Abg analysis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Now I have enough content for a thorough, well-structured ABG analysis guide. Let me compile everything.
Arterial Blood Gas (ABG) Analysis
Normal Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mm Hg |
| PaO2 | 70 - 95 mm Hg (age-dependent) |
| HCO3- | 22 - 26 mmol/L |
| Base Excess (BE) | -2 to +2 mEq/L |
| SaO2 | 95 - 100% |
- pH < 7.35 = acidemia; pH > 7.45 = alkalemia
- PaCO2 < 35 = hyperventilation; PaCO2 > 45 = hypoventilation/hypercapnia
Step-by-Step Interpretation
Step 1 - Determine the pH
- < 7.35 = Acidosis
- > 7.45 = Alkalosis
- 7.35-7.45 = Normal (but a disorder may still exist - check other values)
Step 2 - Identify the Primary Disorder
| Disorder | pH | PaCO2 | HCO3- |
|---|---|---|---|
| Respiratory acidosis | ↓ | ↑ | Normal/↑ |
| Respiratory alkalosis | ↑ | ↓ | Normal/↓ |
| Metabolic acidosis | ↓ | Normal/↓ | ↓ |
| Metabolic alkalosis | ↑ | Normal/↑ | ↑ |
Rule: The parameter that matches the pH change is the primary driver.
Step 3 - Assess Compensation
Compensation is never complete - it only partially corrects the pH.
| Primary Disorder | Compensatory Response | Formula |
|---|---|---|
| Metabolic acidosis | ↓ PCO2 (hyperventilation) | Expected PCO2 = 1.3 × ΔHCO3- below normal; or Winter's formula: PCO2 = (1.5 × HCO3-) + 8 ± 2 |
| Metabolic alkalosis | ↑ PCO2 (hypoventilation) | Expected ΔPCO2 = 0.6 × ΔHCO3- |
| Respiratory acidosis (acute) | ↑ HCO3- (buffering) | HCO3- ↑ 1 mmol/L per 10 mm Hg ↑ PCO2 |
| Respiratory acidosis (chronic) | ↑ HCO3- (renal) | HCO3- ↑ 4 mmol/L per 10 mm Hg ↑ PCO2 |
| Respiratory alkalosis (acute) | ↓ HCO3- | HCO3- ↓ 2 mmol/L per 10 mm Hg ↓ PCO2 |
| Respiratory alkalosis (chronic) | ↓ HCO3- (renal) | HCO3- ↓ 5 mmol/L per 10 mm Hg ↓ PCO2 |
Key: If measured compensation does NOT match predicted, a mixed disorder is present.
- Respiratory compensation for metabolic disorders: rapid (minutes-hours)
- Metabolic compensation for respiratory disorders: slow (3-5 days for full renal compensation)
Step 4 - Calculate the Anion Gap (if metabolic acidosis)
Anion Gap = Na+ - (Cl- + HCO3-)
- Normal AG: 8-12 mEq/L (some use 12 as upper limit)
- Correct for albumin: for every 1 g/dL drop in albumin below 4, add 2.5 mEq/L to measured AG
| High AG Metabolic Acidosis (MUDPILES) | Normal AG Metabolic Acidosis (HARDUP) |
|---|---|
| Methanol | Hyperalimentation / Hospital saline |
| Uremia | Acid infusion / Addison's disease / Carbonic anhydrase inhibitors |
| DKA (diabetic ketoacidosis) | Renal tubular acidosis |
| Paraldehyde / Propylene glycol | Diarrhea |
| Iron / Isoniazid | Ureteral diversion |
| Lactic acidosis | Pancreatic fistula |
| Ethylene glycol | |
| Salicylates |
Step 5 - Assess Oxygenation
A-a Gradient = FiO2 × (Patm - PH2O) - (PaO2 + PaCO2/0.8)
Simplified estimate of normal A-a gradient: (Age/4) + 4
| Mechanism of Hypoxemia | A-a Gradient |
|---|---|
| V/Q mismatch (e.g., pneumonia, PE) | Increased |
| Diffusion impairment (e.g., ILD) | Increased |
| R-to-L shunt | Increased |
| Hypoventilation | Normal |
| Altitude / low FiO2 | Normal |
| Hepatopulmonary syndrome | Increased |
Normal PaO2 by age (sitting): PaO2 = 104.2 - (0.27 × age in years)
Acid-Base Map
This diagram plots pH vs PCO2 with labeled zones for each primary and mixed disorder:
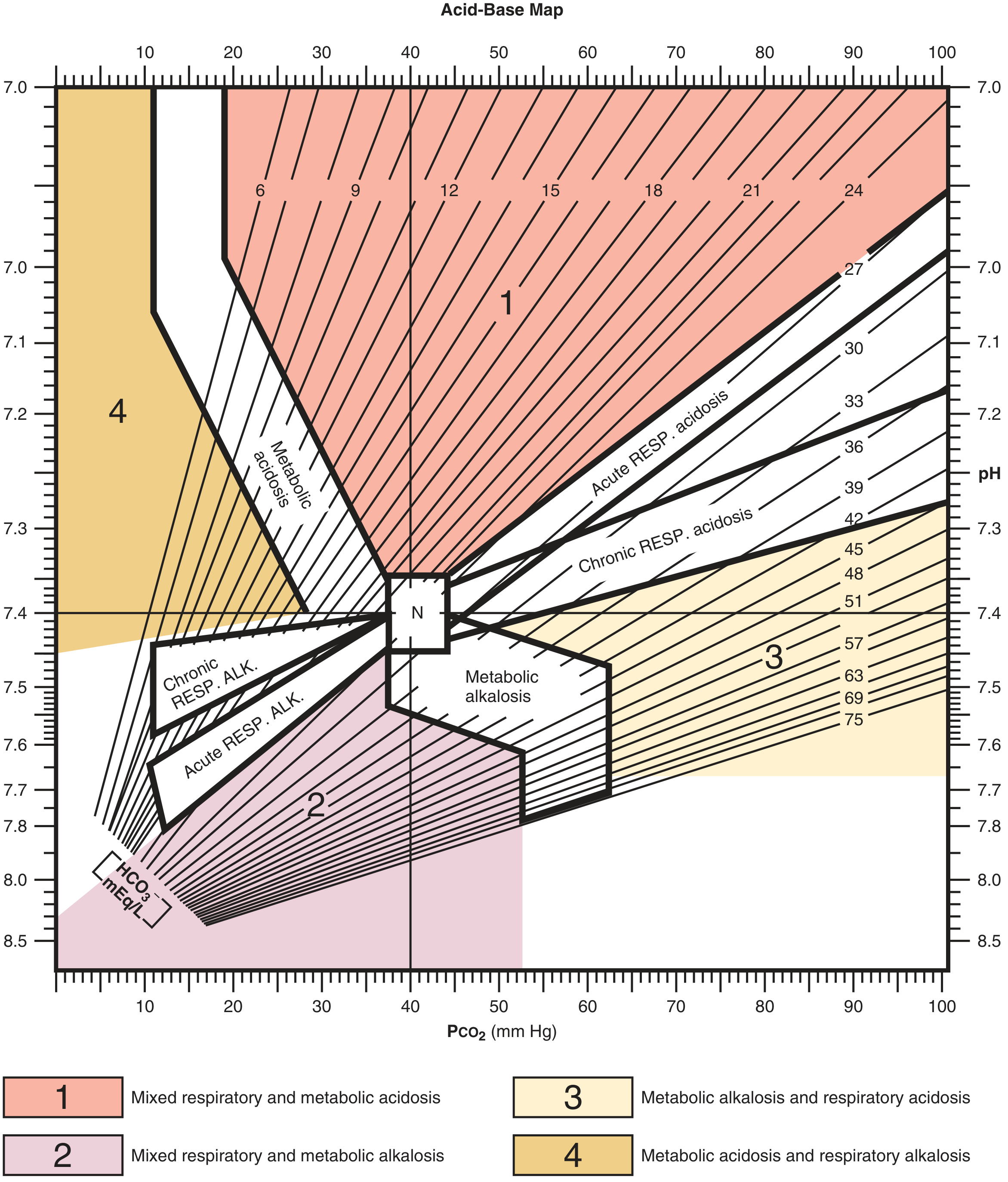
Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Zone 1 (upper right, red): Mixed respiratory + metabolic acidosis
- Zone 2 (lower left, pink): Mixed respiratory + metabolic alkalosis
- Zone 3 (lower right, yellow): Metabolic alkalosis + respiratory acidosis
- Zone 4 (upper left, orange): Metabolic acidosis + respiratory alkalosis
- N (center): Normal
Worked Examples
Example 1 - Metabolic acidosis with compensation:
A 58-year-old with 1 week of diarrhea: Na+ 133, K+ 2.8, pH 7.26, Cl- 118, PCO2 13, HCO3- 5
- pH < 7.40 → acidosis
- HCO3- is low, PCO2 is not elevated → primary metabolic acidosis
- Expected PCO2 = 40 - (1.3 × [25-5]) = 40 - 26 = 14 mm Hg; actual = 13 → appropriate compensation, no mixed disorder
Example 2 - Respiratory alkalosis (sepsis):
A 74-year-old with sepsis: pH 7.49, PCO2 25, HCO3- 22
- pH > 7.45 → alkalosis
- PCO2 low, HCO3- normal → primary respiratory alkalosis
- Cause: hyperventilation from sepsis/fever
Quick Reference: Henderson-Hasselbalch Equation
pH = 6.1 + log10([HCO3-] / 0.003 × PaCO2)
This is the backbone of ABG interpretation. Any change in HCO3- (metabolic) or PaCO2 (respiratory) drives a change in pH.
Venous Blood Gas (VBG) vs. ABG
- Venous pH averages ~0.03 lower than arterial
- PvCO2 averages 3-8 mm Hg higher than PaCO2
- VBG is unreliable in hypotensive patients and severe hypercapnia
- A normal PvCO2 can be used to exclude hypercapnia
Sources: Goldman-Cecil Medicine, Roberts & Hedges' Clinical Procedures in Emergency Medicine, Barash's Clinical Anesthesia, ROSEN's Emergency Medicine
Abg analysis from.basics.to.clinicals
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
This is a complete ABG guide covering everything from physiology to clinical application. Here's what's included:
Part 1 - Physiology: Why the body needs tight pH control, Henderson-Hasselbalch equation, the three buffer systems (chemical, respiratory, renal) and their speeds.
Part 2 - Normal Values: All parameters with clinical significance.
Part 3 - The 6-Step Approach:
- pH status
- Primary disorder identification
- Compensation assessment (with all formulas)
- Anion gap + albumin correction (MUDPILES / HARDUP)
- Urine anion gap for normal-AG acidosis
- Delta-delta ratio to unmask hidden mixed disorders
Part 4 - Four Primary Disorders in Depth: Each with pathophysiology, causes, clinical features, and management - including lactic acidosis Type A/B, metabolic alkalosis chloride-responsive vs. resistant, permissive hypercapnia in ARDS, and respiratory alkalosis as an early sepsis sign.
Part 5 - Osmolar Gap: Toxic alcohol ingestion, estimation formulas.
Part 6 - Oxygenation: A-a gradient and all six mechanisms of hypoxemia.
Part 7 - Mixed Disorders: Using the acid-base map and Δ/Δ ratio with classic clinical scenarios.
Part 8 - Four Worked Clinical Cases: DKA with hidden metabolic alkalosis, ethylene glycol ingestion, early sepsis, and acute-on-chronic COPD.
This is a shared conversation. Sign in to Orris to start your own chat.