explain the shoulder joint to me
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have rich, detailed content from Gray's Anatomy for Students plus two outstanding anatomical diagrams. I have everything needed for a thorough explanation. Let me now compile the full answer.
The Shoulder (Glenohumeral) Joint
Overview
The shoulder joint - formally the glenohumeral joint - is a multiaxial ball-and-socket synovial joint between the large spherical head of the humerus and the small, shallow glenoid cavity of the scapula. It has the greatest range of motion of any joint in the body, but this mobility comes directly at the cost of bony stability. Stability is therefore achieved by soft-tissue structures: the rotator cuff muscles, the glenoid labrum, and surrounding ligaments.
1. Articular Surfaces
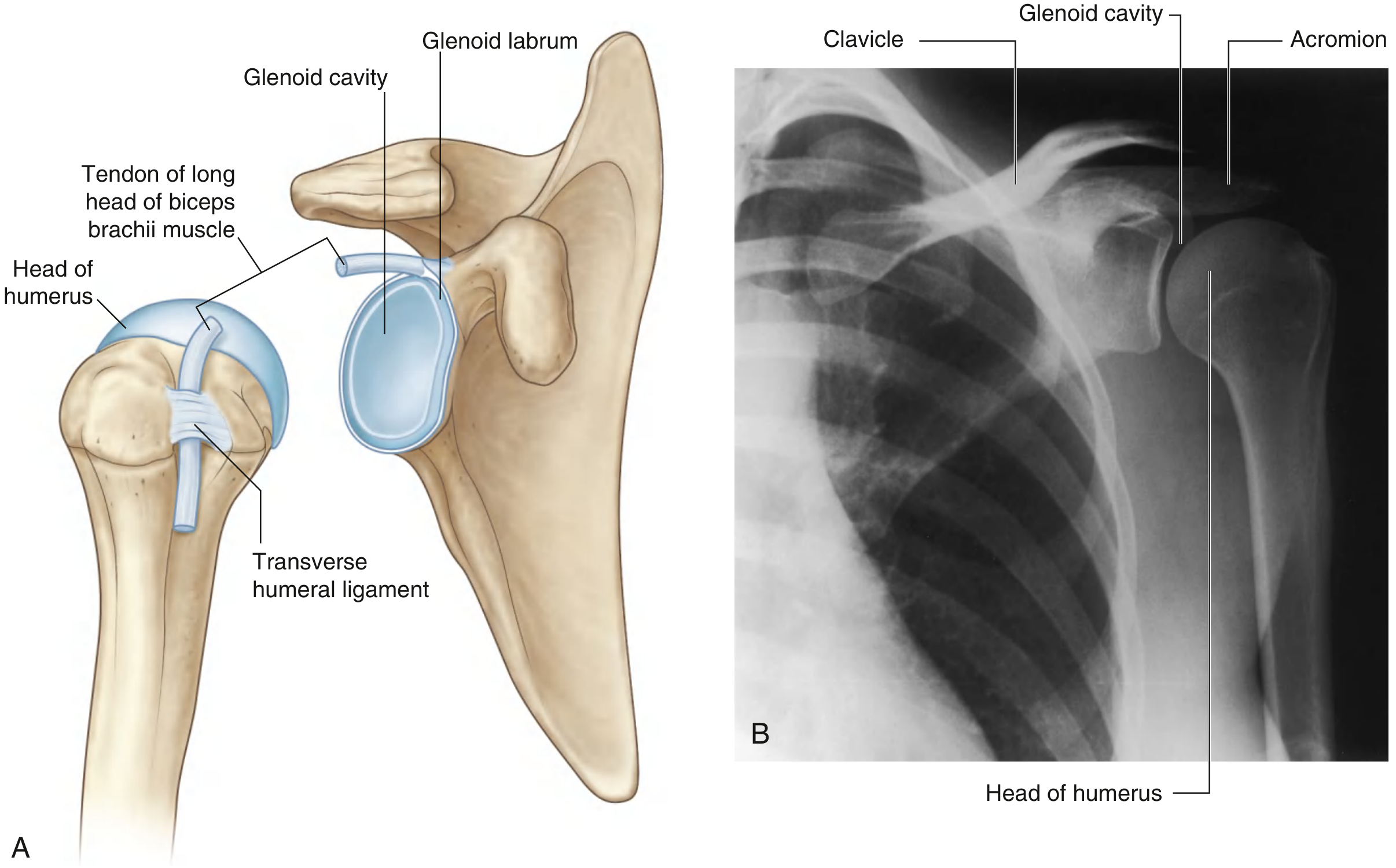
- Head of the humerus - large, spherical, covered by hyaline cartilage. Faces medially, superiorly, and posteriorly.
- Glenoid cavity of the scapula - small, shallow, pear-shaped fossa also covered by hyaline cartilage. Only about one-quarter to one-third of the humeral head articulates with it at any one time.
The size mismatch is the key feature: it grants enormous mobility but demands soft-tissue stabilizers to prevent dislocation.
2. Glenoid Labrum
The glenoid cavity is deepened and expanded at its periphery by a fibrocartilaginous collar - the glenoid labrum - which attaches around the rim of the fossa. Superiorly, the labrum is continuous with the tendon of the long head of biceps brachii, which attaches to the supraglenoid tubercle and passes through the joint cavity superior to the humeral head. The labrum effectively increases the contact area and adds roughly 50% more depth to the socket.
3. Joint Capsule
The fibrous membrane of the joint capsule:
- Attaches to the margin of the glenoid cavity (outside the labrum) and to the anatomical neck of the humerus
- On the humerus, the medial attachment extends further inferiorly onto the shaft - creating a loose, redundant inferior fold that accommodates full abduction
- Contains openings that allow the synovial membrane to bulge outward and form bursae
The synovial membrane lines the inner surface of the fibrous membrane, is loose inferiorly, and also wraps around the tendon of the long head of biceps as it runs through the joint and into the intertubercular sulcus (bicipital groove).
4. Ligaments
The fibrous capsule is reinforced by several key ligaments:
| Ligament | Attachment | Function |
|---|---|---|
| Superior glenohumeral | Superomedial glenoid → lesser tubercle | Limits inferior translation; forms part of the rotator interval |
| Middle glenohumeral | Upper glenoid margin → anatomical neck | Limits external rotation at lower angles of abduction |
| Inferior glenohumeral | Inferior glenoid margin → anatomical neck (3 parts: anterior/posterior bands + axillary recess) | Most important stabilizer; limits anterior-inferior instability during abduction. Functions as a "hammock" |
| Coracohumeral | Base of coracoid process → greater and lesser tubercles | Limits inferior translation; stabilizes long head of biceps in the bicipital groove |
| Transverse humeral | Greater tubercle → lesser tubercle | Holds the tendon of the long head of biceps in the intertubercular sulcus |
The capsule is notably thinner and looser posteriorly - which is why anterior dislocations are far more common (the humeral head escapes inferiorly and anteriorly).
There is also a bony-ligamentous arch formed above the joint by the coracoacromial ligament spanning the coracoid process to the acromion - this protects the joint superiorly.
5. Bursae
Several bursae reduce friction around the joint:
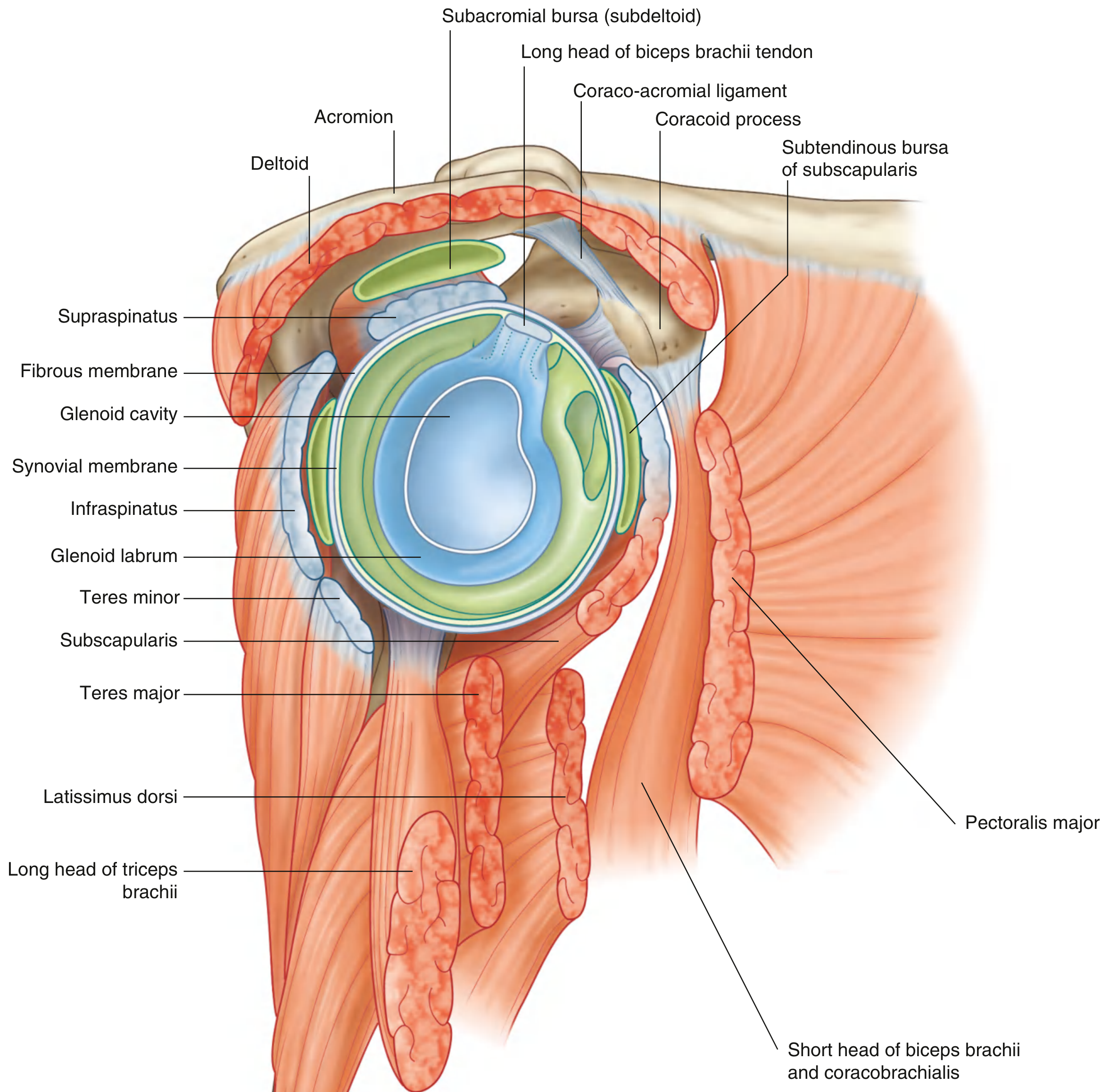
- Subacromial (subdeltoid) bursa - between the acromion/deltoid and the supraspinatus tendon/joint capsule. This does NOT communicate with the joint normally, but rupture of the rotator cuff can open communication.
- Subtendinous bursa of subscapularis - between the subscapularis tendon and the fibrous membrane. Communicates with the joint through a gap in the capsule.
- Bursa between the coracoid process and the joint capsule.
6. The Rotator Cuff (SITS)
The rotator cuff is the primary dynamic stabilizer. Four muscles form a musculotendinous collar that blends with the joint capsule around the posterior, superior, and anterior aspects of the joint:
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Supraspinatus | Supraspinous fossa of scapula | Greater tubercle (superior facet) | Initiates abduction (first 15°), depresses humeral head |
| Infraspinatus | Infraspinous fossa of scapula | Greater tubercle (middle facet) | Lateral (external) rotation |
| Teres minor | Lateral border of scapula | Greater tubercle (inferior facet) | Lateral rotation |
| Subscapularis | Subscapular fossa (anterior scapula) | Lesser tubercle | Medial (internal) rotation; sole anterior rotator cuff muscle |
The cuff holds the humeral head compressed into the glenoid cavity throughout movement. The long head of biceps brachii (passing over the top of the humeral head inside the joint) also contributes by resisting upward translation of the humerus.
7. Movements and Range of Motion
The glenohumeral joint performs six movements:
| Movement | Primary Muscles | Approximate Range |
|---|---|---|
| Flexion | Anterior deltoid, pectoralis major (clavicular head), coracobrachialis | 0-180° (with scapular rotation) |
| Extension | Posterior deltoid, latissimus dorsi, teres major | 0-60° |
| Abduction | Supraspinatus (0-15°), then middle deltoid | 0-120° glenohumeral; up to 180° with scapulothoracic contribution |
| Adduction | Pectoralis major, latissimus dorsi, teres major | - |
| Medial rotation | Subscapularis, pectoralis major, latissimus dorsi, teres major, anterior deltoid | 0-70° |
| Lateral rotation | Infraspinatus, teres minor, posterior deltoid | 0-90° |
| Circumduction | Combination of all the above | - |
Full arm elevation to 180° requires a 2:1 glenohumeral-to-scapulothoracic rhythm: for every 3° of elevation, 2° occurs at the glenohumeral joint and 1° at the scapulothoracic articulation.
8. Vascular Supply
The glenohumeral joint is supplied predominantly by:
- Anterior and posterior circumflex humeral arteries (branches of the axillary artery)
- Suprascapular artery (branch of the thyrocervical trunk)
9. Nerve Supply
The joint is innervated by branches from the posterior cord of the brachial plexus and from the:
- Suprascapular nerve (C5, C6)
- Axillary nerve (C5, C6)
- Lateral pectoral nerve (C5, C6, C7)
This follows Hilton's Law: the nerves supplying a joint are the same nerves that supply the muscles acting across it.
10. Why the Shoulder Dislocates So Easily
The combination of a shallow socket, loose inferior capsule, and reliance on muscles (rather than bony constraint) makes the shoulder the most frequently dislocated major joint. The common mechanism is a fall on an outstretched hand with the arm abducted and externally rotated - the humeral head is levered out anteriorly and inferiorly, tearing the anterior inferior labrum (a Bankart lesion) and often leaving an impression fracture on the posterolateral humeral head (a Hill-Sachs lesion).
Sources: Gray's Anatomy for Students, pp. 826-829; General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy, p. 285.
This is a shared conversation. Sign in to Orris to start your own chat.