Notes on heartfailure with diagram mnemonicsfor mbbbs 4 year university exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material. Let me compile everything into detailed, mnemonic-rich exam notes.
Heart Failure - Complete MBBS Exam Notes
Quick Reference Mnemonics
1. DEFINITION
Heart failure (HF) is a clinical syndrome in which the heart cannot pump blood to adequately meet the metabolic demands of peripheral tissues, or can do so only at elevated filling pressures.
"The end stage of many forms of chronic heart disease." - Robbins & Cotran Pathologic Basis of Disease
2. CLASSIFICATION
A. By Ejection Fraction (EF)
| Type | EF | Mechanism | Mnemonic |
|---|---|---|---|
| HFrEF (Systolic HF) | < 40% | Impaired contraction | Systolic = Squeeze fails |
| HFmrEF (Mid-range) | 40-49% | Mixed | Middle = Mixed |
| HFpEF (Diastolic HF) | ≥ 50% | Impaired relaxation/filling | Preserved = Pump works but Poor filling |
HFpEF patients: tend to be older, female, obese, hypertensive, diabetic
B. ACC/AHA Stages (Progressive - CANNOT go backwards)
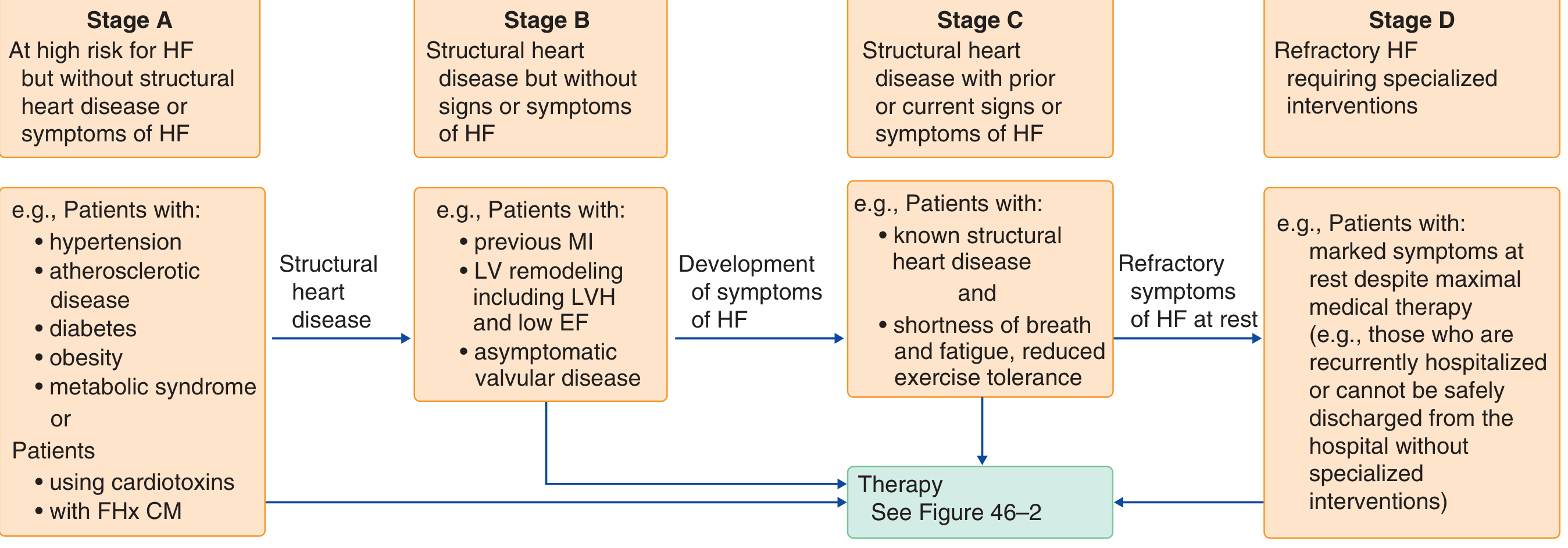
Mnemonic: "At Best, Clinicians Defeat HF"
| Stage | Description | Example |
|---|---|---|
| A | At risk, NO structural disease | HTN, DM, obesity |
| B | structural disease, NO symptoms | Previous MI, LVH, low EF |
| C | structural disease + symptoms | SOB + known heart disease |
| D | refractory HF despite max therapy | Recurrently hospitalized |
C. NYHA Functional Classification (Fluctuates up and down)
Mnemonic: "No Symptoms, Slight, Marked, Rest" = NSSMR or just count 1-4
| Class | Symptoms |
|---|---|
| I | No symptoms with ordinary activity |
| II | Slight limitation; comfortable at rest |
| III | Marked limitation; comfortable only at rest |
| IV | Symptoms at rest; any activity causes discomfort |
3. ETIOLOGY
Mnemonic: "CHIVATO Pres" (causes of HF)
| Letter | Cause |
|---|---|
| C | Coronary artery disease (70% of cases in developed world) |
| H | Hypertension |
| I | Idiopathic dilated cardiomyopathy |
| V | Valvular heart disease |
| A | Alcohol, Anthracyclines (cardiotoxins) |
| T | Thyroid disease (high-output) |
| O | Obesity, anemia, AV fistulae (high-output states) |
| Pres | Pressure/volume overload |
"Rheumatic heart disease remains a major cause in Africa and Asia." - Braunwald's Heart Disease
4. PATHOPHYSIOLOGY
The 4 Major Systems Involved
Mnemonic: "HVKN" - "Has Very Keen Neurons"
- H - Heart itself (cardiomyopathy of overload)
- V - Vasculature (increased afterload/preload)
- K - Kidney (RAAS activation, fluid retention)
- N - Neurohumoral circuits (SNS, RAAS, ANP)
Compensatory Mechanisms (initially helpful, eventually harmful)
Mnemonic: "FAN-H"
| Mechanism | Description |
|---|---|
| F - Frank-Starling | Increased filling → stretch → more forceful contraction |
| A - Adrenergic activation | NE raises HR, contractility, vascular resistance |
| N - Natriuretic peptides | ANP/BNP released; cause diuresis & vasodilation |
| H - Hypertrophy | Myocardial adaptation to increased workload |
Types of Hypertrophy
Mnemonic: "Pressure = Parallel (concentric); Volume = Series (eccentric)"
| Type | Stimulus | Sarcomere assembly | Result |
|---|---|---|---|
| Concentric | Pressure overload (HTN, AS) | Parallel | Thick wall, small cavity |
| Eccentric | Volume overload (MR, AR) | In series | Dilated chamber |
Forward vs. Backward Failure
BACKWARD FAILURE FORWARD FAILURE
(blood backs up) (inadequate output)
| |
Left: pulmonary congestion Low CO → organ hypoperfusion
Right: systemic/portal congestion Prerenal azotemia
Hypoxic encephalopathy
5. LEFT-SIDED HEART FAILURE
Mnemonic: "DOPODA" (pulmonary symptoms)
| Symptom/Sign | Mechanism |
|---|---|
| D - Dyspnea on exertion | Pulmonary congestion |
| O - Orthopnea | Redistribution of fluid on lying down |
| P - PND (paroxysmal nocturnal dyspnea) | Same as orthopnea, nocturnal |
| O - Output low (fatigue, weakness) | Reduced CO |
| D - Dilated heart (cardiomegaly) | Ventricular remodeling |
| A - Added sounds (S3/S4), AF risk | Volume overload, atrial dilation |
Lung findings (progressive):
- Perivascular/interstitial edema
- Alveolar septal widening
- Alveolar fluid + "heart failure cells" (hemosiderin-laden macrophages)
- Fine basal crepitations (rales)
- Pleural effusion (usually serous)
"Heart failure cells are hemosiderin-laden macrophages - telltale signs of previous pulmonary edema." - Robbins
6. RIGHT-SIDED HEART FAILURE
Mnemonic: "JALE + Edema" (Jugular, Ascites, Liver, Edema)
| Feature | Detail |
|---|---|
| J - JVP elevated | Systemic venous congestion |
| A - Ascites | Portal hypertension |
| L - Liver enlarged ("nutmeg liver") | Centrilobular congestion → cardiac cirrhosis |
| E - Edema (dependent) | Pedal/pretibial edema; sacral in bedridden |
| S - Splenomegaly | Congestive, with platelet sequestration |
Most common cause of right HF = LEFT HF (pulmonary hypertension)
Isolated right HF = cor pulmonale (caused by lung disease, pulmonary HTN, PE, OSA)
"Nutmeg liver": red-brown centrilobular zones + tan periportal zones on cut section.
7. DIAGNOSIS
Diagnostic Flowchart (Goldman-Cecil Medicine)
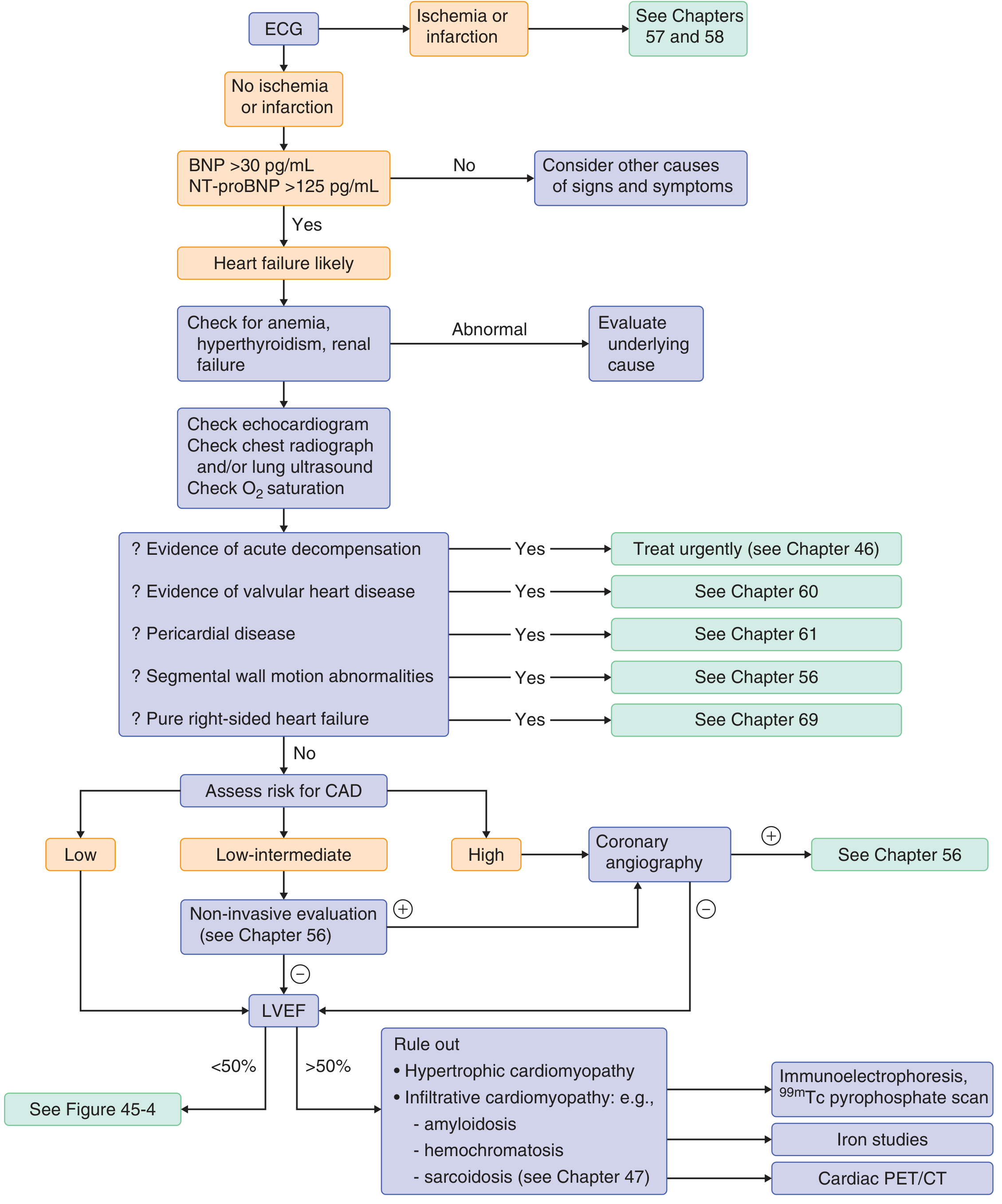
Key steps:
- ECG (rule out ischemia/infarction)
- BNP/NT-proBNP: BNP >30 pg/mL or NT-proBNP >125 pg/mL = HF likely
- Check for secondary causes: anemia, hyperthyroidism, renal failure
- Echo + CXR + O2 saturation
- Assess LVEF: <50% vs ≥50% directs further workup
Biomarkers - BNP/NT-proBNP
Mnemonic: "BNP = Bad News Peptide" - goes up when ventricles are stressed
| Marker | Source | Half-life | Cutoff |
|---|---|---|---|
| BNP | Ventricular myocytes | 20 min | >30 pg/mL (non-acute) / >100 pg/mL (acute) |
| NT-proBNP | Cleavage product | Longer (hours) | >125 pg/mL |
- BNP is released in response to ventricular wall tension and stretch
- Provides diagnostic AND prognostic information
- Levels correlate with NYHA class and guide therapy
CXR findings in HF:
Mnemonic: "ABCDE" of pulmonary oedema on CXR
| Letter | Finding |
|---|---|
| A | Alveolar shadowing ("bat wing" / "butterfly" pattern) |
| B | Kerley B lines (horizontal lines at bases = interstitial oedema) |
| C | Cardiomegaly (CTR > 0.5) |
| D | Diversion (upper lobe diversion of blood flow) |
| E | Effusion (pleural) |
8. MANAGEMENT
Overall Framework - By Stage
| Stage | Goals | Treatment |
|---|---|---|
| A | Risk reduction | Treat HTN, DM, obesity, stop cardiotoxins |
| B | Prevent HF onset | ACEi/ARB, beta-blocker if prior MI |
| C | Symptom relief + prevent progression | Full HFrEF regimen below |
| D | Symptom control | Advanced therapies (VAD, transplant, palliative care) |
The "Fantastic Four" Disease-Modifying Drugs in HFrEF
Mnemonic: "ABMS" or "A Beautiful Medical Strategy"
| Drug class | Key drug(s) | Benefit |
|---|---|---|
| A - ACEi/ARNI | Enalapril / Sacubitril-Valsartan | Reduces mortality ~20-25% |
| B - Beta-blocker | Carvedilol, Bisoprolol, Metoprolol succinate | Reduces mortality ~34% |
| M - MRA | Spironolactone, Eplerenone | Reduces mortality ~30% |
| S - SGLT2 inhibitor | Dapagliflozin, Empagliflozin | Reduces HF hospitalisation + death |
Note: ARNI (sacubitril-valsartan) is preferred over ACEi in symptomatic HFrEF when tolerated.
Diuretics (for fluid overload - symptom relief, NOT mortality benefit)
Mnemonic: "FLAT"
| Drug | Class | Use |
|---|---|---|
| F - Furosemide | Loop diuretic | First line for oedema |
| L - Loop diuretics (general) | All loop agents | Most potent diuresis |
| A - Add thiazide (metolazone) | Sequential nephron blockade | Diuretic resistance |
| T - Torsemide | Loop, better oral bioavailability | Alternative to furosemide |
Additional Agents
| Drug | Indication | Notes |
|---|---|---|
| Digoxin | Symptomatic HF, AF + HF | Reduces hospitalization; no mortality benefit |
| Hydralazine + ISDN | African Americans; ACEi-intolerant | Mortality benefit in Black patients |
| Ivabradine (I-channel inhibitor) | HR ≥70 in sinus rhythm on max beta-blocker | Reduces HF hospitalization |
| IV Iron (ferric carboxymaltose) | Iron deficiency (ferritin <100 or 100-300 + TSat <20%) | Improves symptoms, exercise capacity |
Device Therapy
Mnemonic: "CID" = Cardiac Implant Devices
| Device | Indication |
|---|---|
| C - CRT (Cardiac Resynchronization Therapy) | LVEF ≤35%, LBBB, QRS ≥150ms, NYHA III-IV |
| I - ICD (Implantable Cardioverter Defibrillator) | LVEF ≤35%, NYHA II-III, >1 year expected survival |
| D - Diastolic management (lifestyle + medications) | HFpEF |
9. IMPORTANT EXAM FACTS (High-Yield)
Precipitants of Acute Decompensation
Mnemonic: "I FAIL MED"
| Letter | Precipitant |
|---|---|
| I | Infection (especially pneumonia) |
| F | Failure to take medications/dietary non-compliance (high Na) |
| A | Arrhythmias (especially AF) |
| I | Ischemia/MI |
| L | Lifestyle: alcohol, excess fluids |
| M | Medications: NSAIDs, negative inotropes, cardiotoxins |
| E | Embolism (PE) |
| D | Drugs missed (non-compliance) / Diastolic dysfunction worsening |
Prognosis
- Median survival: 1.7 years (men) and 3.2 years (women) - Framingham Study
- 5-year survival only 25% (men) and 38% (women) - worse than many cancers
- BNP level, LVEF, NYHA class, renal function = key prognostic indicators
Key Pathology Facts (Robbins)
| Finding | Significance |
|---|---|
| Heart failure cells | Hemosiderin-laden macrophages in alveoli from previous pulmonary oedema |
| Nutmeg liver | Centrilobular congestion in right HF |
| Cardiac cirrhosis | End-stage right HF with centrilobular fibrosis |
| Concentric hypertrophy | Pressure overload (HTN, AS) |
| Eccentric hypertrophy | Volume overload (AR, MR, dilated CMP) |
10. ONE-PAGE SUMMARY DIAGRAM
HEART FAILURE
|
┌───────────────────┴───────────────────┐
SYSTOLIC (HFrEF) DIASTOLIC (HFpEF)
EF < 40% EF ≥ 50%
Pump can't squeeze Pump can't fill/relax
Dilated chamber Stiff, thick wall
Older men, IHD Older women, HTN/DM
|
┌──────────┴──────────┐
LEFT-SIDED HF RIGHT-SIDED HF
(Pulmonary symptoms) (Systemic symptoms)
Dyspnea, PND, JVP↑, Oedema,
Orthopnoea, Hepatomegaly,
Crepitations, Ascites,
Pulm oedema Nutmeg liver
COMPENSATORY MECHANISMS (FAN-H):
Frank-Starling → RAAS → SNS → Hypertrophy
→ Initially helpful, eventually HARMFUL
TREATMENT (Stage C HFrEF):
"ABMS" = ACEi/ARNI + Beta-blocker + MRA + SGLT2i
+ Diuretics (symptoms) + Device therapy
11. QUICK DRUG TARGETS
| Drug | Mechanism | Target |
|---|---|---|
| ACEi/ARNI | Block RAAS + neprilysin | Prevents remodeling |
| Beta-blocker | Block SNS | Prevents sudden death |
| MRA | Block aldosterone | Prevents fibrosis |
| SGLT2i | Glucosuria → osmotic diuresis + direct cardiac effects | Reduces hospitalisation |
| Furosemide | Block Na/K/2Cl in loop of Henle | Relieve oedema |
| Digoxin | Inhibit Na/K ATPase → ↑Ca → ↑contractility | Symptoms only |
| Ivabradine | Block I(f) funny current | Lower HR |
Sources: Robbins & Cotran Pathologic Basis of Disease (2023); Braunwald's Heart Disease, 2-Vol Set; Goldman-Cecil Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.