Kindly provide detailed theory of 1. Types of incision used in Tympanomastoid surgery with photo 2. Types of endoscopic Tympanomastoid surgery
Reading File
Finding Sources
Finding Sources
Searching the Web
types of incisions tympanomastoid surgery postauricular endaural
Finding Sources
Finding Sources
Reading Web Page
https://entokey.com/incisions-and-approaches
Searching the Web
endoscopic tympanomastoid surgery types transcanal fully endoscopic TEES classification 2024
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11456086
I now have comprehensive information from multiple sources. Let me compile the full detailed response.
Tympanomastoid Surgery: Incisions & Endoscopic Approaches
PART 1: TYPES OF INCISIONS IN TYMPANOMASTOID SURGERY
The three standard surgical approaches to the external auditory canal, middle ear, and mastoid are: (1) Transcanal, (2) Endaural, and (3) Postauricular. For extended access to the temporal base, modified variants exist. Each incision has specific indications based on the extent of disease and the surgical goal.
1. TRANSCANAL INCISION (Transcanal Tympanomeatal Incision)
Description:
The transcanal approach involves incisions made entirely within the external auditory canal (EAC) without any external skin incision on the auricle or behind the ear. The tympanomeatal flap is raised from within the canal itself.
Types of tympanomeatal incisions:
- Posterior tympanomeatal incision: A curved incision made in the posterior canal skin, 5-6 mm lateral to the tympanic annulus, running from approximately 12 o'clock to 6 o'clock posteriorly. The skin-periosteum flap is elevated forward to expose the posterior tympanic cavity.
- Anteriorly based incision (used in stapedectomy): A tympanomeatal incision that is elevated anteriorly to expose the oval window niche.
Indications:
- Tympanoplasty for posterior perforations
- Myringoplasty (small central perforations)
- Ossiculoplasty
- Stapedectomy/stapedotomy
- Excision of small glomus tympanicum tumors
- Insertion of ventilating tubes
- Exploratory tympanotomy for limited disease
Advantages:
- No external skin incision - no scar
- Quicker recovery, less postoperative pain
- Shorter operative time
- Ideal for confined middle ear disease
Limitations:
- Anterior canal wall bulge may obscure anterior quadrant of tympanic membrane
- Does NOT provide mastoid access
- Limited exposure; unsuitable for extensive cholesteatoma or mastoid disease
- Technically difficult in narrow EACs
2. ENDAURAL INCISION
The endaural incision gives access to the EAC, tympanic membrane, epitympanum, and can be extended for limited mastoid access (with Heermann extension).
Structure of the Endaural Incision (Three Segments):

The three segments are:
- Circumferential segment - a curved incision inside the EAC around the superior circumference
- Intercartilaginous segment - passes between the helical crus and the tragus (the meatus)
- Vertical limb (superior limb) - extends upward into the temporal region to expose the temporalis fascia and linea temporalis
Heermann Extension: An additional superior incision that extends upward into the temporal scalp, greatly expanding access to the mastoid cortex.
Indications:
- Canalplasty (e.g., for exostoses)
- Tympanoplasty for anterior perforations (where postauricular access risks anterior canal collapse)
- Anterior atticotomy
- Total drum replacement
- Limited mastoidectomy (with Heermann extension)
- Preferred when abnormally small EAC meatus prevents good transcanal access
Advantages:
- Better exposure than transcanal for anterior tympanic membrane
- Access to temporalis fascia for graft harvesting
- Avoids the risk of anterior auricle displacement (which can cause collapsing canal) seen with postauricular incision
- Scar is concealed in the preauricular/intertragal notch region
Limitations:
- The scar sits in the intercartilaginous notch and can be visible
- More limited posterior mastoid exposure compared to postauricular
- Does not easily allow the wide field needed for extensive mastoid surgery
3. POSTAURICULAR INCISION
This is the workhorse incision of tympanomastoid surgery and the most widely used approach for mastoidectomy, tympanomastoidectomy, and any operation requiring access to the full tympanomastoid compartment.

Surgical technique:
- A C-shaped incision is made approximately 1 cm posterior to the postauricular crease/sulcus, running from the helical rim superiorly down to the mastoid tip inferiorly
- Care is taken NOT to place the incision in the sulcus itself (leads to poor healing and deepening of the sulcus)
- In young children, where the mastoid tip is undeveloped and the facial nerve exits more laterally, the inferior limb is taken further posterior to protect the facial nerve
- The incision goes through skin and subcutaneous fat to the layer of loose areolar tissue overlying the superficial temporalis fascia
- This loose areolar tissue layer is harvested for tympanoplasty grafting
- A T-shaped or inferiorly based periosteal incision is then made along the linea temporalis to expose the mastoid cortex
(Shambaugh Surgery of the Ear - Incisions chapter; Cummings Otolaryngology, Ch. 143)
Indications:
- Tympanomastoidectomy (canal-wall-up and canal-wall-down)
- Cortical (simple) mastoidectomy
- Canal-wall-up mastoidectomy for cholesteatoma
- Canal-wall-down mastoidectomy
- Tympanoplasty for anterior perforations
- Hypotympanotomy
- Cochlear implantation
- Any surgery requiring full access to the tympanomastoid compartment
Advantages:
- Excellent, wide surgical exposure of the entire mastoid and tympanomastoid compartment
- Generous graft harvest (temporalis fascia, areolar tissue)
- Allows T-shaped periosteal flap for obliteration
- Safe, familiar approach with established anatomical landmarks
Limitations:
- Longer operative time and recovery vs. transcanal
- External scar (usually hides well in the postauricular fold)
- Risk of anterior auricular displacement causing collapsing canal if dissection is too aggressive anteriorly
- More postoperative pain and swelling
4. MODIFIED POSTAURICULAR INCISION
An extension of the standard postauricular incision, curved more superiorly toward the temporal scalp. Used for:
- Cochlear implantation (modified C-shape, 3-4 cm behind the postauricular fold)
- Access to the temporal fossa
- Extended procedures involving the sigmoid sinus area
5. EXTENDED POSTAURICULAR INCISION
A large postauricular incision extending into the upper neck, allowing access to:
- The tympanomastoid compartment
- Upper neck
- Infratemporal fossa
6. PREAURICULAR (LATERAL FACIAL) INCISION
Used for access to:
- Infratemporal fossa
- Upper neck
- Middle fossa surface of temporal bone (with superior extension)
7. POSTAURICULAR TRANSTEMPORAL INCISION
Used for middle fossa approach to access the superior surface of the temporal bone, internal auditory canal, and skull base.
8. SUBOCCIPITAL INCISION
Used for retrosigmoid/suboccipital access to the posterior fossa and cerebellopontine angle.
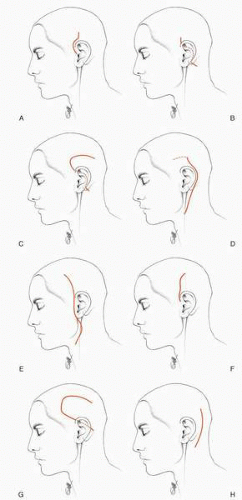
The image below shows the full range of incisions in temporal bone and lateral skull base surgery:
Summary Table of Incisions:
| Incision | Access | Typical Procedures |
|---|---|---|
| Transcanal tympanomeatal | Tympanic membrane, posterior middle ear | Type I tympanoplasty, stapedectomy, ossiculoplasty, ventilating tubes |
| Endaural | EAC, tympanic membrane, limited epitympanum | Canalplasty, anterior tympanoplasty, atticotomy, limited mastoidectomy |
| Postauricular | Full tympanomastoid compartment | Mastoidectomy, tympanomastoidectomy, CWU/CWD surgery, cochlear implant |
| Modified postauricular | Tympanomastoid + temporal fossa | Cochlear implantation, extended skull base |
| Extended postauricular | Tympanomastoid + upper neck + infratemporal fossa | Infratemporal surgery |
(Cummings Otolaryngology Table 9.1; Shambaugh Surgery of the Ear, Ch. 30)
PART 2: TYPES OF ENDOSCOPIC TYMPANOMASTOID SURGERY
The evolution of endoscopic ear surgery (EES) over the past three decades has introduced a spectrum of approaches ranging from endoscope-assisted inspection to fully endoscopic canal-wall-down procedures. The central philosophy is using the natural ear canal as the surgical corridor, bypassing the narrowest portion of the EAC to reach the middle ear directly.
BACKGROUND AND RATIONALE
The microscope provides excellent magnification but requires line-of-sight visualization, forcing surgeons to drill through the mastoid to reach areas such as the sinus tympani, facial recess, and anterior epitympanum. The endoscope, by contrast, provides a wide-angle, panoramic view and allows surgeons to look "around corners" using angled lenses (typically 0°, 30°, and 45° Hopkins rod endoscopes, 2.7-4 mm diameter). Advances in HD camera technology have made real-time 4K-quality imaging possible. (Cummings Otolaryngology, Ch. 144)
CLASSIFICATION OF ENDOSCOPIC EAR SURGERY
The Massachusetts Eye and Ear Infirmary (MEEI) TEES Classification System is the most widely used framework:
| Class | Description |
|---|---|
| Class 1 | Endoscope used for inspection only; main surgery with microscope |
| Class 2 | Endoscope-assisted surgery (endoscope + microscope combined) |
| Class 3 | Totally Endoscopic Ear Surgery (TEES) - no external incision, no microscope |
TYPE 1: ENDOSCOPIC INSPECTION / OTOENDOSCOPY (Class 1)
Description:
The endoscope is passed transtympanically (through the tympanic membrane) or transcanally to inspect the middle ear after or alongside microscopic surgery. No active dissection is performed with the endoscope.
Historical context:
Poe introduced transtympanic endoscopy in the 1990s through a myringotomy. Thomassin and colleagues used endoscopic inspection at the end of canal-wall-up mastoidectomy procedures to verify the degree of cholesteatoma eradication. (Shambaugh Surgery of the Ear, Ch. 20)
Role:
- Second-look procedures after primary mastoidectomy
- Inspection of sinus tympani, facial recess, and anterior epitympanum post-microscopic dissection
- Reduces residual cholesteatoma rates: Thomassin showed residual disease dropped from 47.7% to 5.5% by adding endoscopic inspection to canal-wall-up mastoidectomy
Endoscope used: 1.9 mm or 2.7 mm, 0° and 30° Hopkins rod endoscope; passed through speculum into the EAC and through the tympanic membrane.
TYPE 2: ENDOSCOPE-ASSISTED EAR SURGERY (Class 2)
Description:
A combined approach where the microscope provides the primary surgical field (usually through a postauricular approach), and the endoscope is used selectively to inspect or dissect areas not accessible to the microscope - particularly the sinus tympani, retrotympanum, hypotympanum, and anterior epitympanum.
Subtypes:
a) Endoscope-assisted canal-wall-up (CWU) tympanomastoidectomy:
The standard postauricular CWU mastoidectomy is performed under the microscope. At key steps (before closure, or when dissecting toward the sinus tympani), an angled endoscope is introduced either through the EAC or through the mastoid antrum to look into areas the microscope cannot reach.
b) Endoscope-assisted canal-wall-down (CWD) mastoidectomy:
Yung demonstrated that in CWD mastoidectomy, an endoscope revealed sinus tympani disease in more than one-third of cases that would otherwise have been missed. (Scott-Brown's Otorhinolaryngology, Vol. 2, Ch. 10)
c) Endoscope-guided second-look mastoidectomy:
McKennan described a small postauricular stab incision through which an endoscope inspects the mastoid cavity to look for residual cholesteatoma at second-look procedures, avoiding a full re-exploration. A transcanal approach with angled endoscopes is also preferred for second-look procedures focused on the epitympanum and sinus tympani. (Shambaugh, Ch. 20)
Advantages over pure microscopy:
- Reduces residual disease rates comparable to CWD results while preserving the canal wall
- Allows visualization of sinus tympani, retrofacial recess, anterior epitympanum, and Eustachian tube orifice without additional bone removal
- Reduces need for second-stage procedures
TYPE 3: TOTALLY ENDOSCOPIC EAR SURGERY (TEES) - Class 3
Description:
The entire operation is performed endoscopically through the EAC without any external incision. The endoscope and surgical instruments are introduced through the meatus, and all dissection, graft placement, and reconstruction is performed under endoscopic guidance on a video monitor.
Key principle: The transcanal approach bypasses the narrowest part of the canal and reaches the tympanic membrane directly. A tympanomeatal flap is raised under the endoscope, and the entire middle ear is accessed through this single natural corridor.
Endoscope held in nondominant hand; instruments in dominant hand (one-handed technique).
Patient selection criteria:
| Favorable | Unfavorable |
|---|---|
| Normal/generous EAC diameter | Stenotic EAC |
| Disease limited to tympanic membrane and middle ear | Mastoid extension of disease |
| Cholesteatoma not extending posterior to dome of lateral SCC | Extension posterior to lateral SCC dome |
| No prior canal-wall-down surgery | Previous CWD cavity |
(Cummings Otolaryngology, Table 144.1)
Specific TEES operations:
A. Endoscopic Myringoplasty / Type I Tympanoplasty
- First described in 1992 (Tarabichi)
- Graft take rates of ~92%, air-bone gap closure to <10 dB in 83%
- Equivalent outcomes to microscope-assisted cases
- Graft placed as underlay (fat, fascia, or perichondrium) via transcanal route
B. Endoscopic Tympanoplasty with Ossiculoplasty
- Visualization of the oval and round window regions is superior to the microscope
- Ossiculoplasty with PORP/TORP or autologous incus interposition performed entirely transcanally
- Tensor fold can be opened endoscopically to restore ventilation pathways
C. Endoscopic Atticotomy / Epitympanotomy
- Transcanal endoscopic atticotomy (TEA) for pars flaccida retraction pockets and limited attic cholesteatoma
- The scutum is partially removed to expose the lateral epitympanum and malleus head
- The anterior and posterior epitympanum (separated by the "cog" - a bony septum) can be fully explored
- Cartilage reconstruction of the attic wall follows disease clearance
- Tarabichi described this in 168 patients with retraction pockets/cholesteatoma; recurrence rate 7%
D. Endoscopic Transcanal Cholesteatoma Surgery
- For cholesteatoma confined to mesotympanum, epitympanum, facial recess, sinus tympani, hypotympanum, and Eustachian tube - endoscopic access is excellent
- Cholesteatoma involving the sinus tympani (the most common site of recurrence) is particularly accessible, as the endoscope can look directly into this recess
- Retraction pocket dissected step-by-step through the middle ear following the matrix around ossicles and ligaments
- For cholesteatoma with attic + antral extension (without lateral SCC extension), Class 3 TEES has been successfully performed
Key evidence: In a study of 25 patients with squamosal-type COM treated with Class 3 TEES, mean operative time was 118 minutes, with no conversion to microscopic surgery and no patients requiring additional mastoidectomy. (PMC11456086)
E. Endoscopic Retrotympanotomy (Transcanal Endoscopic Approach to Sinus Tympani)
- The sinus tympani, located posterior and inferior to the stapes and facial nerve, is the most difficult area to visualize with the microscope
- An angled endoscope (30° or 45°) provides direct visualization and access without facial recess dissection
- The retrofacial approach via endoscope is far less traumatic than traditional microscopic techniques
F. Endoscopic Second-Look Procedures
- A tympanomeatal flap is elevated transcanally, providing access for angled endoscope inspection of the entire middle ear
- 75% of second-stage procedures at Shambaugh's institution were accomplished via transcanal endoscopic approach (Shambaugh Surgery of the Ear)
TYPE 4: ENDOSCOPIC-ASSISTED MASTOIDECTOMY / HYBRID APPROACHES
For cholesteatoma extending into the mastoid beyond the dome of the lateral semicircular canal, a purely transcanal approach is insufficient. In these cases, a hybrid approach combines:
- Postauricular (microscopic) mastoidectomy for the mastoid component
- Transcanal endoscopic approach for middle ear and deep recesses
This eliminates the need for canal-wall-down surgery in many cases because the endoscope provides adequate access to the sinus tympani, facial recess, and epitympanum via the canal - reducing the morbidity of open mastoid cavities. (Cummings Otolaryngology, Ch. 144)
TYPE 5: TOTALLY ENDOSCOPIC CANAL-WALL-DOWN SURGERY
In experienced hands, even canal-wall-down (open cavity) mastoidectomy can be performed endoscopically by combining a retroauricular endoscopic access with transcanal visualization. This remains a niche technique practiced at high-volume TEES centers.
ADVANTAGES OF ENDOSCOPIC OVER MICROSCOPIC APPROACHES (Summary)
| Parameter | Endoscopic (TEES) | Microscopic |
|---|---|---|
| External incision | None (Class 3) | Required (postauricular/endaural) |
| Visibility of sinus tympani | Excellent (direct) | Poor (requires facial recess drill-out) |
| Visualization of epitympanum | 270° panoramic | Line of sight only |
| Postoperative pain | Significantly less | More |
| NSAID use | 1.3 pills/week | 5.5 pills/week (p<0.001) |
| Hospital stay | Earlier discharge | Longer |
| Canal-wall preservation | More likely | More likely to require CWD |
| Learning curve | Steep (one-handed technique) | Established |
| Mastoid disease | Requires additional access | Full exposure |
KEY LIMITATIONS OF ENDOSCOPIC APPROACH
- One-handed technique - the non-dominant hand holds the endoscope; only one instrument at a time in the dominant hand (no bimanual dissection)
- Thermal risk - prolonged endoscope use can cause caloric vertigo or thermal injury (limit endoscope in situ to 45-60 seconds with 300W light; use 150W to avoid symptoms)
- Hemostasis - any bleeding obscures the lens; meticulous hemostasis with epinephrine pledgets is mandatory
- Mastoid disease - disease extending posterior to the dome of the lateral SCC requires mastoidectomy and microscopic visualization
- Narrow EAC - stenotic canals preclude the transcanal approach
SOURCES
- Shambaugh Surgery of the Ear, Ch. 20: Middle Ear Endoscopic Surgery (pp. 385-396)
- Cummings Otolaryngology Head and Neck Surgery (7th Ed.), Ch. 143: Mastoid Obliteration; Ch. 144: Middle Ear Endoscopic Surgery (Dedmon, Marchioni, Rivas)
- Cummings Otolaryngology, Ch. Totally Endoscopic Ear Surgery for Cholesteatoma (pediatric)
- Scott-Brown's Otorhinolaryngology H&N Surgery Vol. 2, Ch. 10: Endoscopic tympanoplasty, retraction pockets, mastoid surgery
- EntoKey: Incisions and Approaches
- Stanford Oto Surgery Atlas: Endaural Incision
- PMC11456086: Transcanal Endoscopic Management of Squamosal COM (TEES Class 3, 2024)
- ENTtoday: Endoscopic Ear Surgery Advancements (2025)
This is a shared conversation. Sign in to Orris to start your own chat.