We resusitate the patient ,got the heart beat now what? What we can do to the patient's heart beat not to stop again?
Reading File
Finding Sources
Finding Sources
Searching the Web
post-resuscitation care after ROSC preventing rearrest 2024 guidelines
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have the complete algorithm from the textbook. I have all the information needed for a thorough answer.
Here is what you need to do after achieving Return of Spontaneous Circulation (ROSC) - the structured post-cardiac arrest care approach to prevent re-arrest:
Post-Cardiac Arrest Care After ROSC
The moment the heartbeat returns, you enter a critical phase called post-cardiac arrest care. This is when most secondary deaths and re-arrests happen if management is not aggressive and systematic.
Here is the full Adult Post-Cardiac Arrest Care Algorithm from Morgan & Mikhail's Clinical Anesthesiology:
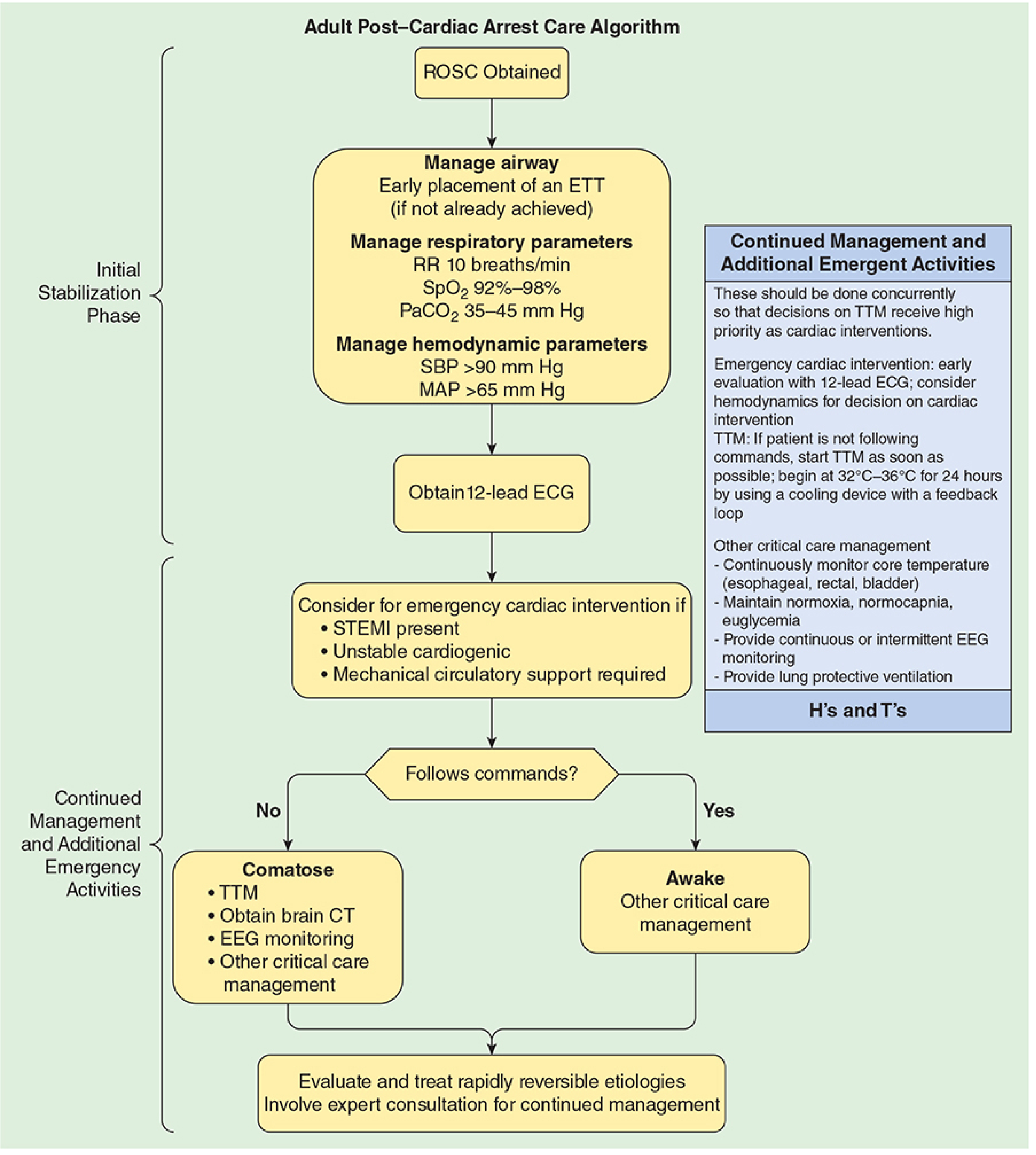
Phase 1: Initial Stabilization (Do Immediately)
1. Airway - Secure It
- If not already intubated, place an endotracheal tube (ETT) immediately
- An unprotected airway is a leading cause of re-arrest from hypoxia
2. Respiratory Parameters - Titrate Carefully
| Target | Value |
|---|---|
| Respiratory Rate | 10 breaths/min |
| SpO2 | 92-98% (NOT 100%) |
| PaCO2 | 35-45 mm Hg (normocapnia) |
Avoid both hyperoxia (causes reperfusion injury) and hypoxia. Avoid hypo/hypercapnia - both worsen cerebral blood flow and outcomes. Use lung-protective ventilation settings.
3. Hemodynamic Parameters - Maintain Perfusion
| Target | Value |
|---|---|
| Systolic BP | > 90 mm Hg |
| Mean Arterial Pressure (MAP) | > 65 mm Hg |
- Post-arrest hypotension occurs in up to 65% of patients within 6 hours of ROSC and is an independent predictor of death (Red Cross/ILCOR guidelines)
- Use IV fluids and vasopressors (norepinephrine, dopamine) as needed to hit these targets
- The 2024 AHA/ILCOR consensus recommends a MAP of at least 60-65 mmHg in adults
Phase 2: Identify and Treat the Cause (The H's and T's)
Re-arrest will happen again if the underlying cause is not fixed. Search for and treat all reversible causes:
| H's | T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins/drug overdose |
| Hypo/Hyperkalemia | Thrombosis - Pulmonary (PE) |
| Hypothermia | Thrombosis - Coronary (MI) |
| Hypoglycemia |
Phase 3: Get a 12-Lead ECG - Check for STEMI
- Obtain a 12-lead ECG as soon as possible
- If STEMI is present, or there is unstable cardiogenic shock, or mechanical circulatory support is needed --> immediate cardiac catheterization / PCI (percutaneous coronary intervention)
- Unrevascularized coronary occlusion is a top cause of re-arrest
Phase 4: Neurological Status and TTM
Ask: Is the patient following commands?
If NOT following commands (comatose):
- Start Targeted Temperature Management (TTM) as soon as possible
- Target core temperature: 32-36°C for 24 hours using a cooling device with feedback loop
- Prevents secondary brain injury from post-arrest cerebral reperfusion damage
- Obtain brain CT scan
- Start continuous or intermittent EEG monitoring (detect and treat seizures - seizures after ROSC worsen outcomes and can cause re-arrest)
- Continuously monitor core temperature (esophageal, rectal, or bladder probe)
If awake and following commands:
- Continue standard critical care management
- Still monitor closely for arrhythmia recurrence
Phase 5: Ongoing Critical Care
- Euglycemia: Control blood sugar - avoid both hypoglycemia and hyperglycemia. Glycemic control in the post-arrest patient significantly impacts outcomes.
- Antiarrhythmic therapy: If the arrest was due to VF/VT, consider IV amiodarone infusion (150 mg over 10 min, then 1 mg/min maintenance) or lidocaine to prevent recurrence.
- Expert consultation: Cardiology, neurology, and critical care involvement for continued management.
- Post-event debriefing of the resuscitation team.
Summary: The 5-Point "Don't Re-Arrest" Plan
| Priority | Action |
|---|---|
| Airway | Intubate, SpO2 92-98%, PaCO2 35-45 |
| Hemodynamics | MAP > 65, SBP > 90 with fluids/vasopressors |
| Cause | Fix the H's and T's, ECG for STEMI/PCI |
| Brain protection | TTM 32-36°C if comatose, EEG for seizures |
| ICU care | Euglycemia, continuous monitoring, antiarrhythmics |
The first hour after ROSC is the most dangerous. Aggressive, protocolized management in an ICU setting is what prevents re-arrest and gives the patient the best chance of survival with neurological recovery.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Fig. 55-14 (Post-Cardiac Arrest Care Algorithm)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 314-320
- ERC/ESICM Post-Resuscitation Care Guidelines 2025
In an emergency situation somehow it's impossible to do ct scan right away , so most of the time patient is unconscious after resuscitation then bp sometimes is High sometimes low and also sometimes normal so in any kind of these situation what we can do? Tell the exact plan or treatment
Finding Sources
Finding Sources
Searching the Web
post-resuscitation unconscious patient BP management hypotension hypertension normotension ICU protocol 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://www.neurocriticalcare.org/Portals/0/ENLS%205.0/ENLS%…
Finding Sources
Finding Sources
I have comprehensive information from both the textbooks and current guidelines (ENLS 6.0 2024, ERC/ESICM 2025, AHA 2024). Let me now compose the detailed, practical answer.
This is one of the most real-world clinical situations - no CT available, patient unconscious, and BP all over the place. Here is the exact plan, broken down by BP scenario.
Post-Resuscitation Management: Unconscious Patient, No CT Available
First - The Universal Steps (Do These No Matter What the BP Is)
These are non-negotiable and come before you even think about BP:
1. Airway - Lock It Down
- Intubate if not already done (RSI with ketamine + succinylcholine or rocuronium)
- Confirm ETT with waveform capnography (EtCO2)
- Set ventilator:
- RR: 10-12 breaths/min
- TV: 6-8 mL/kg ideal body weight (lung-protective)
- SpO2 target: 94-98% - do NOT give 100% O2, it causes cerebral reperfusion injury
- PaCO2 target: 35-45 mm Hg (normocapnia) - avoid both hypo and hypercapnia
2. Lines and Monitoring - Put In Now
- IV access x2 (large bore) or central line
- Arterial line if available (gives you beat-to-beat BP and blood gases)
- Cardiac monitor continuously
- 12-lead ECG immediately - look for STEMI, arrhythmia
- Foley catheter - urine output is your best bedside perfusion marker (target >0.5 mL/kg/hr)
- Check blood glucose - treat hypoglycemia immediately (dextrose 50%, 1 amp)
- Temperature probe (rectal or esophageal) if available
3. Start Targeted Temperature Management (TTM) NOW
Since the patient is unconscious and you cannot do CT, start TTM right away - do not wait:
- Target: 32-36°C for 24 hours
- Use ice packs (axilla, groin, neck), cold IV saline (10-20 mL/kg over 20-30 min), or commercial cooling blanket
- Fever (>37.5°C) after arrest causes severe secondary brain injury - this is your biggest enemy in the absence of CT
- Treat shivering: IV paracetamol 1g, IV magnesium sulfate 2-4g, sedation (propofol infusion 5-50 mcg/kg/min or midazolam 0.02-0.1 mg/kg/hr)
Now - The BP-Specific Plans
SCENARIO A: HYPOTENSION (SBP < 90 mmHg / MAP < 65 mmHg)
This is the most dangerous scenario and the #1 cause of re-arrest after ROSC. It happens in ~65% of patients within 6 hours.
Causes to consider simultaneously:
- Myocardial stunning (most common - heart is stunned from arrest)
- Hypovolemia (from CPR, fluids lost, bleeding)
- Tension pneumothorax (decompress if suspected - needle 2nd ICS MCL, then chest tube)
- Cardiac tamponade (Beck's triad? Do bedside ultrasound/FAST if available)
- Massive PE (history? preceding collapse?)
Step-by-step treatment:
Step 1 - Fluid challenge first (unless lungs are wet)
- IV crystalloid bolus: 250-500 mL normal saline or Ringer's lactate over 10-15 minutes
- Reassess BP and lung sounds after each bolus
- If crackles appear or SpO2 drops - STOP fluids, switch to vasopressors
Step 2 - Start Vasopressor (do not delay)
| Drug | Dose | When to Use |
|---|---|---|
| Norepinephrine (1st choice) | 0.1-0.5 mcg/kg/min IV infusion | All post-arrest hypotension |
| Dopamine (2nd choice) | 5-20 mcg/kg/min IV infusion | If norepinephrine unavailable |
| Epinephrine | 0.1-0.5 mcg/kg/min | Low cardiac output / norepinephrine failing |
| Vasopressin | 0.03-0.04 units/min infusion | Add-on when norepinephrine insufficient |
- Titrate to MAP ≥ 65 mmHg (this protects the brain and coronary circulation)
- If MAP still cannot reach 65 despite norepinephrine + vasopressin - add epinephrine (suggests myocardial stunning / cardiogenic shock)
Step 3 - If cardiogenic shock suspected (stunned heart)
- Add dobutamine 2.5-10 mcg/kg/min (inotrope) alongside the vasopressor
- Consider balloon pump if available at the receiving center
- This patient needs urgent echo and cardiology
SCENARIO B: HYPERTENSION (SBP > 160 mmHg / MAP > 110 mmHg)
This is actually less common but can occur due to catecholamine surge from the arrest itself. In an unconscious patient without CT, hypertension is a red flag for:
- Intracranial hemorrhage causing Cushing's reflex (high BP + bradycardia + irregular breathing = brain herniation)
- Extreme sympathetic surge post-arrest
What to do:
First - Do NOT aggressively lower BP without knowing the cause
- If you suspect Cushing's response (very high BP + bradycardia + irregular/slow respirations), the cause is intracranial pressure - lowering BP here can be fatal. In this case:
- Head of bed at 30°
- Mannitol 0.5-1 g/kg IV over 20 min or hypertonic saline 3% (100-150 mL over 20 min)
- Urgent neurosurgical consultation
- This patient absolutely needs CT as soon as possible - transfer if necessary
If BP is high but patient has no signs of Cushing's (normal HR, normal breathing pattern):
- Often self-resolves as catecholamine surge settles
- Gentle sedation: propofol infusion (titratable, short-acting) or IV labetalol 10-20 mg slow push (has both alpha and beta blockade, does not drop BP suddenly)
- Target: MAP 80-100 mmHg (do NOT bring to "normal" - the brain needs higher perfusion after arrest)
- Avoid nitroprusside and hydralazine in unconscious post-arrest patients - they cause unpredictable drops and can worsen cerebral perfusion
SCENARIO C: NORMAL BP (SBP 90-160, MAP 65-100)
Do not relax - this patient is still critically unstable.
What to do:
- Keep all the universal steps running (airway, TTM, monitoring)
- Start a maintenance IV infusion at ~75-100 mL/hr
- Have vasopressors drawn up and ready to start at bedside
- Recheck BP every 5-10 minutes for the first hour (BP post-arrest can crash suddenly due to myocardial stunning developing over time)
- 12-lead ECG - look for STEMI (can have normal BP and still have an occluded coronary)
- Treat any arrhythmia that appears:
- VT/VF recurrence: Amiodarone 150 mg IV over 10 min, then 1 mg/min infusion for 6 hours
- Bradycardia (HR < 50 with poor BP): Atropine 0.5 mg IV (can repeat up to 3 mg total), then transcutaneous pacing
The "Bedside Bundle" When No CT Is Available
Since you cannot get CT, do these bedside assessments to guide management:
| Bedside Tool | What You're Looking For |
|---|---|
| 12-lead ECG | STEMI (send for PCI), arrhythmia |
| Lung auscultation | Absent breath sounds = pneumothorax |
| FAST/bedside ultrasound (if available) | Tamponade, free fluid, cardiac motion |
| Pupils | Fixed dilated = herniation or drugs; unequal = ICH |
| Blood glucose | Hypoglycemia mimics and worsens coma |
| Temperature | Fever = infection or hyperthermia causing damage |
| Urine output | < 0.5 mL/kg/hr = inadequate perfusion |
| EtCO2 waveform | Declining trend = falling cardiac output |
Summary Card
UNCONSCIOUS POST-ROSC PATIENT - NO CT AVAILABLE
ALWAYS:
✓ Intubate → SpO2 94-98%, RR 10, PaCO2 35-45
✓ 12-lead ECG → STEMI? Arrhythmia?
✓ Blood glucose → fix if low
✓ Start cooling (TTM 32-36°C)
✓ Sedation infusion (propofol or midazolam)
✓ Continuous monitoring + foley
LOW BP (MAP < 65):
✓ 250-500 mL fluid bolus → reassess
✓ Norepinephrine infusion 0.1-0.5 mcg/kg/min
✓ Add vasopressin or epinephrine if fails
✓ Dobutamine if cardiogenic shock
HIGH BP (SBP >160):
✓ Check pupils + HR + breathing (Cushing's?)
✓ If Cushing's: mannitol + 30° HOB
✓ If catecholamine surge: propofol or labetalol
✓ Target MAP 80-100, NOT normal
NORMAL BP:
✓ IV maintenance running
✓ Vasopressors drawn up at bedside
✓ Recheck every 5-10 min x 1 hour
✓ Treat arrhythmia (amiodarone for VT/VF)
The core principle across all BP scenarios is: the brain drives every decision. When there is no CT, treat empirically to protect cerebral perfusion pressure - never let MAP fall below 65, never give 100% oxygen, never hyperventilate, and start cooling as fast as possible.
Sources: ENLS Protocol v6.0 - Resuscitation Following Cardiac Arrest | ERC/ESICM Post-Resuscitation Guidelines 2025 | AHA 2024 International Consensus | Morgan & Mikhail's Clinical Anesthesiology, 7e | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.