MC congenital cataract
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
congenital cataract types lamellar zonular nuclear
Loading Image
Here is a comprehensive summary of congenital cataract based on authoritative ophthalmology textbooks:
Most Common (MC) Congenital Cataract
MC Type: Zonular (Lamellar) Cataract
White opacities that surround the nucleus with alternating clear and white cortical lamellae resembling an onion skin pattern. This is the most common morphological type of congenital cataract. — Wills Eye Manual
Epidemiology
- Occurs in ~3 in 10,000 live births
- 2/3 are bilateral; 1/3 are unilateral
- A cause is identified in ~50% of bilateral cases
Aetiology (Rule of Thirds)
| Category | Details |
|---|---|
| Inherited (~1/3) | AD is MC (most common aetiological factor overall) |
| Systemic disease (~1/3) | Metabolic, chromosomal, intrauterine infections |
| Idiopathic (~1/3) | Unknown cause |
Unilateral cataracts are usually sporadic, without family history or systemic disease.
MC Inheritance: Autosomal Dominant
Familial cataracts can be AD (most common), AR, or rarely X-linked recessive (Nance–Horan syndrome). Phenotype varies in cataract morphology and timing of onset.
Types of Congenital Cataract (with slit-lamp images)
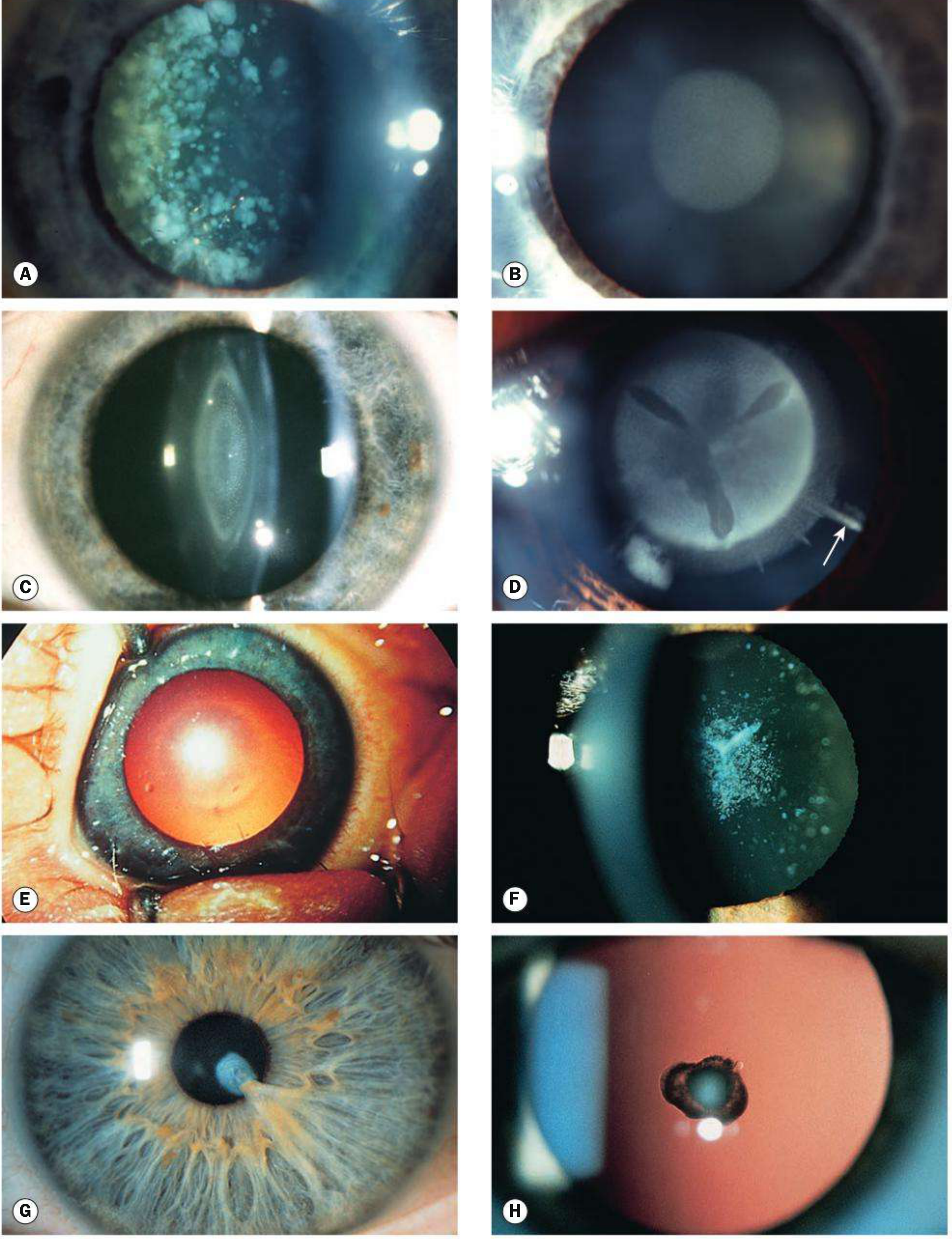
| Type | Features |
|---|---|
| Zonular/Lamellar (MC) | Alternating clear and white lamellae around nucleus; "onion skin" |
| Nuclear | Opacity within embryonic/fetal nucleus |
| Polar — Anterior | Small, near-static; may cause anisometropic amblyopia |
| Polar — Posterior | More variable/progressive; risk of dehiscence during surgery |
| Oil droplet | Pathognomonic of galactosaemia |
| Sutural | Follows Y-suture; seen in Nance–Horan female carriers |
| Coronary | Crown-like opacities at equator |
Key Systemic Associations
Metabolic
| Condition | Cataract Type | Notes |
|---|---|---|
| Galactosaemia (GALT deficiency, AR) | "Oil droplet" opacity | Reversible with dietary modification |
| Galactokinase deficiency | Cataract may be sole manifestation | — |
| Lowe syndrome (X-linked) | Universal cataract + microphakia | + Congenital glaucoma (50%), renal disease, mental retardation |
| Mannosidosis (AR) | Spoke-like posterior cortex opacities | + corneal clouding |
| Hypo/hyperglycaemia, hypoparathyroidism | Variable | — |
Intrauterine Infections (TORCH)
| Infection | Cataract Type | Key Features |
|---|---|---|
| Rubella (MC TORCH cause) | "Pearly white" nuclear cataract | + salt-and-pepper chorioretinitis, microphthalmos, deafness, CHD |
| Toxoplasmosis | Variable | + chorioretinitis, microphthalmos, optic atrophy |
| CMV | Variable | + chorioretinitis, intracranial calcification, hepatosplenomegaly |
| Varicella | Variable | + microphthalmos, cutaneous scarring |
Other
- PFV (Persistent Fetal Vasculature): Usually unilateral; fibrovascular plaque behind lens; elongated ciliary processes; risk of angle-closure glaucoma
- Lowe syndrome, Alport syndrome, chromosomal disorders, aniridia, craniofacial syndromes
Workup
- History: Maternal illness/drugs during pregnancy, family history, steroid use
- Visual assessment (Teller cards, following light in non-verbal children)
- Ocular exam: Size, location; cataracts ≥3 mm usually affect vision; check for glaucoma
- Cycloplegic refraction
- B-scan US: If fundus not visible; rule out posterior PFV in unilateral cases
- Labs: RBC galactokinase + GALT (galactosaemia); urine amino acids (Lowe syndrome); TORCH titres
Treatment
- Urgent surgery to prevent deprivation amblyopia:
- Bilateral dense cataracts: Surgery at 4–10 weeks of age
- If surgery is done before 4 weeks → higher risk of juvenile glaucoma
- Post-op amblyopia treatment is mandatory
- Dilating drops (phenylephrine 2.5% TID or cyclopentolate 1% BID) as temporizing measure for small cataracts
- Unilateral cataracts that don't obscure visual axis can still cause amblyopia — treat accordingly
Key High-Yield Points
- MC type: Zonular/lamellar
- MC cause overall: Autosomal dominant inheritance
- MC infective cause: Rubella → "pearly white" nuclear cataract
- MC metabolic cause: Galactosaemia → "oil droplet" opacity (reversible)
- MC inheritance pattern in familial: Autosomal dominant
- Bilateral cataract → search for genetic/metabolic cause; Unilateral → usually sporadic (also think PFV)
- Surgery timing: 4–10 weeks for dense bilateral cataract
Sources: Kanski's Clinical Ophthalmology 10th ed.; Wills Eye Manual
This is a shared conversation. Sign in to Orris to start your own chat.