Cirrhosis of liver, cholecystitis, reffered pain of gall bladder
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have all the material needed for a comprehensive answer. Let me now compose the full response.
Cirrhosis of the Liver, Cholecystitis, and Referred Pain of the Gallbladder
1. Cirrhosis of the Liver
Definition
Cirrhosis is the end stage of any chronic liver disease, characterized by replacement of normal liver parenchyma with fibrous tissue and regenerative nodules, leading to distortion of hepatic architecture and vascular flow.
Pathogenesis
The central pathogenic event is activation of hepatic stellate cells (also called Ito cells or perisinusoidal cells). These cells reside in the space of Disse between hepatocytes and sinusoidal endothelial cells. Normally, they are quiescent and store retinoids (vitamin A). After liver injury:
- They become activated, lose their vitamin A stores, proliferate, and develop prominent rough endoplasmic reticulum
- They secrete extracellular matrix (collagen types I and III, sulfated proteoglycans, glycoproteins)
- They transform into contractile myofibroblasts
This collagen deposition leads to defenestration of sinusoidal endothelial cells ("capillarization" of sinusoids), impairing exchange between plasma and hepatocytes and narrowing sinusoidal diameter.
Normal vs. Cirrhotic Liver
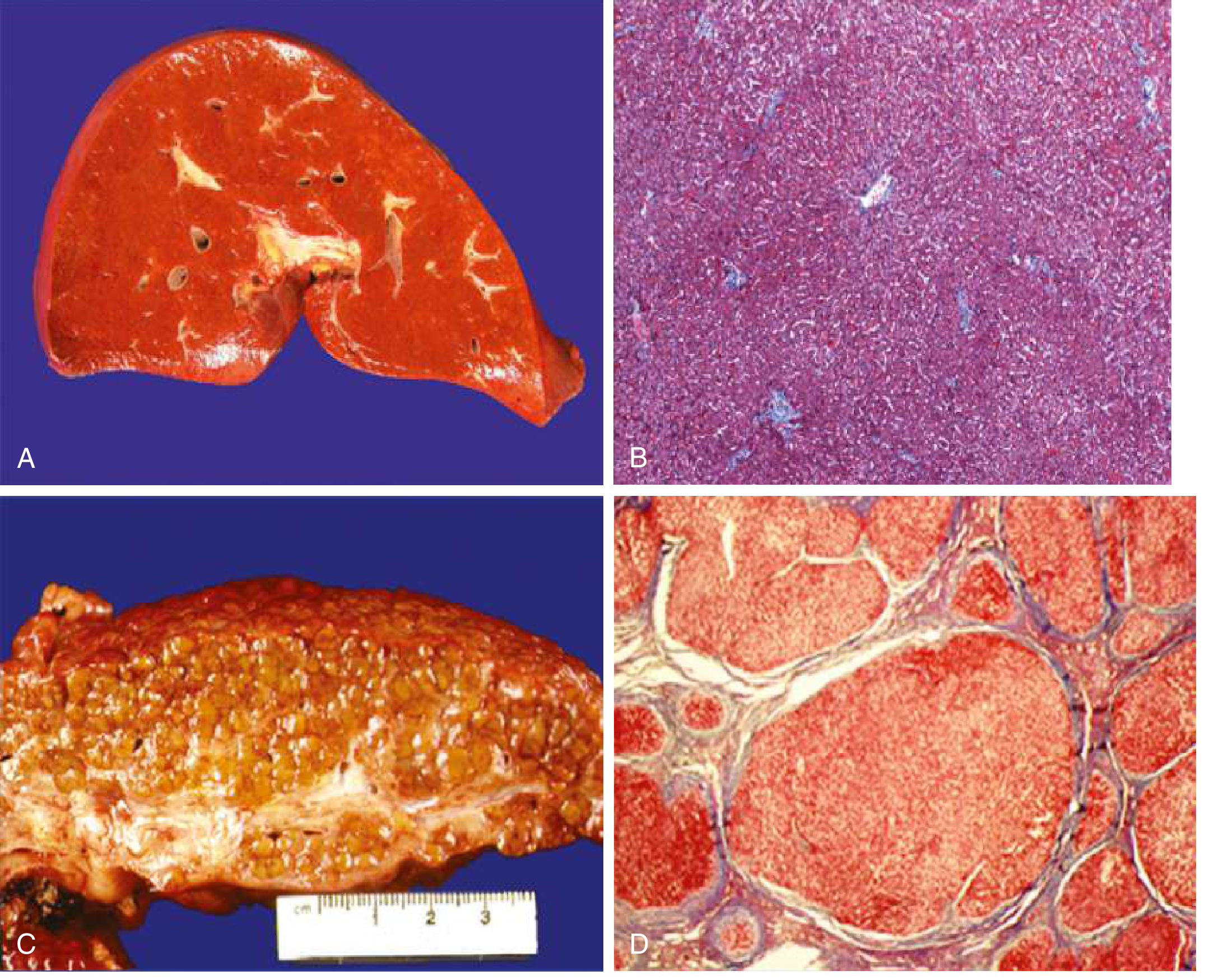
A: Normal liver - smooth surface. B: Normal microscopy - organized sinusoids. C: Cirrhotic liver - irregular, nodular, orange-tawny surface. D: Cirrhotic microscopy - regenerative nodules surrounded by fibrous tissue.
Causes of Cirrhosis
Main causes (>90% of cases):
- Alcoholic liver disease
- Non-alcoholic fatty liver disease (NAFLD/NASH)
- Chronic hepatitis B
Other causes (<2% each):
- Chronic hepatitis C
- Primary biliary cirrhosis, Primary sclerosing cholangitis, Autoimmune hepatitis
- Hemochromatosis, Wilson disease, α1-antitrypsin deficiency
- Budd-Chiari syndrome, Right-sided heart failure
- Drugs/toxins, Cystic fibrosis
Complications of Cirrhosis
The two main consequences are portal hypertension (with hyperdynamic circulation) and liver insufficiency:
| Complication | Mechanism |
|---|---|
| Ascites | Portal hypertension + hypoalbuminemia; most frequent sign of decompensation (80%) |
| Variceal hemorrhage | Portosystemic collaterals (gastroesophageal varices); medium/large varices bleed at ~15%/year |
| Hepatic encephalopathy | Both portal hypertension and liver insufficiency |
| Jaundice | Liver insufficiency - failure to excrete bilirubin |
| Spontaneous bacterial peritonitis (SBP) | Complication of ascites |
| Hepatorenal syndrome | Functional renal failure |
| Hepatocellular carcinoma | Can occur at any stage |
Clinical Stages
Compensated cirrhosis:
- Mostly asymptomatic; diagnosed incidentally
- Nonspecific fatigue, weight loss, decreased libido, sleep disturbances
- ~40% already have esophageal varices (asymptomatic)
- Transition to decompensated at ~5-7% per year; median time ~6 years
Decompensated cirrhosis:
-
Defined by: ascites, variceal hemorrhage, hepatic encephalopathy, jaundice, or any combination
-
Rapidly progressive; can be accelerated by recurrent bleeding, HRS, hepatopulmonary syndrome, or sepsis
-
Goldman-Cecil Medicine, pp. 1614-1617
2. Cholecystitis
Definition & Overview
Inflammation of the gallbladder - almost always associated with gallstones. It is one of the most common indications for abdominal surgery in the US.
Types
A. Acute Calculous Cholecystitis (most common - 90% of cases)
Precipitant: Obstruction of the gallbladder neck or cystic duct by a stone.
Pathogenesis (chemical inflammation first, then possibly bacterial):
- Obstruction of bile outflow causes bile stasis
- Phospholipases hydrolyze biliary lecithin to lysolecithin - toxic to mucosa
- Disruption of protective glycoprotein mucous layer exposes epithelium to bile salt detergent action
- Prostaglandins released from distended gallbladder wall amplify mucosal and mural inflammation
- Increased intraluminal pressure compromises mucosal blood flow - ischemia
- Bacterial infection may be superimposed later
Morphology:
- Gallbladder: enlarged, tense, bright red or violaceous (subserosal hemorrhages)
- Serosa covered by fibrinous or fibrinopurulent exudate
- Lumen filled with turbid bile, fibrin, blood, pus
- If filled with pus: empyema of the gallbladder
- Severe: green-black necrotic wall - gangrenous cholecystitis
Clinical features:
- Steady, severe upper abdominal pain radiating to the right shoulder
- Fever, nausea, leukocytosis
- Right subcostal tenderness and rigidity (abdominal muscle spasm)
- Murphy's sign positive
- Diagnosis: ultrasonography (gallstones + thickened gallbladder wall)
Complications:
- Bacterial superinfection leading to cholangitis or sepsis
- Gallbladder perforation - local abscess or diffuse peritonitis
- Cholecystoenteric fistula (biliary-enteric fistula)
- Gallstone ileus
B. Acute Acalculous Cholecystitis (5-12% of cases)
- No gallstones; results from gallbladder stasis and ischemia
- Occurs in seriously ill patients: major surgery, severe trauma, severe burns, sepsis
- High mortality due to associated conditions
- Diagnosis rests on high clinical suspicion
C. Chronic Cholecystitis
- May follow repeated acute attacks or develop insidiously (most common)
- Almost always associated with gallstones, but gallstones are not essential for inflammation
- Supersaturation of bile predisposes to both chronic inflammation and stone formation
- Microorganisms (E. coli, enterococci) cultured from bile in ~1/3 of cases
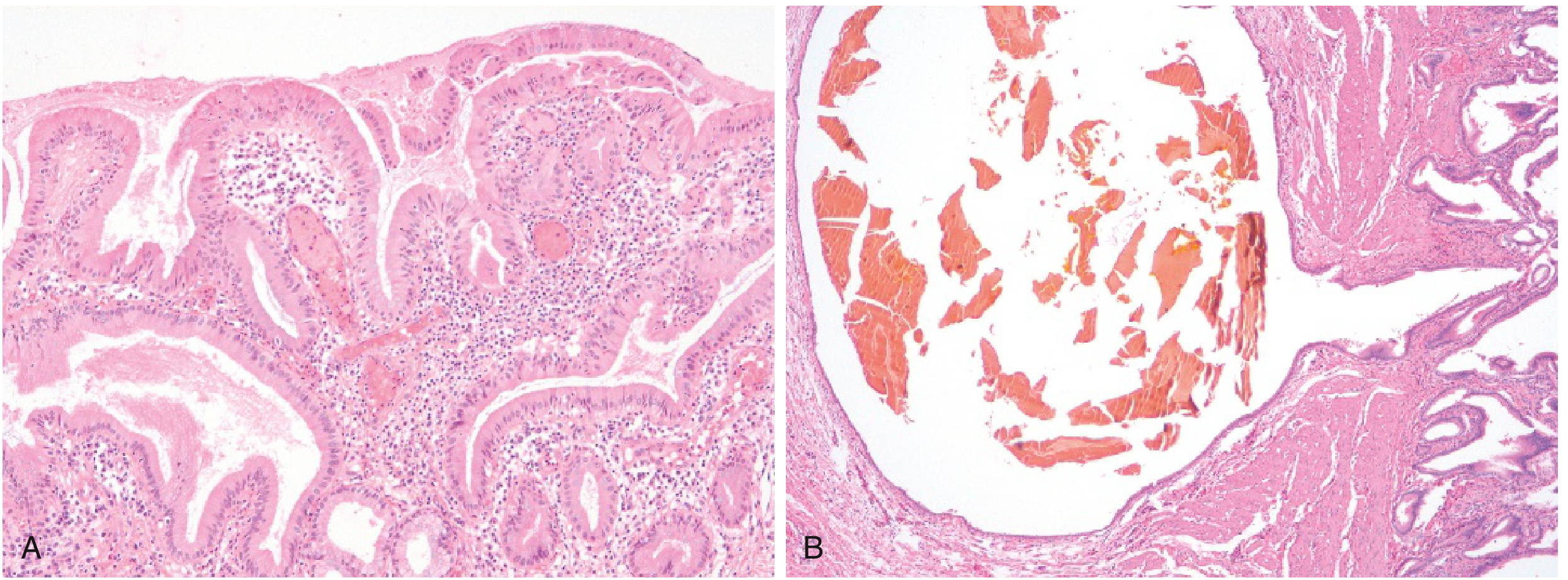
Morphology:
- Marked subepithelial and subserosal fibrosis
- Chronic inflammatory cells (lymphocytes) in the wall
- Prominent Rokitansky-Aschoff sinuses (outpouchings of mucosal epithelium through the wall)
Clinical features: Recurrent attacks of epigastric or right upper quadrant pain; nausea; vomiting - often triggered by fatty meals
- Robbins & Kumar Basic Pathology, pp. 632-633
3. Referred Pain of the Gallbladder
Mechanism of Referred Pain
Referred pain is visceral pain perceived as arising from a somatic location. It follows the dermatomal rule: visceral afferents enter the spinal cord at the same segments as somatic afferents from a distant skin site, causing the brain to mislocalize the pain to the dermatome.
The gallbladder is supplied by sympathetic nerves from the 7th to 9th thoracic segments (T7-T9).
Three Patterns in Acute Cholecystitis (a classic teaching example)
Acute cholecystitis demonstrates all three types of abdominal pain in sequence:
| Stage | Pattern | Location | Description |
|---|---|---|---|
| Early (cystic duct impaction) | Visceral | Epigastrium / midline | Vague, diffuse; foregut origin |
| Progressive (serosal involvement) | Somatoparietal | Right upper quadrant | Intense, well-localized, lateralized |
| Referred | Referred | Right scapula / right shoulder | Via T7-T9 dermatomal rule |
Sites of Referred Pain
- Biliary colic / cholecystitis: Pain radiates from the right hypochondrium to the inferior angle of the right scapula and right shoulder - because the gallbladder shares T7-T9 sympathetic innervation with the skin over the right shoulder/scapular region
- Diaphragmatic irritation: Bile, blood, or inflammatory exudate under the diaphragm (phrenic nerve C3, C4, C5) refers pain to the ipsilateral shoulder tip via the supraclavicular nerves (C3-C4)
Referred Pain Diagram
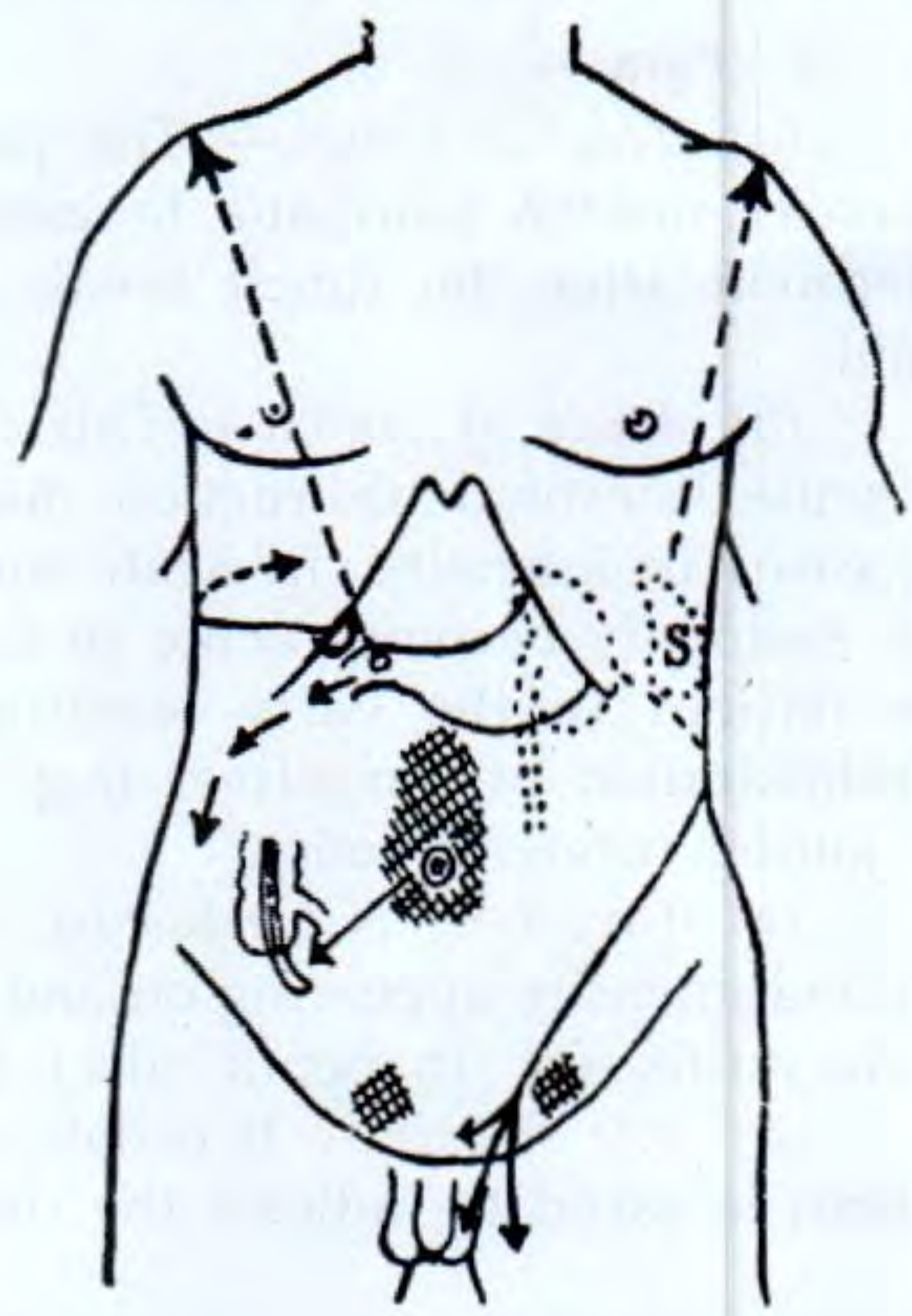
Arrows indicate referred pain pathways - note bilateral shoulder referral for diaphragmatic irritation and right scapular referral for biliary pathology.
Key Nerve Supply Summary
| Structure | Sympathetic Supply | Referred Pain Site |
|---|---|---|
| Gallbladder | T7-T9 | Right scapula / right shoulder |
| Stomach, duodenum, jejunum | T5-T8 | Epigastrium |
| Ileum, appendix | T9-T10 | Periumbilical |
| Colon | T11-T12, L1-L2 | Hypogastrium |
| Diaphragm | Phrenic (C3, C4, C5) | Ipsilateral shoulder tip |
| Kidney/ureter | L1-L2 (genitofemoral nerve) | Loin to groin, testis, inner thigh |
- Costanzo Physiology 7th Ed., p. 90
- Yamada's Textbook of Gastroenterology 7th Ed.
- S Das Manual on Clinical Surgery 13th Ed., p. 456
Quick Summary Table
| Topic | Key Points |
|---|---|
| Cirrhosis | End-stage liver disease; hepatic stellate cell activation; portal HTN + liver failure; compensated vs. decompensated |
| Cholecystitis | Almost always with gallstones; chemical injury first, then bacterial; acute vs. chronic; Rokitansky-Aschoff sinuses in chronic |
| Referred pain (gallbladder) | Via T7-T9; right scapular angle + right shoulder; dermatomal rule; diaphragmatic irritation can also refer to shoulder via C3-C5 |
This is a shared conversation. Sign in to Orris to start your own chat.