Detailed about humoral and cellular immune response
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Humoral and Cellular Immune Response
The adaptive immune response has two major arms: humoral immunity (antibody-mediated, driven by B cells) and cellular immunity (cell-mediated, driven by T cells). Both develop concurrently after antigen encounter and are interdependent. Unlike innate immunity, adaptive immunity is highly antigen-specific, slower to develop, and generates immunological memory.
OVERVIEW: Adaptive vs. Innate Immunity
| Feature | Innate | Adaptive |
|---|---|---|
| Speed | Immediate (minutes-hours) | Slow (days-weeks) |
| Antigen specificity | Non-specific | Highly specific |
| Memory | No | Yes |
| Key cells | Phagocytes, NK cells | T lymphocytes, B lymphocytes, APCs |
| Mediators | Complement, defensins, TLRs | Antibodies, cytokines |
- Jawetz Melnick & Adelberg's Medical Microbiology, 28e, Table 8-1
PART 1: HUMORAL IMMUNE RESPONSE
Definition
Humoral immunity is mediated by secreted antibodies produced by the B lymphocyte lineage. It primarily defends against extracellular pathogens (bacteria, toxins, free viruses).
B Cell Development and Maturation
-
B cells originate and mature in the bone marrow from pluripotent hematopoietic stem cells
-
Pre-B cell growth is stimulated by IL-7 (from bone marrow stromal cells)
-
B cells then mature and proliferate as primed B cells under the influence of IL-4, IL-5, and IL-6
-
Each B cell undergoes VDJ recombination of immunoglobulin genes, producing a unique B cell receptor (BCR) specific for a single antigen
-
Naive B cells co-express IgM and IgD on their surface
-
After maturation, B cells migrate to secondary lymphoid organs (lymph nodes, spleen, MALT) to await antigen encounter
-
Fischer's Mastery of Surgery, 8e, "B-Cell Maturation and Function"
Antibody Structure
The immunoglobulin molecule consists of:
- Two identical heavy chains + two identical light chains
- A variable region (antigen-binding site, made up of variable portions of both heavy and light chains)
- A constant region - the Fc fragment, which:
- Interacts with Fc receptors on phagocytes (opsonization)
- Activates the complement system (for certain isotypes)
- Heavy chain genes are on chromosome 14; light chain genes on chromosome 2
Immunoglobulin Isotypes (Classes)
There are 9 isotypes in humans:
| Isotype | Function |
|---|---|
| IgM | First antibody produced; highly effective at activating complement; forms pentamer |
| IgD | Co-expressed with IgM on naive B cells; BCR signaling |
| IgG (1-4) | Main serum antibody; opsonization, complement activation, ADCC, crosses placenta |
| IgA (1-2) | Mucosal immunity (GI tract, respiratory tract, breast milk) |
| IgE | Allergic responses, anti-parasitic defense; activates mast cells and eosinophils |
- Fischer's Mastery of Surgery, 8e
B Cell Activation: Two Signals Required
Signal 1: Antigen binds the BCR (surface immunoglobulin), which cross-links two adjacent receptors - this physical cross-linking initiates intracellular signaling. The co-receptor complex CD19-CD21-CD81 lowers the threshold for activation.
Signal 2 (Costimulation): T cell help via CD40L (on T cell) binding to CD40 on the B cell, along with cytokines.
- Fischer's Mastery of Surgery, 8e; Cellular and Molecular Immunology
T-Dependent vs. T-Independent Responses
T-Dependent Antigens (most protein antigens):
- Require CD4+ T helper cell collaboration
- Results in: class switching, affinity maturation, long-lived plasma cells, memory B cells
- Produce IgG, IgA, IgE (high-affinity)
T-Independent Antigens (polysaccharides, lipopolysaccharides):
-
Activate B cells directly through BCR cross-linking (multivalent repeating epitopes)
-
Rapid but simpler response
-
Mostly low-affinity IgM; no memory or affinity maturation
-
Cellular and Molecular Immunology, Chapter 12
Key Processes in T-Dependent Humoral Response
1. Germinal Centre Reaction
After B cell activation in lymph nodes, some B cells enter germinal centres where:
- Somatic hypermutation of immunoglobulin variable region genes occurs
- Affinity maturation selects for B cells with highest-affinity BCRs (low-affinity cells undergo apoptosis)
- Class switching (isotype switching): B cells switch from IgM to IgG, IgA, or IgE under cytokine instruction from T follicular helper (Tfh) cells
2. Plasma Cells
- Terminally differentiated, antibody-secreting cells
- A single B cell can give rise to ~5000 plasma cells within one week, each secreting ~2000 antibody molecules per second
- Long-lived plasma cells migrate to bone marrow and continue secreting antibody for years
3. Memory B Cells
-
Long-lived resting cells
-
On re-exposure to the same antigen, they rapidly differentiate into plasma cells
-
Basis of the secondary (anamnestic) immune response
-
Cellular and Molecular Immunology, Chapter 12
Primary vs. Secondary Antibody Response
| Feature | Primary Response | Secondary Response |
|---|---|---|
| Speed | Slow (1-2 weeks) | Rapid (days) |
| Magnitude | Lower | Much higher (10-100x) |
| Predominant Ig | IgM first, then IgG | IgG (and IgA/IgE) |
| Affinity | Lower | Higher (affinity maturation) |
| Duration | Shorter | Longer |
| Basis | Naive B cell activation | Memory B cell activation |
Effector Functions of Antibodies
- Neutralization - antibodies block pathogen binding to host cell receptors
- Opsonization - IgG Fc region binds Fc receptors on macrophages/neutrophils, enhancing phagocytosis
- Complement activation - IgM and IgG activate the classical complement pathway → lysis (MAC), opsonization (C3b), inflammation (C3a/C5a)
- Antibody-Dependent Cellular Cytotoxicity (ADCC) - IgG-coated targets are destroyed by NK cells via Fc receptor binding
- Mucosal protection - secretory IgA prevents pathogen adherence to mucosal surfaces
- Mast cell / basophil activation - IgE crosslinking on mast cells triggers degranulation (allergic response and anti-parasite defense)
PART 2: CELLULAR (CELL-MEDIATED) IMMUNE RESPONSE
Definition
Cell-mediated immunity is driven by T lymphocytes and is the principal defense against intracellular pathogens (viruses, mycobacteria, fungi), transplanted cells, and tumors.
T Cell Development
- T cells originate in the bone marrow but travel to the thymus to mature
- In the thymus:
- VDJ recombination of TCR β chain, then α chain DNA
- Positive selection: T cells that can recognize self-MHC survive
- Negative selection: T cells that react too strongly to self-antigens (autoreactive) are deleted (central tolerance)
- Result: mature naive T cells expressing either CD4 or CD8 emerge into the periphery
Antigen Presentation: MHC Restriction
- MHC Class I (on ALL nucleated cells): presents endogenous (intracellular) peptides (viral proteins, tumor antigens) to CD8+ T cells
- MHC Class II (on APCs: dendritic cells, macrophages, B cells): presents exogenous (extracellular) peptides to CD4+ T cells
This is the core of MHC restriction: CD4 binds to MHC class II; CD8 binds to MHC class I.
T Cell Activation: Two-Signal Requirement
Signal 1: TCR binds to MHC-peptide complex on APC (antigen-specific recognition)
- CD4 or CD8 acts as a co-receptor, stabilizing the interaction
Signal 2 (Costimulation): CD28 on the T cell binds B7-1 (CD80) or B7-2 (CD86) on the APC
- Without signal 2, T cells become anergic (tolerant), not activated
Together, these signals trigger:
- DNA synthesis and T cell proliferation
- IL-2 secretion and upregulation of IL-2 receptors (autocrine growth loop)
- IFN-γ secretion
- Differentiation into effector T cells
Negative regulation: CTLA-4 and PD-1 are checkpoint receptors that dampen T cell responses to prevent excessive activation.
- Jawetz Melnick & Adelberg's Medical Microbiology, 28e
CD4+ T Helper Cell Subsets
Once activated, naive CD4+ T cells differentiate into specialized effector subsets depending on the cytokine microenvironment and the nature of the antigen:
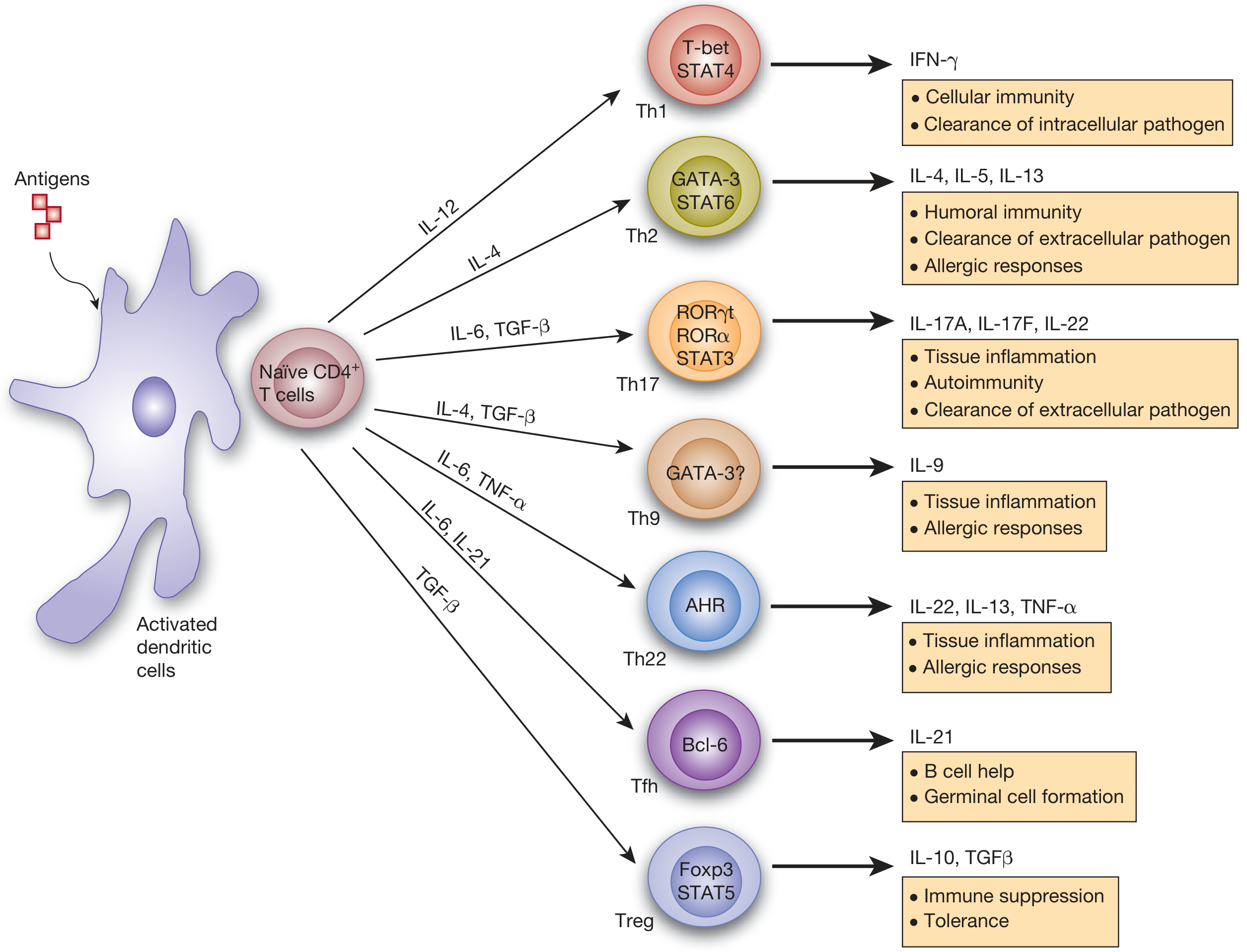
Figure: CD4+ T cell differentiation into Th1, Th2, Th17, Tfh, Treg, Th9, Th22 subsets (Fishman's Pulmonary Diseases)
| Subset | Inducing Cytokines | Master TF | Effector Cytokines | Function |
|---|---|---|---|---|
| Th1 | IL-12, IL-2 | T-bet, STAT4 | IFN-γ, IL-2 | Activates macrophages; cell-mediated immunity against intracellular pathogens (viruses, mycobacteria); promotes IgG class switching |
| Th2 | IL-4 | GATA-3, STAT6 | IL-4, IL-5, IL-13 | Activates B cells for IgE production; eosinophil activation; anti-parasitic; allergic responses |
| Th17 | IL-6 + TGF-β | RORγt, STAT3 | IL-17A, IL-17F, IL-22 | Defense against extracellular bacteria and fungi at mucosal surfaces; involved in autoimmunity |
| Tfh | IL-6, IL-21 | Bcl-6 | IL-21 | Localizes in lymph nodes; provides help to B cells; drives germinal centre formation and antibody class switching |
| Treg | TGF-β | Foxp3, STAT5 | IL-10, TGF-β | Immune suppression, peripheral tolerance, prevention of autoimmunity |
| Th9 | IL-4 + TGF-β | GATA-3? | IL-9 | Tissue inflammation, allergic responses |
| Th22 | IL-6, TNF-α | AHR | IL-22, IL-13, TNF-α | Tissue inflammation, allergic responses |
- Fishman's Pulmonary Diseases, Jawetz Medical Microbiology
CD8+ Cytotoxic T Lymphocytes (CTLs)
Activation:
- CTL precursors (CD8+ T cells) recognize antigen + MHC class I on infected/abnormal cells
- Most CD8 activation is independent of costimulation (unlike CD4+ cells)
- CD4+ T helper cells "license" dendritic cells to activate CD8+ T cells (via CD40-CD40L), or provide cytokines (IL-2, IL-6) nearby
- Once activated, CTLs produce IL-2 and IFN-γ
Mechanisms of target cell killing:
-
Perforin-granzyme pathway:
- CTL releases perforin (forms pores in target cell membrane)
- Granzymes (serine proteases) enter through pores and activate caspases → apoptosis
-
Fas-FasL pathway:
- CTL expresses FasL (CD95L), which binds Fas (CD95) on target cell → caspase-mediated apoptosis
-
Cytokine secretion: IFN-γ activates macrophages and upregulates MHC expression
Targets:
-
Virally infected cells (present viral peptides via MHC I)
-
Tumor cells
-
Intracellular bacteria
-
Transplanted cells (allograft rejection)
-
Roitt's Essential Immunology; Jawetz Medical Microbiology
Macrophage Activation in Cell-Mediated Immunity
- Th1 cells secrete IFN-γ, the most potent macrophage-activating cytokine
- Activated macrophages become "classically activated" (M1 phenotype):
- Enhanced phagocytosis and intracellular killing
- Increased reactive oxygen/nitrogen species production
- Enhanced antigen presentation (upregulate MHC II)
- Secretion of pro-inflammatory cytokines (TNF-α, IL-1, IL-6)
- This is the primary mechanism for killing intracellular pathogens such as Mycobacterium tuberculosis and Leishmania
PART 3: IMMUNOLOGICAL MEMORY
Both humoral and cellular arms generate memory cells after a primary response:
| Memory Type | Cells | Features |
|---|---|---|
| Humoral | Memory B cells, long-lived plasma cells | Rapid IgG response on re-exposure; high affinity; maintained by bone marrow plasma cells secreting antibody for years |
| Cellular | Memory CD4+ and CD8+ T cells | Lower activation threshold; faster clonal expansion; more potent effector functions |
Secondary response characteristics:
-
Faster (days vs. weeks)
-
Larger magnitude
-
Higher affinity antibodies (IgG, IgA, IgE predominate)
-
This underpins vaccine-induced protection
-
Cellular and Molecular Immunology, Chapter 12
PART 4: INTERACTION BETWEEN HUMORAL AND CELLULAR IMMUNITY
The two arms are not separate - they constantly cooperate:
-
Th2 cells drive B cell activation, class switching, and high-affinity IgE/IgG production (humoral)
-
Tfh cells in germinal centres are essential for affinity maturation and long-lived plasma cell generation
-
B cells act as APCs - they capture native antigen via BCR, process it, and present peptides to CD4+ T cells via MHC II (the "hapten-carrier" effect)
-
CD4+ Th1 cells help activate CD8+ CTLs by licensing dendritic cells
-
ADCC bridges both arms: IgG antibodies coat targets which are then killed by NK cells (innate) and CTLs
-
Successful T cell immunosuppression (e.g., in transplantation) also prevents alloantibody formation by B cells, because T cell-mediated alloimmunity drives B cell alloantibody production
-
Fischer's Mastery of Surgery, 8e; Jawetz Medical Microbiology, 28e
SUMMARY TABLE: Humoral vs. Cellular Immunity
| Feature | Humoral Immunity | Cellular Immunity |
|---|---|---|
| Mediated by | B cells / Antibodies | T cells (CD4+, CD8+) |
| Primary defense against | Extracellular bacteria, toxins, free viruses | Intracellular pathogens, viruses, tumors, fungi |
| Key cells | B cells, Plasma cells, Memory B cells | CD4+ Th, CD8+ CTLs, Memory T cells |
| APCs present via | MHC Class II (to CD4+) | MHC Class I (to CD8+) |
| Effector molecules | IgM, IgG, IgA, IgE | IFN-γ, Perforin, Granzymes, FasL |
| Killing mechanism | Neutralization, Opsonization, Complement, ADCC | CTL cytotoxicity, Macrophage activation |
| Memory | Memory B cells + long-lived plasma cells | Memory CD4+ and CD8+ T cells |
| Clinical relevance | Vaccine antibody titers, Autoimmune Ab, Allergy | TB, viral infections, transplant rejection, cancer immunosurveillance |
Sources:
- Cellular and Molecular Immunology, Chapter 12 - B Cell Activation and Antibody Production
- Jawetz Melnick & Adelberg's Medical Microbiology, 28e - Adaptive Immunity
- Fishman's Pulmonary Diseases and Disorders - T Helper Cell Differentiation
- Fischer's Mastery of Surgery, 8e - B-Cell Maturation and Function
- Roitt's Essential Immunology - CTL effectors
- Harrison's Principles of Internal Medicine, 22e - Humoral and Cellular Immune Responses
Facilitated diffusion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Excellent - I now have comprehensive textbook content and clear diagrams. Let me compile the full detailed answer.
Facilitated Diffusion
Definition
Facilitated diffusion is a form of passive transport in which molecules move across the cell membrane down their electrochemical (concentration) gradient - from a region of high concentration to low concentration - with the assistance of specific membrane proteins (carriers or channels). It requires no energy (no ATP).
Classification of Membrane Transport
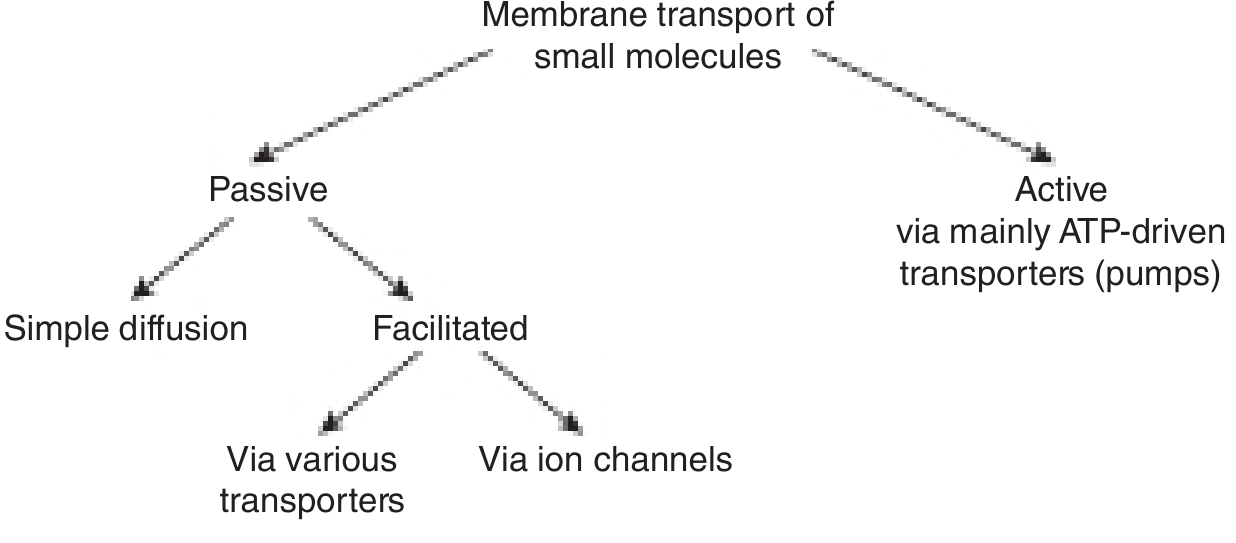
Figure: Membrane transport of small molecules - passive (simple diffusion and facilitated) vs. active (ATP-driven). - Harper's Illustrated Biochemistry, 32e
Why Is It Needed?
The cell membrane is a hydrophobic lipid bilayer. It is freely permeable to:
- Small, nonpolar molecules (O₂, CO₂, ethanol, steroids)
- Small uncharged polar molecules (water, urea)
But it is impermeable to:
- Large molecules (glucose, amino acids)
- Charged ions (Na⁺, K⁺, Ca²⁺, Cl⁻)
- Hydrophilic substances
These molecules cannot cross the bilayer by simple diffusion - they require a protein "facilitator," hence facilitated diffusion.
Mechanism
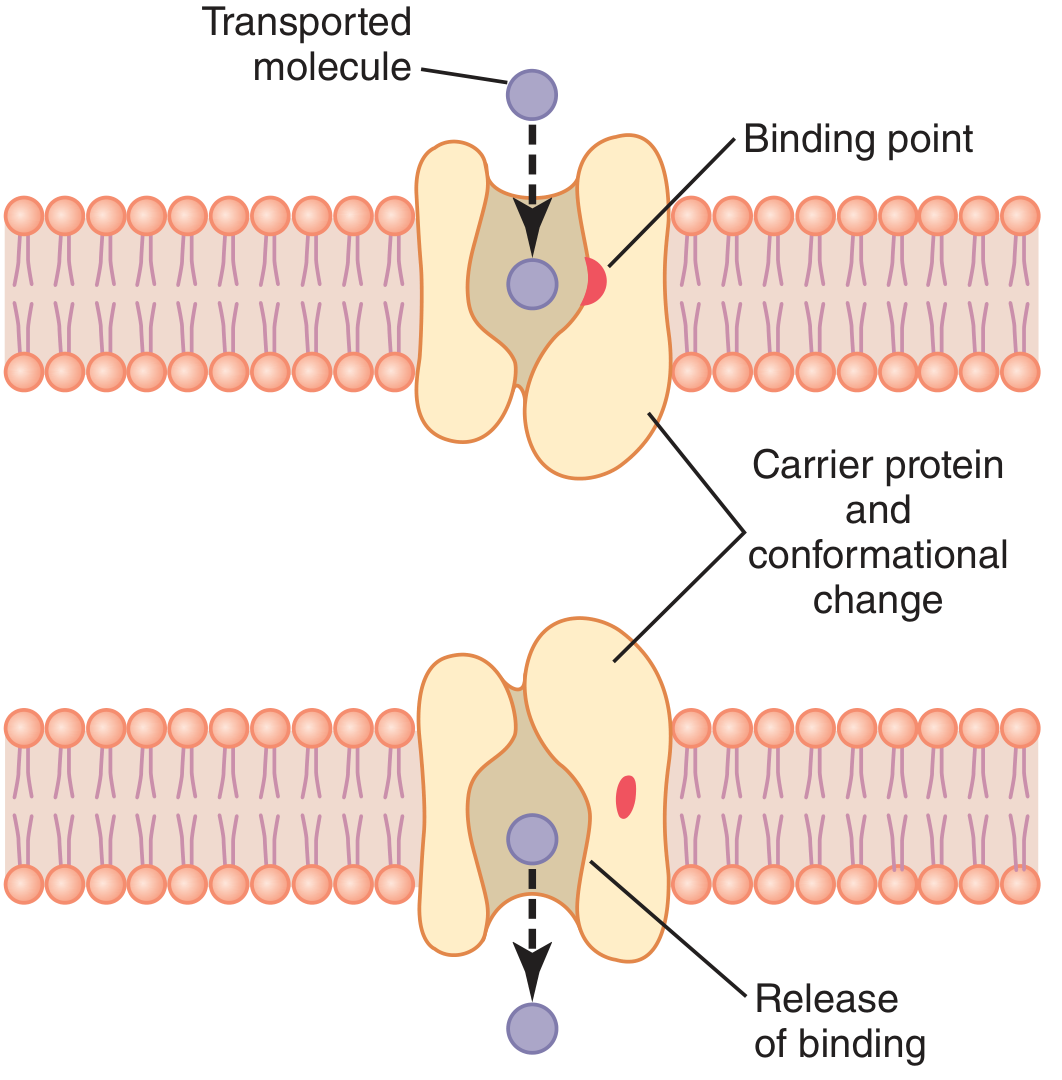
Figure: Postulated mechanism of facilitated diffusion via carrier protein - Guyton & Hall, Medical Physiology
The mechanism works as follows:
- The carrier protein has a pore large enough to partially accommodate the specific molecule
- An intrapore binding receptor (binding site) captures the molecule
- A conformational change occurs in the carrier protein - the pore flips from facing one side of the membrane to the other
- Because the binding force is weak, thermal motion causes the molecule to break free and be released on the opposite side
- The carrier returns to its original conformation and is ready to transport again
- Net movement is always down the concentration gradient - the carrier can transport in either direction, but net flux follows the gradient
- Guyton and Hall Textbook of Medical Physiology
Two Types of Proteins Mediating Facilitated Diffusion
1. Carrier Proteins (Transporters / Permeases)
| Property | Detail |
|---|---|
| Mechanism | Bind solute, undergo conformational change to transfer it across |
| Speed | Slower (100-1000 molecules/sec) |
| Examples | GLUT transporters (glucose), amino acid carriers |
| Transport type | Passive (facilitated diffusion) AND active transport |
2. Ion Channel Proteins
| Property | Detail |
|---|---|
| Mechanism | Form aqueous pores/channels through the membrane |
| Speed | Much faster (10⁶-10⁸ ions/sec) |
| Examples | Na⁺, K⁺, Ca²⁺, Cl⁻ channels; ligand-gated channels |
| Transport type | Passive transport only |
| Selectivity | Selective for specific ions based on size and charge |
- Harper's Illustrated Biochemistry, 32e, Table 40-4
Transport System Classifications (by directionality)
| System | Description | Example |
|---|---|---|
| Uniport | Moves one type of molecule bidirectionally (facilitated diffusion) | GLUT transporters (glucose) |
| Symport | Two solutes move in the same direction (active cotransport) | Na⁺-glucose cotransporter (SGLT) |
| Antiport | Two solutes move in opposite directions (active cotransport) | Na⁺-Ca²⁺ exchanger (3Na⁺ in, 1Ca²⁺ out) |
Note: Symport and antiport use the energy from an existing electrochemical gradient and are forms of secondary active transport, not facilitated diffusion.
Key Characteristics of Facilitated Diffusion
1. Saturation Kinetics (Vmax)
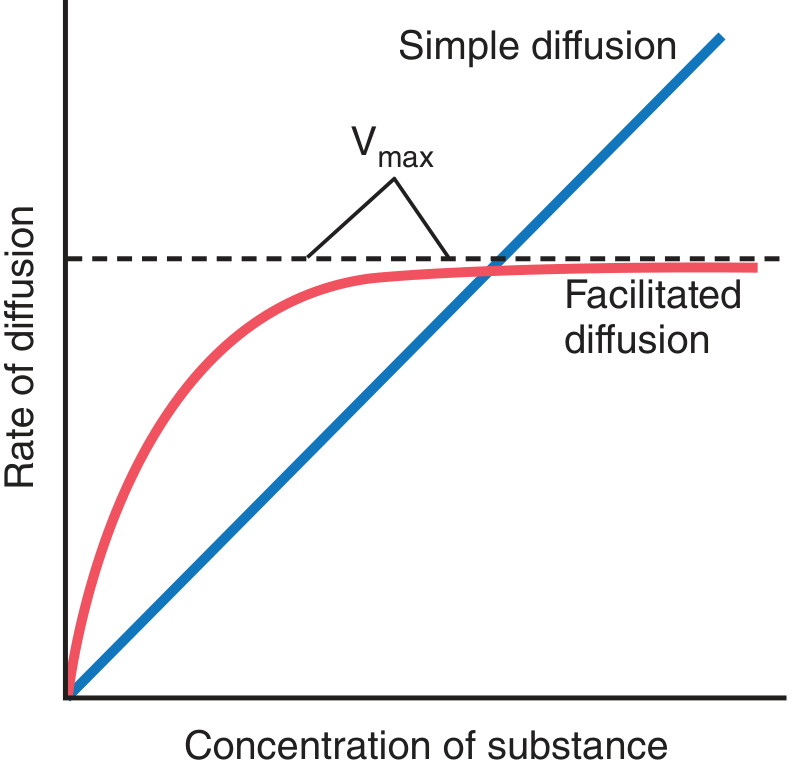
Figure: Rate of diffusion vs. concentration. Simple diffusion rises linearly; facilitated diffusion plateaus at Vmax. - Guyton & Hall Medical Physiology
- In simple diffusion: rate increases linearly and indefinitely with concentration
- In facilitated diffusion: rate increases initially but then plateaus at a maximum rate (Vmax) as all carrier proteins become occupied (saturated)
- This is exactly like enzyme kinetics (Michaelis-Menten), with a Km for the solute
2. Specificity (Stereospecificity)
- Each carrier protein is highly specific for its substrate
- Example: GLUT transporters carry D-glucose but NOT L-glucose (the mirror-image stereoisomer)
- Other monosaccharides (D-galactose, fructose) may use related but distinct carriers
3. Competition
- Structurally similar molecules compete for the same carrier binding sites
- Example: D-galactose and phlorizin competitively inhibit GLUT-mediated glucose transport
- D-galactose is itself transported; phlorizin merely occupies the site
4. Bidirectionality
- The carrier can move molecules in EITHER direction
- Net movement is always down the concentration gradient - the side with higher concentration "wins"
5. No Energy Required
-
Proceeds spontaneously as long as a concentration gradient exists
-
Stops at equilibrium (when concentrations on both sides are equal)
-
Costanzo Physiology, 7e; Guyton & Hall Medical Physiology
Resemblance to Enzyme Kinetics
Both facilitated diffusion and enzyme reactions share:
| Feature | Enzyme | Facilitated Diffusion |
|---|---|---|
| Specific binding site | Active site | Carrier binding site |
| Saturable | Vmax | Vmax |
| Binding affinity | Km | Km (for solute) |
| Competitive inhibition | Yes | Yes |
| Substrate modification | Yes (product formed) | No (substrate unchanged) |
- Harper's Illustrated Biochemistry, 32e
Important Examples
GLUT Transporters (Glucose Transporters)
There are at least 14 GLUT family members in humans, each with tissue-specific expression:
| Transporter | Location | Notes |
|---|---|---|
| GLUT1 | Erythrocytes, brain (blood-brain barrier), endothelium | Basal glucose uptake |
| GLUT2 | Liver, pancreatic β-cells, kidney, intestine (basolateral) | Low-affinity, high-capacity; glucose sensor in β-cells |
| GLUT3 | Neurons | High affinity; ensures brain glucose supply |
| GLUT4 | Skeletal muscle, adipose tissue, heart | Insulin-regulated - key transporter |
| GLUT5 | Small intestine, testes | Primarily fructose |
GLUT4 and Insulin:
-
Normally, GLUT4 resides in intracellular vesicles in the cytosol
-
Insulin triggers translocation of GLUT4 to the plasma membrane
-
This increases membrane density of the transporter and Vmax of glucose uptake by 10-20-fold in insulin-sensitive tissues (skeletal muscle, adipose, heart)
-
This is the mechanism by which insulin lowers blood glucose after a meal
-
Guyton & Hall Medical Physiology
Amino Acid Transporters
- Multiple specific carriers for neutral, acidic, and basic amino acids
- In the intestine and kidney, some amino acid transport uses Na⁺-dependent secondary active transport (not facilitated diffusion), but basolateral exit often uses facilitated diffusion
Ion Channels
- Na⁺/K⁺ channels in neurons underlie the action potential
- Ca²⁺ channels in cardiac and skeletal muscle
- CFTR (Cl⁻ channel) - defective in cystic fibrosis
Facilitated Diffusion vs. Simple Diffusion vs. Active Transport
| Feature | Simple Diffusion | Facilitated Diffusion | Active Transport |
|---|---|---|---|
| Energy (ATP) | No | No | Yes |
| Direction | Down gradient | Down gradient | Against gradient |
| Protein carrier | No | Yes (carrier or channel) | Yes (pump) |
| Saturation | No | Yes (Vmax) | Yes (Vmax) |
| Specificity | No | Yes | Yes |
| Competition | No | Yes | Yes |
| Examples | O₂, CO₂, lipids | Glucose (GLUT), ions (channels) | Na⁺/K⁺ ATPase, Ca²⁺ ATPase |
| Rate vs. concentration | Linear | Hyperbolic (plateaus) | Hyperbolic (plateaus) |
Clinical Relevance
-
Diabetes mellitus - impaired GLUT4 translocation due to insulin resistance; cells fail to take up glucose despite high blood glucose
-
Hypoglycemia in fasting - brain depends almost entirely on GLUT3 (high-affinity) for basal glucose; it is not insulin-dependent
-
SGLT2 inhibitors (gliflozins) - block Na⁺-glucose cotransporters in renal tubules; used to treat T2DM by promoting glucose excretion in urine (note: SGLT is active transport, not facilitated diffusion - but basolateral glucose exit from tubular cells back into blood uses GLUT2, a facilitated transporter)
-
Cystic fibrosis - loss of CFTR (a Cl⁻ channel) impairs facilitated Cl⁻ diffusion across epithelial cells → thick mucus in lungs, pancreatic ducts
-
Pharmacokinetics - many drugs enter cells via facilitated diffusion through organic anion/cation transporters (OAT, OCT); saturation of these transporters affects drug bioavailability and drug-drug interactions - Goodman & Gilman's Pharmacological Basis of Therapeutics
Sources:
- Guyton and Hall Textbook of Medical Physiology - Facilitated Diffusion Using Membrane Carrier Proteins
- Costanzo Physiology, 7e - Facilitated Diffusion
- Harper's Illustrated Biochemistry, 32e - Transporters and Facilitated Diffusion
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Basic Mechanisms of Membrane Transport
This is a shared conversation. Sign in to Orris to start your own chat.