Does m2 and m4 increase receptor increase calcium levels or decrease
Reading File
Finding Sources
Finding Sources
The textbooks confirm the answer clearly. Here is the full breakdown:
M2 and M4 Muscarinic Receptors: Effect on Calcium
M2 and M4 receptors DECREASE (inhibit) calcium signaling - they do NOT increase it.
Here is how the different muscarinic subtypes compare:
Excitatory Receptors (M1, M3, M5) - INCREASE calcium
- Coupled to Gq protein
- Activate phospholipase C → generate IP3 and DAG
- IP3 triggers release of calcium from the endoplasmic reticulum → increases intracellular calcium
Inhibitory Receptors (M2, M4) - DECREASE/inhibit
- Coupled to Gi protein (inhibitory G protein, pertussis toxin-sensitive)
- Inhibit adenylyl cyclase → decrease cAMP
- Do not generate IP3, so they do not mobilize intracellular calcium
- They actually attenuate calcium-dependent signaling pathways
Summary Table
| Receptor | G Protein | Effect on cAMP | Effect on Calcium |
|---|---|---|---|
| M1, M3, M5 | Gq | No direct effect | ↑ Increase (via IP3) |
| M2, M4 | Gi | ↓ Decrease (inhibit adenylyl cyclase) | ↓ Decrease / No increase |
Clinical relevance
- In the heart, M2 receptors (predominant subtype) slow the rate via Gi → reduced cAMP → reduced Ca²⁺ influx through L-type channels → negative chronotropy/dromotropy
- In the bladder detrusor, M3 (not M2/M4) mediates the main contractile response because it is the calcium-mobilizing subtype
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. | Campbell-Walsh Urology
Give very very mbbs detalied comparision btw sympathetic ns and parasympathetic ns
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Sympathetic vs Parasympathetic Nervous System - Complete MBBS Comparison
1. OVERVIEW / NICKNAME
| Feature | Sympathetic (SNS) | Parasympathetic (PSNS) |
|---|---|---|
| Nickname | "Fight or Flight" / "Thoracolumbar" | "Rest and Digest" / "Craniosacral" |
| Walter Cannon's term | "Preparation for flight or fight" | "Vegetative nervous system" |
| General function | Emergency, catabolic, energy expenditure | Conservation, anabolic, housekeeping |
| Discharge pattern | Mass discharge (whole system at once) | Discrete, organ-specific responses |
2. ANATOMICAL ORIGIN (Outflow)
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
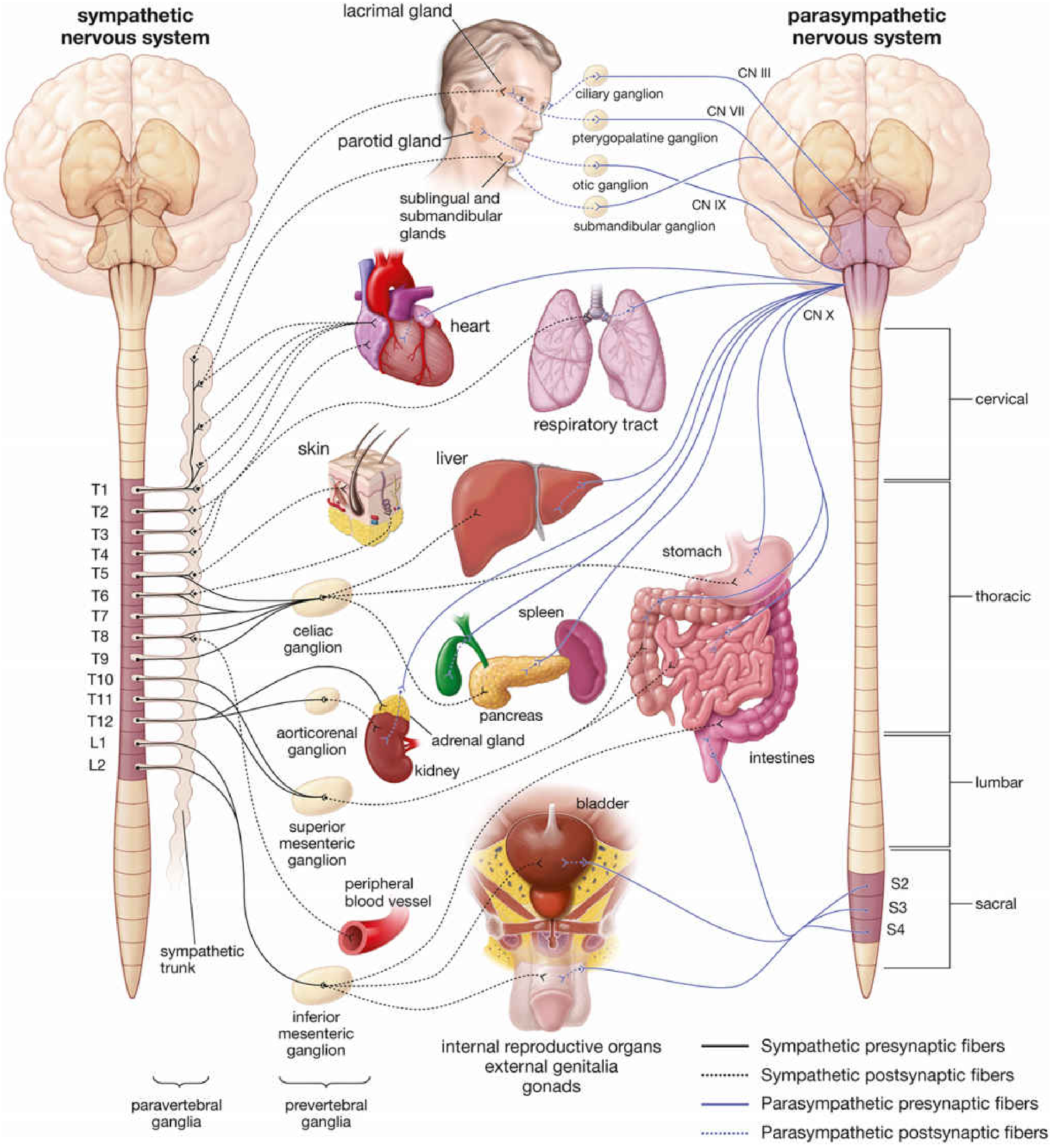
| Origin in CNS | Thoracic T1-L2 (or T1-L3) spinal cord | Brainstem (CN III, VII, IX, X) + Sacral S2-S4 |
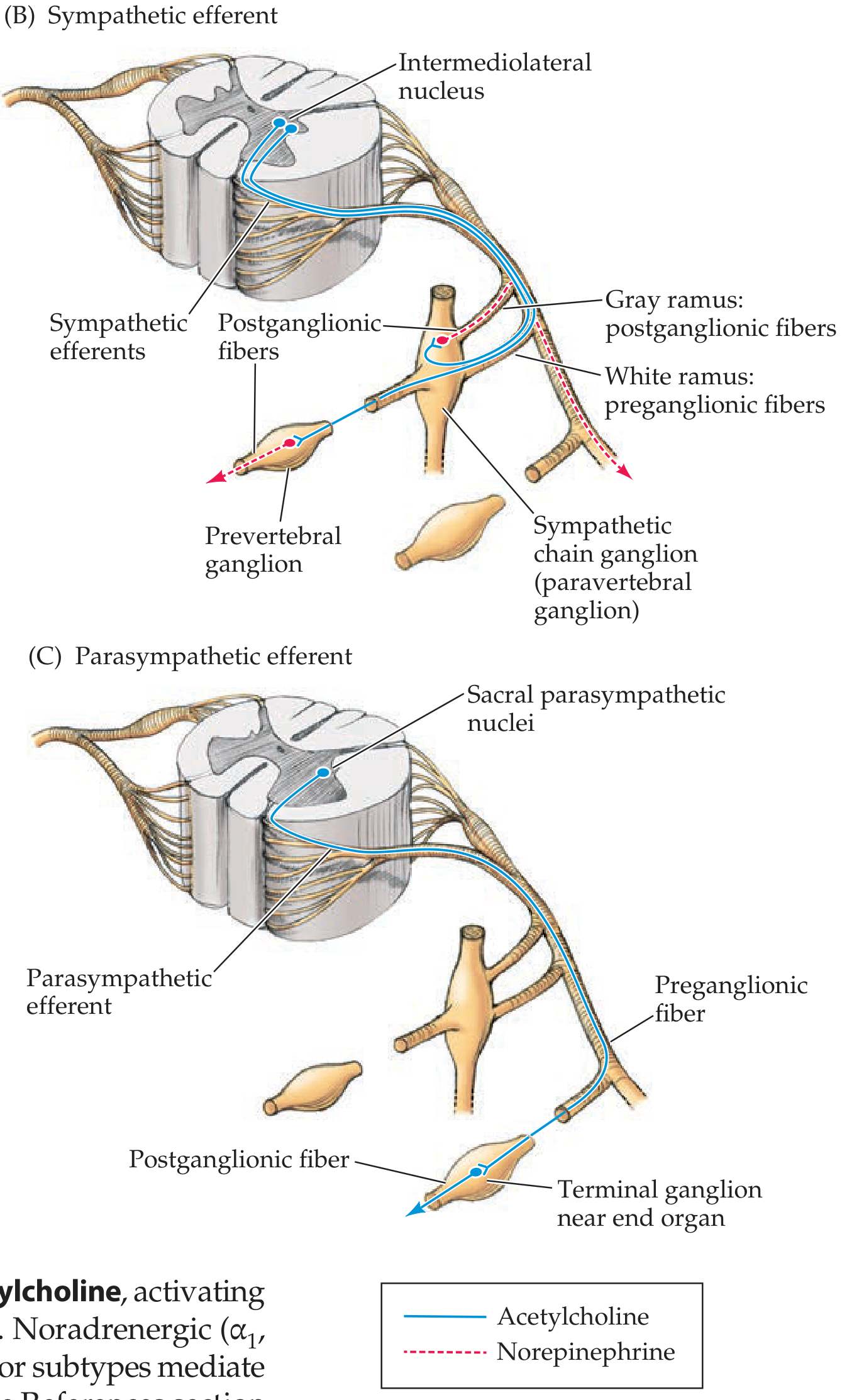
| Cell body location (preganglionic) | Intermediolateral cell column (lateral horn) of spinal cord | Cranial nerve nuclei in brainstem + sacral parasympathetic nuclei |
| Alternate name | Thoracolumbar division | Craniosacral division |
Mnemonic - PSNS cranial nerves: "Some Say Marry Money But My Brother Says Big Brains Matter More" (or simply: CN III, VII, IX, X)
3. GANGLIA - LOCATION AND DISTANCE
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Ganglia location | Near the spinal cord (paravertebral or prevertebral) - far from target organ | Near/in the wall of target organ (terminal ganglia) - close to effector |
| Paravertebral ganglia | Sympathetic chain/trunk on either side of vertebral column | None |
| Prevertebral ganglia | Celiac, superior mesenteric, inferior mesenteric, aorticorenal ganglia | None |
| Terminal (intramural) ganglia | None | Present (in or near organ wall) |
| Named ganglia (head/neck for PSNS) | Superior, middle (often absent), inferior (stellate) cervical ganglia | Ciliary, pterygopalatine, otic, submandibular ganglia |
Sympathetic chain allows: Upper thoracic cord (T1-T3) to reach head and neck via cervical chain ganglia.
4. PRE- AND POSTGANGLIONIC FIBERS
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Preganglionic fiber | Short (ganglion near cord) | Long (ganglion near organ) |
| Postganglionic fiber | Long (travels far to organ) | Short (just the last bit to organ) |
| Preganglionic fiber type | Lightly myelinated (B fibers) | Lightly myelinated (B fibers) |
| Postganglionic fiber type | Unmyelinated (C fibers) | Unmyelinated (C fibers) |
| Preganglionic branching | High (1 pre → many post neurons) = diffuse response | Low (1 pre → few post neurons) = discrete response |
| Ratio (pre:post) | 1:20 or more | 1:1 to 1:3 |
Clinical implication: SNS produces widespread simultaneous responses; PSNS produces targeted responses.
5. NEUROTRANSMITTERS
| Site | Sympathetic | Parasympathetic |
|---|---|---|
| Preganglionic → Ganglion | Acetylcholine (ACh) - acts on Nicotinic receptors (Nn) | Acetylcholine (ACh) - acts on Nicotinic receptors (Nn) |
| Postganglionic → Target organ | Norepinephrine (NE) - acts on Adrenergic receptors | Acetylcholine (ACh) - acts on Muscarinic receptors |
| Exception 1 - Sweat glands | Acetylcholine (cholinergic sympathetic!) on M3 receptors | - |
| Exception 2 - Adrenal medulla | Pre-ganglionic ACh → Chromaffin cells release Epinephrine (80%) + NE (20%) directly into blood | - |
| Exception 3 - Blood vessels (some) | Vasodilator fibers use ACh | - |
Key fact: The adrenal medulla = modified sympathetic ganglion. Chromaffin cells = modified postganglionic neurons that secrete into blood instead of a synapse.
6. RECEPTORS
Adrenergic Receptors (Sympathetic targets)
| Receptor | Location | Effect when activated |
|---|---|---|
| α1 | Vascular smooth muscle, iris (dilator), bladder sphincter, prostate | Vasoconstriction, mydriasis, sphincter contraction |
| α2 | Presynaptic (autoreceptors), platelets, fat cells | Inhibit NE release, platelet aggregation, fat inhibition |
| β1 | Heart (SA node, AV node, ventricles) | ↑HR (chronotropy), ↑conduction (dromotropy), ↑contractility (inotropy) |
| β2 | Bronchial smooth muscle, vascular smooth muscle (skeletal muscle), uterus, bladder detrusor | Bronchodilation, vasodilation, uterine relaxation |
| β3 | Adipose tissue, bladder detrusor | Lipolysis, detrusor relaxation |
Cholinergic Receptors (Parasympathetic targets + autonomic ganglia)
| Receptor | Location | Effect |
|---|---|---|
| Nicotinic (Nm) | NMJ (skeletal muscle) | Muscle contraction |
| Nicotinic (Nn) | All autonomic ganglia, adrenal medulla | Ganglionic transmission |
| Muscarinic M1 | CNS, gastric parietal cells | ↑Gastric acid, CNS excitation |
| Muscarinic M2 | Heart (SA, AV node) | ↓HR, ↓conduction (Gi - inhibit cAMP) |
| Muscarinic M3 | Smooth muscle, glands, endothelium | Contraction of smooth muscle, gland secretion, vasodilation (via NO) |
| Muscarinic M4 | CNS, lung | Inhibitory (Gi) |
| Muscarinic M5 | CNS | Excitatory (Gq) |
7. ORGAN-BY-ORGAN EFFECTS
Diagrammatic Overview
Detailed Organ Effects Table
| Organ / System | Sympathetic Effect | Receptor | Parasympathetic Effect | Receptor |
|---|---|---|---|---|
| Heart - Rate | ↑ Heart rate (tachycardia) | β1 | ↓ Heart rate (bradycardia) | M2 |
| Heart - Contractility | ↑ Force of contraction | β1 | ↓ Slightly | M2 |
| Heart - Conduction (AV node) | ↑ Conduction velocity | β1 | ↓ Conduction (AV block possible) | M2 |
| Blood vessels (most) | Vasoconstriction | α1 | Minimal innervation (vasodilation via NO) | M3 |
| Blood vessels (skeletal muscle) | Vasodilation | β2 | None | |
| Bronchi / Bronchioles | Bronchodilation, ↓ secretions | β2 | Bronchoconstriction, ↑ secretions | M3 |
| Eye - Pupil | Mydriasis (dilates) - radial/dilator muscle contracts | α1 | Miosis (constricts) - sphincter pupillae contracts | M3 |
| Eye - Ciliary muscle | Relaxation → far vision | β | Contraction → near vision (accommodation) | M3 |
| Salivary glands | Thick, viscous saliva (↓ volume) | α1, β | Watery, copious saliva (↑ volume) | M3 |
| Lacrimal glands | No significant innervation | - | ↑ Tear secretion | M3 |
| GI - Motility | ↓ Peristalsis, ↓ tone | α2, β2 | ↑ Peristalsis, ↑ tone | M3 |
| GI - Sphincters | Contracts (closes) | α1 | Relaxes (opens) | M3 |
| GI - Secretions | ↓ | α2 | ↑ (gastric acid, enzymes) | M1, M3 |
| Liver | Glycogenolysis, gluconeogenesis (↑ blood glucose) | β2, α1 | Glycogen synthesis | M |
| Pancreas | ↓ Insulin secretion | α2 | ↑ Insulin and enzyme secretion | M3 |
| Bladder (Detrusor) | Relaxation (allows filling) | β2, β3 | Contraction (micturition) | M3 |
| Bladder (Internal sphincter) | Contracts (retention) | α1 | Relaxes (permits micturition) | M3 |
| Uterus (pregnant) | Contraction | α1 | Variable | |
| Uterus (non-pregnant) | Relaxation | β2 | Variable | |
| Male genitalia | Ejaculation | α1 | Erection (↑ blood flow via NO) | M |
| Kidney (renin) | ↑ Renin secretion | β1 | ↓ Renin | - |
| Skin - Sweat glands | ↑ Sweating (cholinergic!) | M3 | None | |
| Skin - Piloerection | Hair stands up (goosebumps) | α1 | None | |
| Adrenal medulla | ↑ Epi + NE release (via ACh on Nn) | Nn | None | |
| Metabolic | ↑ Glycogenolysis, ↑ lipolysis, ↑ glucose, ↑ FFA | β | Anabolic/storage | - |
Memory trick for erection/ejaculation: "Point and Shoot" - Parasympathetic = erection (Point), Sympathetic = ejaculation (Shoot)
8. STRUCTURES WITH ONLY ONE DIVISION
| Structure | Innervated only by... |
|---|---|
| Blood vessels (most) | Sympathetic only |
| Sweat glands | Sympathetic only (but cholinergic!) |
| Piloerector muscles | Sympathetic only |
| Adrenal medulla | Sympathetic only (preganglionic directly) |
| Lacrimal gland | Parasympathetic only |
| Ciliary muscle | Parasympathetic only |
| Nasopharyngeal glands | Parasympathetic only |
9. NEUROTRANSMITTER SYNTHESIS, STORAGE AND TERMINATION
Norepinephrine (Sympathetic)
- Synthesis: Tyrosine → DOPA → Dopamine → NE (in vesicles) → Epi (adrenal medulla only, via PNMT enzyme)
- Termination: Mainly reuptake into presynaptic terminal (uptake-1 = NET transporter); also COMT (extraneuronal), MAO (intraneuronal)
- Drugs blocking reuptake: Cocaine, tricyclic antidepressants
Acetylcholine (Parasympathetic)
- Synthesis: Choline + Acetyl-CoA → ACh (via choline acetyltransferase, ChAT)
- Termination: Rapid hydrolysis by Acetylcholinesterase (AChE) in synaptic cleft
- Drugs blocking AChE: Neostigmine, physostigmine, organophosphates
10. SECOND MESSENGER SYSTEMS
| Receptor | G Protein | Second Messenger | Effect |
|---|---|---|---|
| α1 adrenergic | Gq | ↑ IP3/DAG → ↑ Ca²⁺ | Contraction, secretion |
| α2 adrenergic | Gi | ↓ cAMP | Inhibition, NE autofeedback |
| β1, β2, β3 adrenergic | Gs | ↑ cAMP → PKA | Relaxation (smooth muscle), ↑HR/contractility (heart) |
| M1, M3, M5 muscarinic | Gq | ↑ IP3/DAG → ↑ Ca²⁺ | Smooth muscle contraction, secretion |
| M2, M4 muscarinic | Gi | ↓ cAMP | ↓ HR, inhibition |
| Nicotinic (Nn, Nm) | None (ion channel) | Na⁺ influx → depolarization | Fast excitation |
11. COMPARISON TABLE - STRUCTURAL SUMMARY
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Origin | T1-L2 (thoracolumbar) | CN III, VII, IX, X + S2-S4 (craniosacral) |
| Preganglionic fiber | Short | Long |
| Postganglionic fiber | Long | Short |
| Ganglion location | Para/prevertebral (near cord) | Terminal (near/in organ) |
| Pre:Post ratio | 1:20+ (divergence) | 1:1-3 (discrete) |
| Preganglionic NT | ACh (Nicotinic Nn) | ACh (Nicotinic Nn) |
| Postganglionic NT | Norepinephrine (adrenergic) | ACh (muscarinic) |
| Postganglionic receptor | Adrenergic (α1, α2, β1, β2, β3) | Muscarinic (M1-M5) |
| Exceptions in NT | Sweat glands = ACh; Adrenal medulla = Epi | None |
| General effect | Catabolic, fight-or-flight | Anabolic, rest-and-digest |
| Distribution | Widespread (entire body) | Selective (mainly head, thorax, abdomen, pelvis) |
12. PHARMACOLOGICAL HANDLE (High-yield for MBBS)
| Drug class | Division | Mechanism | Example | Use |
|---|---|---|---|---|
| Beta-blockers | Block SNS | Block β receptors | Propranolol (β1+β2), Metoprolol (β1) | Hypertension, angina, arrhythmia |
| Alpha-blockers | Block SNS | Block α1 receptors | Prazosin, Tamsulosin | Hypertension, BPH |
| Beta-2 agonists | Mimic SNS | Activate β2 | Salbutamol | Asthma |
| Anticholinergics (antimuscarinics) | Block PSNS | Block M receptors | Atropine | Bradycardia, peptic ulcer, COPD |
| Anticholinesterases | Potentiate PSNS | Block AChE | Neostigmine | Myasthenia gravis, reverse NMJ block |
| Muscarinic agonists | Mimic PSNS | Activate M receptors | Pilocarpine | Glaucoma |
Sources: Neuroanatomy through Clinical Cases 3rd Ed. | Lippincott Illustrated Reviews Pharmacology 7th Ed. | Ganong's Review of Medical Physiology 26th Ed. | Guyton & Hall Textbook of Medical Physiology | Histology - A Text and Atlas (Histology)
How does m3 acting drugs cause hypotension
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Excellent - the textbooks have given the full picture. Here is the complete answer:
How M3-Acting Drugs Cause Hypotension
The Short Answer - A Receptor Correction First
Important note: Katzung's Pharmacology specifically states the vascular vasodilation by muscarinic agonists is mediated via M2 receptors on endothelium (not M3) in intact vessels. However, M3 receptors are present on endothelial cells in some vascular beds (e.g. skeletal muscle via M1/M3), and the mechanism of NO release is the same. For exam purposes in many MBBS curricula, this effect is attributed to M3. The mechanism is identical regardless of which muscarinic subtype is cited.
Step-by-Step Mechanism
Step 1 - Muscarinic Agonist Activates Endothelial Receptors (M2/M3)
When a muscarinic agonist (e.g. ACh, bethanechol, carbachol, pilocarpine) enters the bloodstream, it binds to muscarinic receptors on the vascular endothelium - the inner lining of blood vessels.
- Receptor subtype: M2 (classic) or M3 (in some beds)
- G protein: Gq → activates phospholipase C → ↑ IP3 → ↑ intracellular Ca²⁺ in endothelial cells
Step 2 - eNOS Activation in Endothelium
The rise in intracellular Ca²⁺ inside the endothelial cell:
- Ca²⁺ binds calmodulin
- Ca²⁺-calmodulin complex activates endothelial Nitric Oxide Synthase (eNOS)
- eNOS converts L-arginine → Nitric Oxide (NO)
NO is also known as EDRF - Endothelium-Derived Relaxing Factor (Furchgott & Zawadzki, 1980 - Nobel Prize discovery)
Step 3 - NO Diffuses to Vascular Smooth Muscle
NO is a lipophilic gas - it diffuses freely from the endothelial cell into the adjacent vascular smooth muscle cell.
Step 4 - Activation of Guanylyl Cyclase → ↑ cGMP
Inside the smooth muscle cell:
- NO activates soluble guanylyl cyclase (sGC)
- sGC converts GTP → cyclic GMP (cGMP)
- ↑ cGMP activates Protein Kinase G (PKG)
Step 5 - Smooth Muscle Relaxation → Vasodilation
PKG causes:
- Phosphorylation of myosin light chain kinase (MLCK) → inactivated
- ↓ intracellular Ca²⁺ (Ca²⁺-ATPase activated, Ca²⁺ channels inhibited)
- Result: smooth muscle RELAXES → vessel DILATES
Step 6 - Vasodilation → ↓ Peripheral Vascular Resistance → Hypotension
Vasodilation reduces total peripheral resistance (TPR).
Since: BP = Cardiac Output × TPR
↓ TPR → ↓ Blood Pressure (Hypotension)
Summary Flowchart
Muscarinic agonist (M2/M3)
↓
Endothelial cell: Gq → ↑Ca²⁺ → Ca²⁺-calmodulin → eNOS activated
↓
L-arginine → NITRIC OXIDE (NO)
↓ (diffuses into vascular smooth muscle)
sGC activated → GTP → ↑ cGMP → PKG activated
↓
MLCK inhibited + ↓Ca²⁺ in smooth muscle
↓
VASODILATION
↓
↓ Total Peripheral Resistance
↓
HYPOTENSION
The Critical Paradox - Endothelium Intact vs Absent
This classic experiment (Furchgott & Zawadzki 1980) is a favorite exam topic:
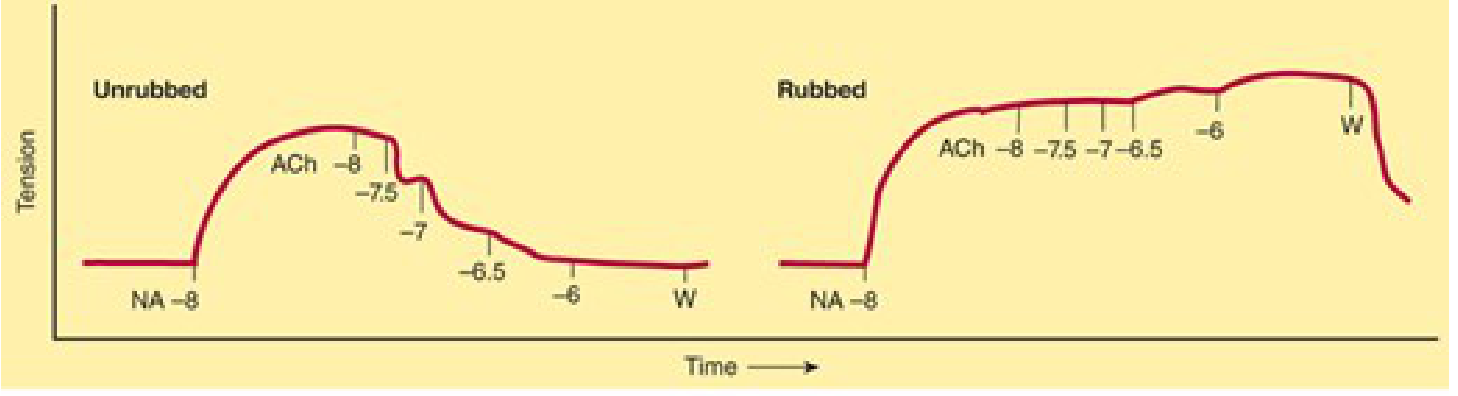
| Condition | Effect of ACh on Blood Vessel |
|---|---|
| Endothelium INTACT (unrubbed) | RELAXATION (vasodilation) - via NO/cGMP |
| Endothelium REMOVED (rubbed) | CONTRACTION (vasoconstriction) - direct M3 on smooth muscle → IP3 → ↑Ca²⁺ |
Key clinical implication: In atherosclerosis, where the endothelium is damaged, ACh (or parasympathetic stimulation) paradoxically causes vasoconstriction instead of vasodilation - a mechanism contributing to angina in diseased coronary arteries.
Additional Mechanisms Contributing to Hypotension
Beyond the NO pathway, muscarinic agonists also lower BP via:
- ↓ Heart rate (M2 on SA node) - bradycardia → ↓ cardiac output
- ↓ AV node conduction (M2) - negative dromotropy
- ↓ Cardiac contractility (M2) - negative inotropy → ↓ cardiac output
- The fall in BP then triggers reflex sympathetic discharge (baroreceptor reflex), which can partially oppose the bradycardia - making the net heart rate effect complex.
Pilocarpine Exception (Exam Favourite)
Pilocarpine IV produces:
- Brief hypotension (M receptor - NO pathway as above)
- Followed by paradoxical hypertension - because it also activates M1 receptors in sympathetic ganglia, causing sympathetic ganglion firing → NE release → vasoconstriction
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed. | Ganong's Review of Medical Physiology 26th Ed. | Barash Clinical Anesthesia 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.