Dry socket
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dry socket" OR "alveolar osteitis" management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a thorough overview of dry socket (alveolar osteitis):
Dry Socket (Alveolar Osteitis)

Definition
Dry socket is a localized inflammation of the alveolar bone that occurs when the blood clot normally present in an extraction socket becomes dislodged or undergoes fibrinolytic dissolution, exposing bare bone. It is not primarily an infection - the pain arises from inflammation of exposed alveolar bone, not from suppuration.
- Roberts and Hedges' Clinical Procedures in Emergency, p. 1576
- Tintinalli's Emergency Medicine, p. 1623
Incidence
- Occurs in 2-5% of all routine tooth extractions
- Rises to 20-30% after removal of impacted mandibular third molars
- Rosen's Emergency Medicine, p. 862; Tintinalli's Emergency Medicine, p. 1623
Pathophysiology
After extraction, a blood clot fills the socket and provides a scaffold for healing. If this clot is lost (mechanically dislodged or broken down by fibrinolysis), the underlying alveolar bone is exposed to oral bacteria and inflammation ensues - a localized osteomyelitis of the exposed bone.
Timing
Symptoms typically begin 2-5 days after extraction, and the condition can persist for 5 to 40 days without treatment.
Risk Factors / Contributing Causes
| Category | Specific Factors |
|---|---|
| Mechanical loss of clot | Smoking, straw use, excessive rinsing/spitting, sucking |
| Surgical factors | Traumatic extraction, inadequate blood supply to site, foreign bodies left in socket |
| Local infection | Preexisting pericoronitis or periodontal disease |
| Medications/hormones | Oral contraceptives, corticosteroids, hormone replacement therapy |
| Prior history | Previous episode of dry socket (familial tendency noted) |
- Roberts and Hedges', p. 1576; Scott-Brown's Otorhinolaryngology, p. 1271
A 2026 systematic review (PMID 41578912) found that COX-2 selective inhibitors (e.g., celecoxib) may also increase the risk of alveolar osteitis - a relatively new finding worth noting.
Clinical Features (Signs & Symptoms)
- Moderate to severe pain localized to the extraction site, often radiating to the ear
- Foul odor or taste in the absence of purulence
- Empty socket - no visible clot, bare bone visible
- Symptoms 3-5 days after extraction
- No swelling, purulence, lymphadenitis, or fever (distinguishes it from osteomyelitis)
Key distinction: Dry socket causes no fever or leukocytosis. Osteomyelitis causes fever, leukocytosis, malaise, and nausea. - Roberts and Hedges', p. 1576
Treatment
1. Pain Block First
Because the pain of dry socket is not relieved by traditional oral analgesics, an inferior alveolar nerve block (IAN block) provides instant relief and allows treatment to proceed comfortably.
2. Socket Irrigation
Gently irrigate the socket with warmed saline or chlorhexidine 0.12% oral rinse to remove debris. Gentle suctioning of accumulated material follows.
3. Socket Packing
Pack the socket with one of the following:
- Gauze (1/4 inch) impregnated with eugenol (oil of cloves) or local anesthetic - packed to the level of the gingival cusps; needs replacement every 24-36 hours
- Gelfoam slurry with eugenol - Gelfoam acts as a matrix to hold eugenol in place
- Commercial dry socket paste (e.g., Dry Socket Paste, Dressol-X) - sticky eugenol-containing paste that stays in place longer; can be used alone or mixed with Gelfoam
Multiple packings may be needed before healing is complete. Dental follow-up is mandatory.
4. Analgesics
NSAIDs are preferred over narcotics for dry socket pain. - Roberts and Hedges', p. 1577
5. Antibiotics
- Not routinely required once the socket is packed
- Reserved for cases with systemic signs of infection
- Local socket treatment (curettage to allow fresh clot to reform) is the definitive approach
- Scott-Brown's Otorhinolaryngology, p. 1271; Tintinalli's, p. 1623
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Dry socket | Afebrile, no leukocytosis, no swelling, empty socket |
| Osteomyelitis | Fever, leukocytosis, malaise, nausea |
| Periapical abscess | Swelling, fluctuance, tooth tenderness to percussion |
| Postextraction bleeding | Active blood in socket, hemostatic problem |
Prevention
- Avoid smoking, straw use, and forceful rinsing/spitting post-extraction
- Atraumatic surgical technique
- Preoperative chlorhexidine rinse or socket irrigation may reduce incidence
- Consider avoiding COX-2 inhibitors perioperatively (emerging evidence, PMID 41578912)
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine | Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine
Ianb
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Inferior Alveolar Nerve Block (IANB)
Overview
The IANB is the primary regional anesthetic technique for the mandible. Because the mandibular cortical bone is thick (unlike the maxilla), infiltrative anesthesia is usually insufficient for mandibular teeth - a nerve block is required. It should be in every emergency provider's skill set for dental trauma, dry socket, periapical abscess, and pericoronitis.
- Roberts and Hedges' Clinical Procedures in Emergency, p. 663
- Tintinalli's Emergency Medicine, p. 1632
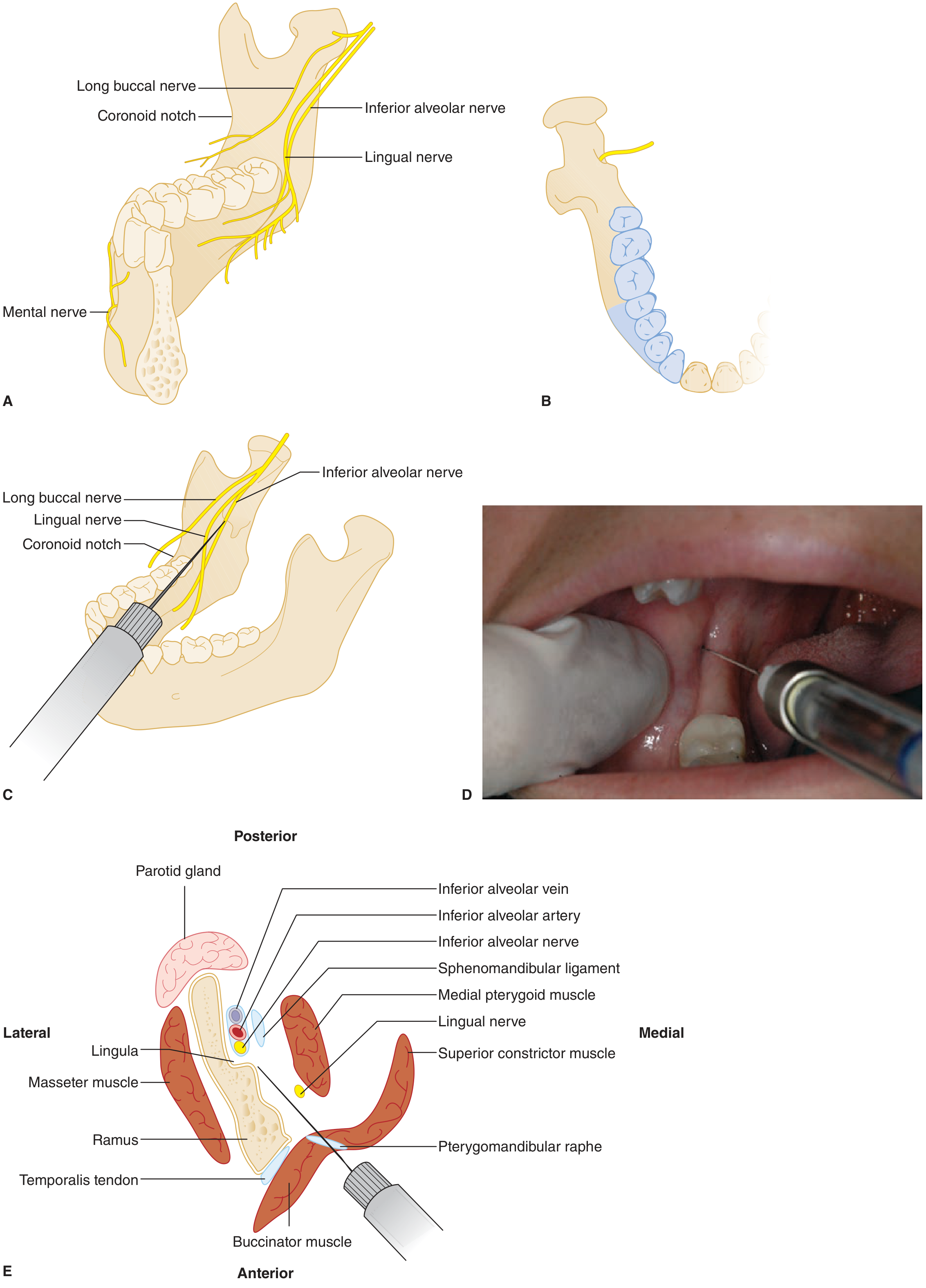
Nerve Anatomy
The inferior alveolar nerve (IAN) is the largest branch of the mandibular nerve (V3 - trigeminal). Its course:
- Descends deep to the external pterygoid muscle
- Passes between the ramus of the mandible and the sphenomandibular ligament
- Enters the mandibular canal (at the mandibular foramen, guarded by the lingula)
- Travels through the mandibular canal innervating all lower teeth on that side
- Bifurcates at the mental foramen:
- Mental nerve - exits to supply the lower lip and chin
- Incisive branch - continues to the anterior teeth
The lingual nerve runs superficial and medial to the IAN and is easily co-blocked with the same injection.
Area of Anesthesia
A successful IANB anesthetizes:
- All teeth on the ipsilateral side of the mandible
- Lower lip and chin (via mental nerve blockade)
- Usually also the floor of the mouth, lingual gingiva, and anterior 2/3 of the tongue (via lingual nerve)
Equipment
- Aspirating dental syringe (monojet) or standard 3-mL aspirating syringe
- 27-gauge, 32-mm needle (long dental needle)
- Local anesthetic cartridge (lidocaine 2% with epinephrine 1:100,000 is standard)
- Topical anesthetic gel (20% benzocaine or 5% lidocaine)
Patient Positioning
Patient seated upright or semi-reclined with head firmly against the headrest. The body of the mandible should be parallel to the floor when the mouth is open. The operator ideally stands on the contralateral side for better visual access.
Classic (Direct) Technique - Step by Step
Step 1 - Apply topical anesthetic
Dry the mucosa with gauze, then apply topical lidocaine gel to the pterygomandibular area for at least 1 minute.
Step 2 - Identify landmarks
- Palpate the coronoid notch (deepest point of the anterior border of the mandibular ramus) with your index finger or thumb placed in the retromolar fossa
- Retract tissue toward the cheek to reveal the pterygomandibular triangle/depression (between the pterygomandibular raphe medially and the coronoid notch laterally)
Step 3 - Needle angulation
- Aim the syringe from the contralateral premolar area (barrel passes between the first and second premolars on the opposite side)
- Failing to achieve this angle is the most common cause of failure
- In children: the mandibular foramen is lower, so the barrel should be held slightly higher
Step 4 - Insertion point
- Insert needle into the pterygomandibular depression at a point 1 to 1.5 cm above the occlusal plane (approximately at the level of the palpating fingertip)
- Advance slowly until bone is contacted at ~20-25 mm depth (posterior wall of the mandibular sulcus, above the lingula)
- If no bone is felt, the needle is likely directed too posteriorly into the parotid gland
Step 5 - Aspirate and inject
- Withdraw needle 1-2 mm from the bone
- Aspirate - if negative for blood, slowly inject 1.5 mL of anesthetic
- Withdraw needle halfway, inject the remainder of the carpule - this ensures lingual nerve block
Step 6 - Onset
- Tingling of the lower lip begins shortly after injection
- Complete anesthesia in 3-5 minutes
Co-blocking Adjacent Nerves
| Nerve | Technique | Area Blocked |
|---|---|---|
| Lingual nerve | Inject remainder of carpule while withdrawing needle halfway | Anterior 2/3 of tongue, floor of mouth, lingual gingiva |
| Long buccal nerve | Inject 0.5 mL distal and buccal to the last mandibular molar | Buccal soft tissue of molars |
Supplementing with long buccal block helps cover aberrant fibers.
Alternative Techniques
| Technique | Key Feature |
|---|---|
| Gow-Gates | Higher injection at the neck of the condyle; broader anesthesia; lower failure rate |
| Akinosi-Vazirani | Closed-mouth technique; used when patient cannot open widely (trismus) |
Failure Rate & Causes
- Classic IANB has a 15-20% failure rate
- Most common cause: incorrect angulation (not directing from contralateral premolars)
- Injection too low (at occlusal level) deposits anesthetic over the bony lingula - anesthetic cannot reach the nerve
- Needle directed too posteriorly enters the parotid gland
Complications
| Complication | Cause | Notes |
|---|---|---|
| Temporary facial nerve palsy | Injection into parotid gland (too posterior) | Benign; resolves spontaneously; protect eye with patch |
| Hematoma | Trauma to inferior alveolar artery/vein or pterygoid plexus | Self-limiting; treat with ice |
| Lingual nerve paresthesia | Inadvertent lingual nerve injury | Usually temporary; rarely permanent |
| Trismus | Local trauma to muscles of mastication | Usually resolves |
| Needle breakage | Bending needle prior to use or redirecting while injecting | Uncommon but serious |
| Vasovagal syncope | Anxiety/pain response | Standard management |
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.