Community acquired pneumonia
Reading File
Finding Sources
Searching PubMed
"community-acquired pneumonia"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent — I now have very comprehensive data. I have epidemiology, pathobiology, clinical features, microbiology, severity scoring (ATS/IDSA criteria), treatment algorithms, and the ICU flowchart. Let me now synthesize a comprehensive, well-structured answer.
Community-Acquired Pneumonia (CAP)
Definition
CAP is an acute infection of the alveolar parenchyma in a patient who was not hospitalized or residing in a long-term care facility ≥14 days before presentation. It is distinct from hospital-acquired pneumonia (HAP, ≥48 h after admission), ventilator-associated pneumonia (VAP), and healthcare-associated pneumonia (HCAP).
Epidemiology
- ~3 million cases and 1.6 million hospitalizations annually in the United States — the most common infectious cause of hospitalization and death
- Hospitalization rates increase exponentially with age: ~1–2/1000 in young adults → ~40/1000 in adults ≥85 years
- ~35% of CAP hospitalizations occur in patients with recent healthcare exposures; ~25% in immunocompromised patients
- Mortality: ~6% in-hospital, rising to ~15% by 30 days in hospitalized patients
- Seasonal peaks (November–March) coincide with influenza, RSV, and other respiratory viruses
- SARS-CoV-2 has become a major viral cause of CAP during and after the pandemic
— Goldman-Cecil Medicine, p. 990–993
Pathobiology
The primary mechanism for most bacterial CAP is microaspiration of oropharyngeal flora. In a healthy lung, three factors maintain equilibrium: immigration, elimination, and relative reproduction rates of microbes. Disease results when any of these are disrupted:
- Increased immigration: GERD, supine position, nasogastric tube, dysphagia
- Decreased elimination: impaired cough/ciliary function, obstructing lesions, immunosuppression
- Microenvironment changes: smoking damage, aging, COPD, bronchiectasis
Hematogenous seeding (e.g., right-sided endocarditis → S. aureus pneumonia) is less common but important. Viruses spread by aerosol/fomites and may facilitate bacterial co-infection (notably influenza + S. pneumoniae or S. aureus).
Aging is the single strongest risk factor — impairs stem cell reserves, mucociliary function, upregulates surface receptors that increase bacterial adhesion, and augments chronic inflammation.
Microbiology
A specific pathogen is not identified in >50% of cases. When identified:
| Setting | Likely pathogens |
|---|---|
| Outpatient, no comorbidities | S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae, respiratory viruses |
| Outpatient, with cardiopulmonary disease | Above + DRSP, enteric Gram-negatives, anaerobes |
| Inpatient, non-ICU | S. pneumoniae (incl. DRSP), H. influenzae, atypicals, mixed infections, enteric GNRs, Legionella |
| Severe CAP / ICU, no Pseudomonas risk | S. pneumoniae, Legionella, H. influenzae, enteric GNRs, S. aureus (incl. CA-MRSA), M. pneumoniae, viruses |
| Severe CAP / ICU, with Pseudomonas risk | All above + P. aeruginosa |
Two organisms causing the most severe CAP in otherwise healthy adults: S. pneumoniae and Legionella.
Risk factors for specific organisms:
- DRSP: Age >65, β-lactam therapy in past 3 months, alcoholism, day care exposure, immunosuppression
- Enteric GNRs / Pseudomonas: Nursing home, structural lung disease (bronchiectasis), corticosteroids >10 mg/day, broad-spectrum antibiotics >7 days in past month, malnutrition
- MDR pathogens: Hospitalization ≥2 days in past 90 days, immunosuppression, prior respiratory isolation of MRSA or P. aeruginosa
- CA-MRSA: Severe necrotizing CAP following influenza
— Fishman's Pulmonary Diseases & Disorders, p. 2202
Clinical Features
Symptoms (frequency in published series):
- Cough: 79–91%
- Fatigue: ~90%
- Fever: 71–75%
- Dyspnea: 67–75%
- Sputum production: 60–65%
- Pleuritic chest pain: 39–49%
The classic pneumococcal presentation — abrupt fever, single severe rigor, bloody sputum, pleuritic pain — is uncommon in practice. Many presentations are atypical, especially in the elderly (confusion, functional decline without fever) or with atypical organisms (headache, GI symptoms, dry cough).
Examination findings: inspiratory crackles (alveolar fluid), bronchial breath sounds (consolidation), dullness + absent breath sounds (pleural effusion), rhonchi/wheeze (bronchial congestion).
Laboratory: Leukocytosis (or leukopenia in severe disease), elevated bilirubin/LFTs, hyponatremia (especially Legionella).
Diagnosis
Chest Imaging
- CXR is required to confirm the diagnosis — infiltrates may be lobar, segmental, interstitial, or multilobar
- Radiographic findings are nonspecific and do not differentiate causative organisms
- Immunocompromised patients may have normal CXR despite clinical disease
- Clinical and radiographic findings may be discordant (patient improving, CXR worsening — this is common early)
- CT chest is more sensitive and should be used when CXR is negative but clinical suspicion remains high
Microbiological Workup
Guided by severity:
| Test | When to obtain |
|---|---|
| Blood cultures (×2) | Hospitalized patients, severe CAP, ICU |
| Sputum Gram stain + culture | Good-quality sputum in hospitalized patients |
| Urine Legionella antigen | Severe CAP, ICU, epidemiologic risk |
| Urine pneumococcal antigen | Hospitalized / severe CAP |
| Respiratory viral panel (PCR) | All hospitalized CAP (guides de-escalation) |
| Procalcitonin | Helpful to support bacterial diagnosis and guide antibiotic duration |
| Bronchoscopy/BAL | Mechanically ventilated, immunocompromised, no response to empiric therapy |
Severity Scoring — Site-of-Care Decision
CURB-65 (simple bedside tool)
One point each for: Confusion, Urea >7 mmol/L (BUN >20 mg/dL), Respiratory rate ≥30/min, Blood pressure <90 systolic or ≤60 diastolic, age ≥65:
- Score 0–1 → outpatient
- Score 2 → consider hospitalization
- Score ≥3 → hospitalize (score ≥4/5 → consider ICU)
PSI (Pneumonia Severity Index / PORT Score)
5-class scoring system incorporating demographics, comorbidities, exam, and labs — more validated but more complex. Class I–II → outpatient; Class III → observation; Class IV–V → inpatient.
ATS/IDSA Criteria for Severe CAP (ICU Admission)
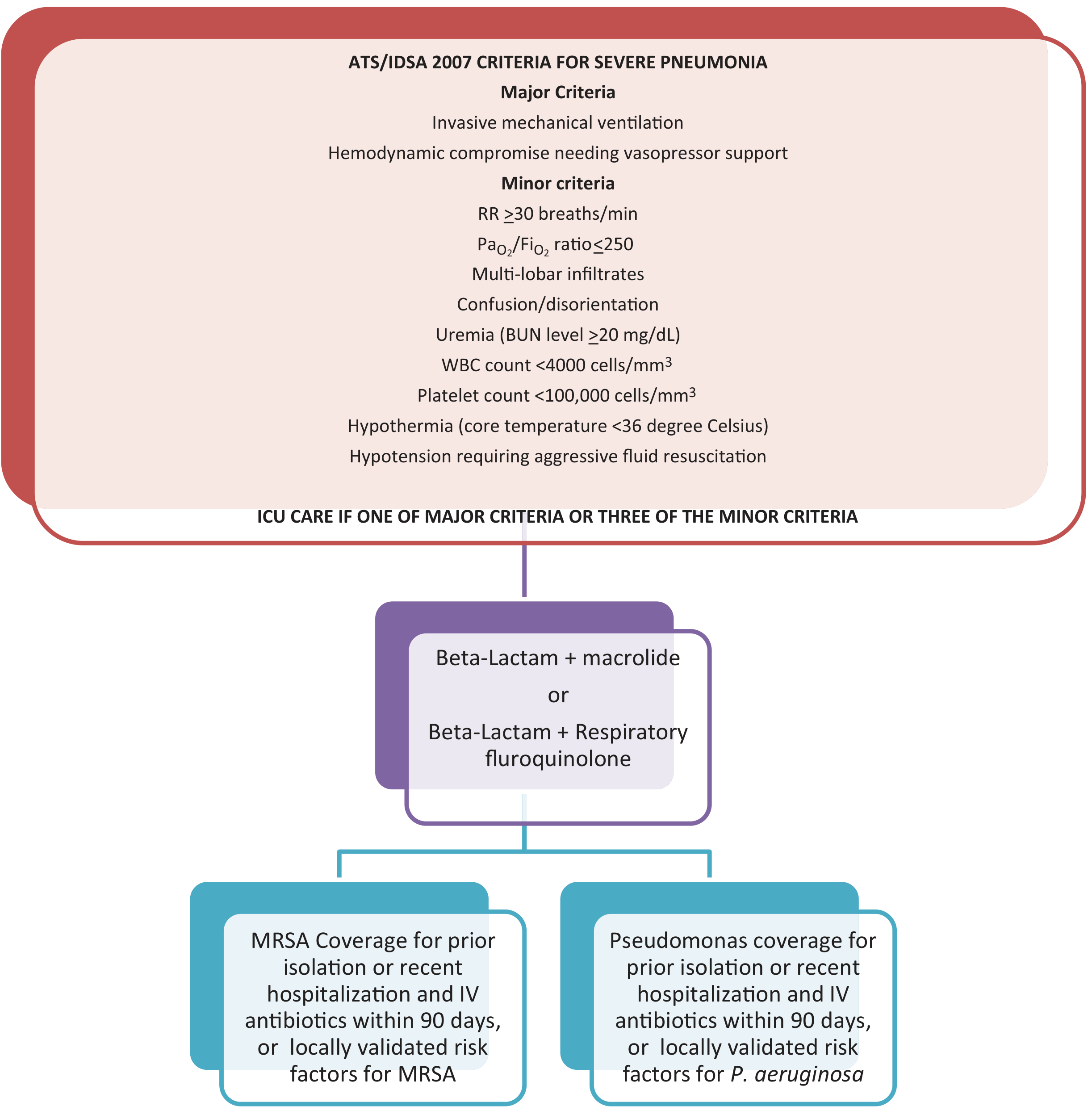
1 major criterion OR ≥3 minor criteria → ICU admission
Major criteria:
- Invasive mechanical ventilation
- Hemodynamic compromise requiring vasopressor support
Minor criteria: RR ≥30/min · PaO₂/FiO₂ ≤250 · Multilobar infiltrates · Confusion/disorientation · BUN ≥20 mg/dL · WBC <4,000/mm³ · Platelets <100,000/mm³ · Core temp <36°C · Hypotension requiring aggressive fluid resuscitation
Treatment
Outpatient CAP
| Patient type | Preferred regimen |
|---|---|
| No comorbidities, low risk | Amoxicillin monotherapy OR doxycycline OR azithromycin (if low local pneumococcal resistance) |
| With comorbidities (COPD, DM, CHF, etc.) | Respiratory fluoroquinolone (levofloxacin, moxifloxacin) OR β-lactam + macrolide |
Newer guidelines (IDSA/ATS 2019) permit β-lactam monotherapy in low-risk outpatient CAP — a change from prior universal atypical coverage.
Inpatient (Non-ICU)
- β-lactam + macrolide (e.g., ceftriaxone + azithromycin) — first-line
- Respiratory fluoroquinolone monotherapy (levofloxacin or moxifloxacin) — alternative
- Add MRSA/Pseudomonas coverage only if:
- Prior respiratory isolation of the organism, OR
- Hospitalization + IV antibiotics within 90 days + locally validated risk factors
Severe CAP (ICU)
- β-lactam + macrolide OR β-lactam + respiratory fluoroquinolone — mandatory combination therapy; monotherapy is never appropriate in ICU patients
- Add anti-MRSA coverage (vancomycin or linezolid) if prior isolation of MRSA or recent hospitalization/IV antibiotics within 90 days
- Add anti-Pseudomonal β-lactam (piperacillin-tazobactam, cefepime, or imipenem) if Pseudomonas risk factors present
- For CA-MRSA necrotizing CAP: linezolid alone OR vancomycin + clindamycin (toxin inhibition)
Duration
- Typically 5 days for mild-moderate CAP with clinical stability
- More prolonged for severe, bacteremic, or complicated cases
- Procalcitonin-guided de-escalation is guideline-supported
Aspiration Pneumonia
Routine additional anaerobic coverage is not recommended by current IDSA/ATS guidelines — most aspiration pneumonias are caused by Gram-negative pathogens, not oral anaerobes.
Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion | ~25% of pneumococcal pneumonia; thoracentesis if moderate-to-large |
| Empyema | 3–5% of hospitalized CAP; requires drainage + prolonged antibiotics |
| Lung abscess | Associated with aspiration, anaerobes, CA-MRSA |
| Respiratory failure | ARDS spectrum; may require intubation/HFNC |
| Cardiac events | AF, new/worsening HF, myocardial ischemia — develop in ~20–25% of hospitalized CAP patients |
| Septic shock | Multi-organ failure, especially with asplenia, pneumococcemia |
Prevention
- Pneumococcal vaccines: PCV15/PCV20 (preferred) or PCV13 + PPSV23 — recommended for all adults ≥65, younger adults with risk factors (asplenia, immunosuppression, chronic lung/heart/liver/kidney disease, diabetes, smokers)
- Influenza vaccine: Annual; reduces risk of influenza-associated bacterial superinfection pneumonia
- COVID-19 vaccines (updated formulations)
- Smoking cessation, optimizing underlying comorbidities
2026 Guideline Update
A new ATS Clinical Practice Guideline for CAP was published January 2026 (PMID 40679934). Key updates include refined antibiotic selection, de-escalation strategies, and updated recommendations on diagnostic testing — this supersedes the 2019 IDSA/ATS guidelines. A parallel French (SPILF/SPLF) guideline update was also published in 2025 (PMID 40037948).
A 2025 systematic review (PMID 40107661) characterized risk factors for drug-resistant pathogens in CAP, informing empiric coverage decisions.
Sources: Goldman-Cecil Medicine (pp. 990–993), Fishman's Pulmonary Diseases & Disorders (pp. 2202–2204), Tintinalli's Emergency Medicine (Chapter 65)
This is a shared conversation. Sign in to Orris to start your own chat.