Write a short note on RS Cells
Reading File
Finding Sources
Searching PubMed
Reed-Sternberg cells Hodgkin lymphoma
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive note on Reed-Sternberg (RS) cells, sourced from Robbins, Cotran & Kumar Pathologic Basis of Disease and Robbins & Kumar Basic Pathology:
Reed-Sternberg (RS) Cells
Definition
RS cells are the large, neoplastic giant cells that are pathognomonic of Hodgkin lymphoma (HL). Their identification in a background of non-neoplastic inflammatory cells is mandatory for the diagnosis of HL.
Morphology
The diagnostic (classic) RS cell is:
- Very large (~45 µm in diameter)
- Binucleated or multinucleated (or a single nucleus with multiple lobes)
- Each nucleus/lobe contains a large, prominent, inclusion-like nucleolus (~5-7 µm) - the size of a small lymphocyte, giving the classic "owl-eye" appearance
- Surrounded by abundant pale cytoplasm
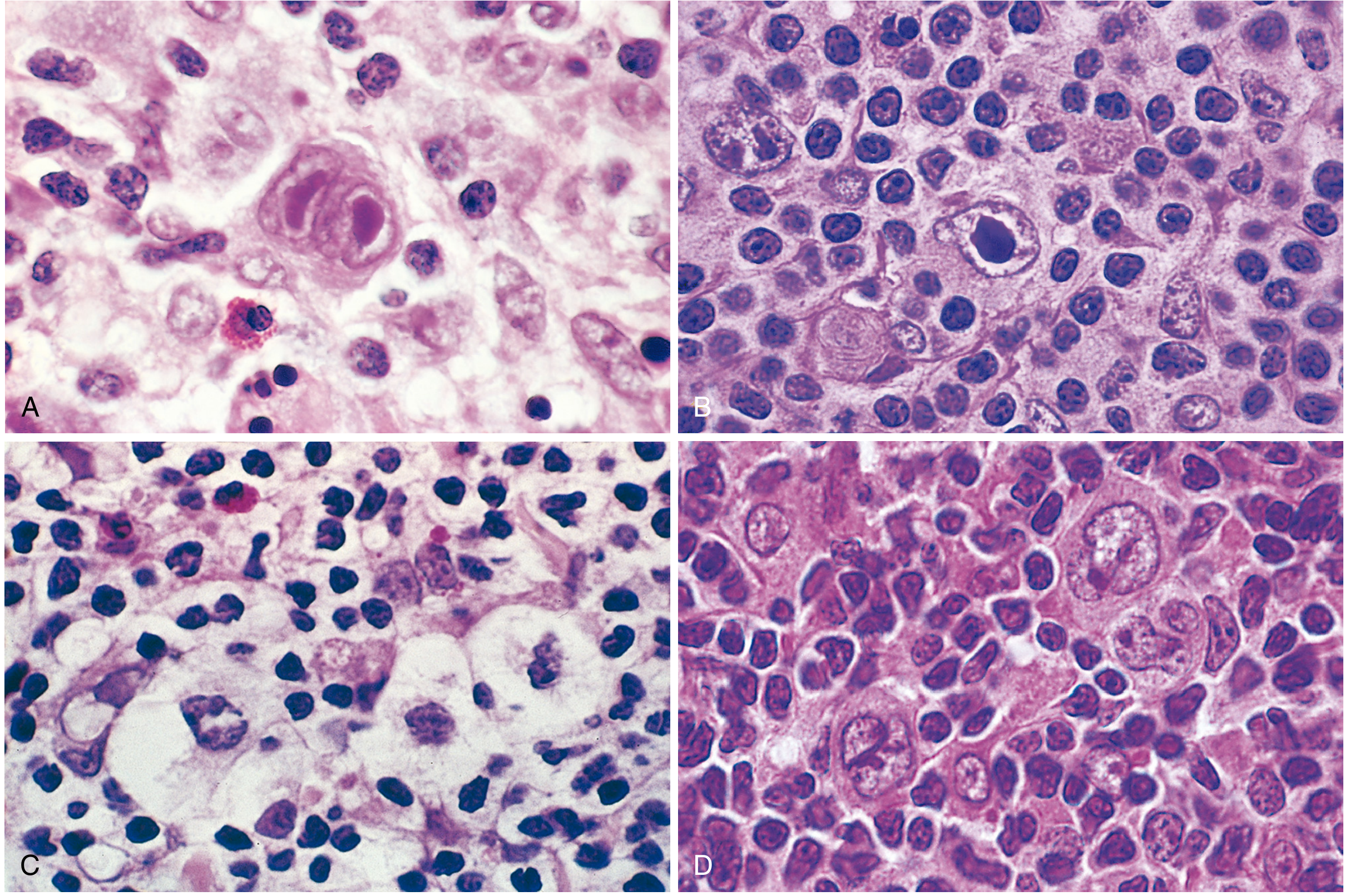
RS Cell Variants
| Variant | Features | Associated Subtype |
|---|---|---|
| Classic (diagnostic) RS cell | Binucleate, owl-eye nucleoli, abundant cytoplasm | All classic HL subtypes |
| Mononuclear (Hodgkin cell) | Single nucleus with large inclusion-like nucleolus | All classic subtypes |
| Lacunar cell | Folded/multilobated nucleus, pale cytoplasm; sits in a clear space (artifact of formalin fixation) | Nodular sclerosis |
| Lymphohistiocytic (L&H / "Popcorn" cell) | Multiple infolded nuclear membranes, small nucleoli, fine chromatin, abundant pale cytoplasm | Nodular lymphocyte predominant HL |
Cell of Origin
RS cells originate from germinal center (or post-germinal center) B cells. This was established by molecular studies on single microdissected RS cells, which showed:
- Clonal IGH gene rearrangements
- Evidence of somatic hypermutation of immunoglobulin genes
Despite this B-cell origin, classic RS cells paradoxically fail to express most B-cell genes, including immunoglobulin genes - likely due to widespread epigenetic reprogramming.
Immunophenotype
| Marker | Classic RS cell | L&H (Popcorn) cell |
|---|---|---|
| CD30 | + | - |
| CD15 | + | - |
| PAX5 | + (weak) | + |
| CD20 | - | + |
| CD45 (LCA) | - | + |
| EBV (LMP-1) | Variable | - |
Pathogenesis
The key molecular event in classic HL is activation of NF-κB, which promotes RS cell growth and survival. This occurs via:
- EBV infection - LMP-1 (a viral latent membrane protein) directly activates NF-κB. EBV is found in RS cells in ~70% of mixed-cellularity HL and a smaller fraction of other classic subtypes.
- Loss-of-function mutations in IκB or TNF-α-induced protein 3 (negative regulators of NF-κB) - in EBV-negative tumors.
- REL proto-oncogene copy number gains on chromosome 2p.
RS cells are aneuploid with diverse chromosomal aberrations.
Immune Evasion
RS cells actively suppress anti-tumor immunity:
- Overexpression of PD-L1 and PD-L2 (encoded on chromosome 9p) - these immune checkpoint ligands antagonize cytotoxic T-cell responses.
- Loss of β2-microglobulin function - prevents expression of MHC class I molecules, so RS cells are invisible to cytotoxic T cells.
- Despite generating a florid reactive inflammatory infiltrate (via cytokines such as IL-5, IL-10, eotaxin, TGF-β), the host immune response is entirely ineffective.
Reactive Background & Cytokine Environment
RS cells secrete cytokines that attract a reactive background infiltrate, which in turn feeds RS cell survival:
- IL-5 - attracts eosinophils
- TGF-β - fibrogenic (responsible for sclerosis in nodular sclerosis HL)
- IL-13 - may stimulate RS cell growth via autocrine signaling
- Eotaxin - chemotactic for eosinophils
Eosinophils and T cells in the background express CD30L and CD40L, which activate CD30/CD40 on RS cells and further upregulate NF-κB - a positive feedback loop.
RS-like Cells in Other Conditions
Classic RS-like cells are not exclusive to Hodgkin lymphoma. Similar-appearing cells may be seen in:
- Infectious mononucleosis
- Certain non-Hodgkin lymphomas
- Solid tissue cancers
Diagnosis of HL therefore requires RS cells in the correct morphologic and immunophenotypic context, confirmed by immunohistochemistry (CD15+, CD30+, CD45-).
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 573-575; Robbins & Kumar Basic Pathology, pp. 417-418
This is a shared conversation. Sign in to Orris to start your own chat.