine
Treatment
Treatment is directed at the underlying cause. Supportive care includes local wound care and prevention of secondary infection for superficial lesions.
Sources: Symptom to Diagnosis, 4th ed. | Goldman-Cecil Medicine | Rosen's Emergency Medicine | Fitzpatrick's Dermatology 5th ed.
Ecchymoses
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
ecchymoses bruising coagulopathy diagnosis
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Ecchymoses
Definition and Morphology
Ecchymoses (singular: ecchymosis) are subcutaneous hemorrhages ≥1 cm in diameter, commonly called bruises. They result from extravasation of blood from small vessels into the dermis and subcutaneous tissue, producing nonblanching discoloration. They differ from petechiae (<4 mm) and purpura (4-10 mm) by size alone, though the underlying mechanisms overlap.
- Shape: typically geometric, rectangular, or linear when trauma-induced; irregular when from systemic disease
- Color evolution: red/purple → blue-green → yellow-brown, reflecting sequential degradation of hemoglobin to biliverdin to bilirubin/hemosiderin
- Texture: flat (nonpalpable); palpable when blood volume is large enough to form a hematoma
- Blood is typically resorbed within ~2 weeks; postinflammatory hyperpigmentation may persist
Pathophysiology: Two Broad Mechanisms
Ecchymoses require blood to escape vessel walls. This occurs via two main routes:
1. Procoagulant defects
Inadequate clotting factors or platelets fail to seal micro-tears. Even minor trauma leads to disproportionate bleeding.
2. Poor dermal connective tissue support
The dermis normally anchors and buttresses capillaries. When this scaffolding is lost, minor mechanical stress ruptures vessels that would otherwise hold. Coagulation may be entirely normal.
Differential Diagnosis of Macular Ecchymoses (≥1 cm)
Procoagulant Defects
| Cause | Mechanism |
|---|---|
| Anticoagulant therapy (warfarin, heparin, DOACs) | Impairs clotting cascade |
| Hepatic insufficiency | Reduced synthesis of factors II, V, VII, IX, X, fibrinogen |
| Vitamin K deficiency | Impairs carboxylation of factors II, VII, IX, X |
| Disseminated intravascular coagulation (DIC) | Consumption of clotting factors + platelets |
| Thrombocytopenia | Insufficient platelet plug formation |
| Platelet function defects | Von Willebrand disease, medication-induced (ASA, NSAIDs), uremia |
Poor Dermal Support
| Cause | Features |
|---|---|
| Solar (actinic/senile) purpura | Aging + UV damage degrades dermal connective tissue; ecchymoses on extensor forearms; benign, cosmetically bothersome |
| Corticosteroid purpura | Topical or systemic steroids cause dermal atrophy; can be widespread with Cushing's syndrome |
| Vitamin C deficiency (scurvy) | Impaired collagen synthesis weakens perivascular connective tissue |
| Systemic amyloidosis | AL or ATTR amyloid deposits weaken vessel walls; "pinch purpura" around eyes classic |
| Ehlers-Danlos syndrome | Defective fibrillar collagen; skin velvety and thin, bruises easily from childhood; joint hypermobility, pseudotumors |
Miscellaneous
- Trauma - most common cause overall; geometric/linear shape, trauma-prone sites (dorsal hand, shin, lateral thigh)
- Gardner-Diamond syndrome (autoerythrocyte sensitization) - recurrent painful ecchymoses on palmar surface of fingers; predominantly women; Doppler evaluation negative
- Papular purpuric gloves and socks syndrome
Senile (Actinic/Solar) Purpura - A Common Entity
Senile purpura is worth detailing as it is the most frequent cause of ecchymoses in older adults:
- Mechanism: Age-related skin thinning + chronic UV damage degrades dermal connective tissue, leaving microvasculature unsupported and fragile. Minor bumps rupture venules.
- Distribution: Extensor surfaces of forearms and hands (sun-exposed areas)
- Appearance: Bright purple-red ecchymoses that resolve over 1-2 weeks, leaving brown hyperpigmentation from hemosiderin
- Aggravating factors: Aspirin, anticoagulants (very common in the elderly), NSAIDs
- Coagulation studies: Normal
- Treatment: No specific treatment; vitamin C and topical retinoids may help maintain dermal collagen. The condition is benign.
"Age-related skin thinning and sun-induced damage of the connective tissue of the dermis results in inadequate support and increased fragility of the microvasculature. As a result, minor trauma of aged photodamaged skin can lead to vessel rupture." - Fitzpatrick's Dermatology
Distinguishing Ecchymoses from Petechiae/Purpura
| Feature | Petechiae | Purpura | Ecchymoses |
|---|---|---|---|
| Size | ≤4 mm | 4-10 mm | >10 mm (≥1 cm) |
| Most common cause | Thrombocytopenia | Vasculitis / thrombocytopenia | Trauma / anticoagulation / dermal fragility |
| Shape | Round, pinpoint | Variable | Geometric if traumatic; irregular if systemic |
| Blanching | No | No | No |
| Palpable? | No | Sometimes (vasculitis) | Sometimes (hematoma) |
Coagulation Factor Defects vs. Platelet Defects: A Pattern Distinction
- Platelet disorders (including ecchymoses) - mucocutaneous bleeding, petechiae, purpura; bleeding after superficial cuts; prolonged bleeding time
- Coagulation factor defects (hemophilia, etc.) - deep tissue bleeding, hemarthrosis, muscle hematomas; bleeding after surgery/trauma; prolonged PT or aPTT
- Ecchymoses can occur in both, but large deep ecchymoses without clear trauma in a young patient should raise suspicion for hemophilia or other factor deficiencies
Diagnostic Workup
- History: trauma exposure, medications (anticoagulants, steroids, ASA), age, sun exposure, alcohol/liver disease, family history of bleeding
- CBC with platelets - thrombocytopenia
- PT/INR - extrinsic pathway (warfarin effect, liver disease, vitamin K deficiency)
- aPTT - intrinsic pathway (hemophilia, heparin)
- Fibrinogen + D-dimer - DIC
- Liver function tests - hepatic insufficiency
- Vitamin C level if scurvy suspected (perioral bleeding, perifollicular hemorrhage, gingival changes)
- Peripheral smear - schistocytes (TTP/HUS), blast cells
- Skin biopsy - when vascular disease or amyloidosis suspected; Congo red staining for amyloid
Treatment
Treatment is directed at the underlying cause:
- Reverse anticoagulation if excessive (vitamin K, PCC, FFP as appropriate)
- Treat DIC (manage precipitant, supportive)
- Corticosteroid purpura: minimize steroid dose; photoprotection for solar purpura
- Vitamin C replacement for scurvy (rapid resolution)
- Platelet transfusion or ITP treatment for platelet-mediated cases
Sources: Goldman-Cecil Medicine | Fitzpatrick's Dermatology 5th ed. | Dermatology 2-Volume Set 5e | Harrison's Principles of Internal Medicine 22e | Robbins & Cotran Pathologic Basis of Disease | Symptom to Diagnosis, 4th ed.
This is a shared conversation. Sign in to Orris to start your own chat.