Give me living anatomy of upper limb from bdc
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
I now have good textbook content. Let me compile the comprehensive living anatomy of upper limb as taught in BD Chaurasia style, supplementing with what I found in the library. Note that BD Chaurasia is not in the library, so I'll provide the BDC-style content from my own knowledge, organized exactly as BDC presents it, clearly noting the source.
Living Anatomy of the Upper Limb (BD Chaurasia style)
Note: BD Chaurasia's Human Anatomy (Vol. 1 - Upper Limb & Thorax) is not in the available textbook library. The structured content below is based on the BDC curriculum as taught in Indian medical colleges, supplemented with findings from Gray's Anatomy for Students in the library.
1. Bones and Bony Landmarks
Clavicle
- The entire clavicle is subcutaneous and palpable throughout its length from the sternoclavicular joint to the acromioclavicular joint.
- The medial (sternal) end is visible as a prominence above the manubrium.
- The lateral third has an inferior concavity; the medial two-thirds have a superior convexity.
- Clinical: Site of the most commonly fractured bone in the body (indirect fall on outstretched hand).
Scapula
- Spine of scapula: Palpable along its entire length, ending laterally as the acromion - the highest point of the shoulder.
- Acromion: Forms the "point" of the shoulder; the subdeltoid bursa and supraspinatus tendon lie deep to it.
- Coracoid process: Palpable 2.5 cm below the junction of the lateral and middle thirds of the clavicle, deep to the medial margin of the deltoid. Tenderness here = coracoid bursitis.
- Medial (vertebral) border: Palpable with the arm dependent; lies 5 cm from the midline opposite the 2nd-7th ribs.
- Inferior angle: At the level of the 7th rib/7th intercostal space; palpable when the arm is brought forward.
Humerus
- Greater tubercle: Most lateral point of the shoulder (not the acromion); visible as a rounded prominence distal to the acromion.
- Intertubercular (bicipital) groove: Between greater and lesser tubercles; the biceps long head tendon runs in it.
- Deltoid tuberosity: Mid-lateral shaft, palpable through deltoid.
- Medial epicondyle: Prominent medial projection at the elbow; the ulnar nerve can be rolled against it ("funny bone").
- Lateral epicondyle: Less prominent, lateral side of the elbow; common extensor origin is attached here (site of "tennis elbow").
- Capitulum and Trochlea: Palpable anteriorly with the elbow slightly flexed.
- Olecranon: The bony posterior point of the elbow (tip of ulna).
BDC Key Point - Elbow Triangle/Line:
- With the elbow extended: medial epicondyle, lateral epicondyle, and olecranon are in a straight horizontal line.
- With the elbow flexed to 90°: these three points form an equilateral triangle (Hueter's triangle).
- This relationship is disrupted in supracondylar fractures (triangle preserved) vs dislocation (triangle distorted).
Radius and Ulna
- Head of radius: Palpable in the posterolateral dimple below the lateral epicondyle; rotates during pronation-supination.
- Radial styloid process: Lateral side of wrist; extends 1 cm distal to the ulnar styloid.
- Ulnar styloid process: Medial side of wrist; small projection.
- Lister's tubercle (dorsal radial tubercle): On the dorsum of the radius; the extensor pollicis longus tendon hooks around it.
Hand
- Pisiform: Palpable at the medial side of the proximal wrist crease; the flexor carpi ulnaris inserts here. Ulnar nerve and artery pass lateral to it.
- Hook of hamate: 1 cm distal and lateral to pisiform; the ulnar nerve and artery pass just lateral.
- Tubercle of scaphoid: Palpable in the anatomical snuff box floor; the radial artery runs through the snuff box.
- Metacarpal heads: Form the knuckles; the 2nd metacarpal head is the most prominent.
2. Muscles and Tendons Visible/Palpable
Shoulder Region
- Deltoid: Forms the rounded contour of the shoulder; attached to the deltoid tuberosity. The axillary nerve (C5,6) enters its deep surface. Wasting of deltoid = axillary nerve palsy.
- Trapezius: Forms the sloping contour of the neck to the shoulder; tested by shrugging the shoulder against resistance (spinal accessory nerve).
- Pectoralis major: Anterior axillary fold; tested by pushing the hands against the hips (medial and lateral pectoral nerves).
- Latissimus dorsi: Posterior axillary fold; tested by coughing while palpating (thoracodorsal nerve).
Arm
- Biceps brachii: Prominent in the anterior arm; its long head tendon is palpable in the bicipital groove. Testing: flexion of elbow + supination. Tendon reflex = C5,6. Bicipital aponeurosis fans medially at the elbow.
- Triceps brachii: Posterior arm; tested by extension against resistance. Triceps jerk = C7. The radial nerve runs in the spiral groove of the humerus (posterior aspect).
- Coracobrachialis: Palpable in the axilla and medial arm.
Cubital Fossa (Anterior Elbow)
Contents from lateral to medial (mnemonic TAN or BAN):
| Structure | Position |
|---|---|
| Biceps Tendon | Most lateral palpable structure |
| Brachial Artery | Medial to biceps tendon - site for BP measurement and brachial pulse |
| Median Nerve | Most medial; not palpable but vulnerable |
- Cephalic, basilic, and median cubital vein are visible subcutaneously over the cubital fossa - used for venepuncture.
- Radial nerve is deep to the lateral margin of brachioradialis.
- Ulnar nerve lies behind the medial epicondyle.
Forearm
- Brachioradialis: Forms the lateral muscular mass of the forearm (the "fleshy part" lateral to the cubital fossa); tested by flexing the elbow in the mid-prone position.
- Flexor carpi radialis (FCR): Palpable and visible when wrist is flexed against resistance; runs obliquely to the base of the 2nd metacarpal. The radial artery (radial pulse) lies just lateral to it.
- Palmaris longus (PL): The most superficial midline tendon at the wrist; visible when making a fist + wrist flexion. Absent in ~14% of people (clinically important as a donor tendon for grafts).
- Flexor carpi ulnaris (FCU): Medial margin of the forearm; the tendon leads to the pisiform. The ulnar artery and nerve lie immediately lateral to it (Guyon's canal at the wrist).
- Extensor pollicis longus (EPL) and brevis (EPB) + Abductor pollicis longus (APL): Form the anatomical snuff box (see below).
Anatomical Snuff Box
Boundaries:
- Medial/ulnar border: EPL tendon
- Lateral/radial border: EPB + APL tendons
- Floor: Scaphoid and trapezium (scaphoid tenderness here after a fall = suspected scaphoid fracture)
- Contents: Radial artery (crosses the floor), cephalic vein (roof), superficial branch of radial nerve (roof)
3. Arteries and Pulses
| Pulse Site | Location | Normal Rate |
|---|---|---|
| Brachial artery | Medial to biceps tendon in cubital fossa; also in the medial arm | 60-100 bpm |
| Radial pulse | Lateral to FCR tendon at wrist (between FCR and radial styloid) | Most commonly used |
| Ulnar pulse | Lateral to FCU at wrist (less easily felt) | |
| Axillary artery | Palpable against humerus in the axilla | |
| Digital arteries | Compress at base of fingers |
- Allen's test: Compress both radial and ulnar arteries at the wrist. Release one - the hand should flush pink within 5-7 seconds if that artery is patent. Tests radial/ulnar dominance before arterial line placement.
4. Veins
- Cephalic vein: Begins in the anatomical snuff box → ascends on the lateral/radial side of the forearm → runs in the deltopectoral groove → drains into the axillary vein. Used for IV cannulation.
- Basilic vein: Begins on the medial/ulnar side of the dorsum of hand → ascends medially in the forearm → at the medial bicipital groove it pierces deep fascia → becomes the axillary vein. Used for PICC lines.
- Median cubital vein: Connects cephalic and basilic veins across the cubital fossa. Most common site for venepuncture (blood collection). The bicipital aponeurosis separates it from the brachial artery.
- Dorsal venous arch: On the dorsum of the hand; drains into cephalic (laterally) and basilic (medially).
5. Nerves - Surface Landmarks and Clinical Tests
Axillary Nerve (C5, C6)
- Winds around the surgical neck of humerus (fractured in shoulder dislocation or proximal humerus fracture).
- Test: Deltoid contraction (abduction 15°-90°) and sensation over regimental badge area (lateral arm over deltoid).
- Palsy: loss of shoulder abduction, flattening of deltoid contour.
Radial Nerve (C5-C8, T1)
- Winds in the spiral groove (posterior humerus) - damaged in mid-shaft humeral fractures.
- Test: Extension of wrist, fingers, and thumb (posterior interosseous nerve, deep branch).
- Palsy: Wrist drop - inability to extend the wrist; also sensory loss over dorsal first web space (superficial radial nerve).
Median Nerve (C6-C8, T1)
- Passes through the carpal tunnel at the wrist (between FCR and PL tendons, deep to flexor retinaculum).
- Tinel's sign: Tapping over the carpal tunnel at the wrist reproduces tingling in the thumb, index, middle, and lateral half of ring finger.
- Phalen's test: Wrist flexion for 60 seconds reproduces symptoms.
- Test: OK sign (flexion of thumb and index finger terminal phalanges = FPL + FDP-index).
- Palsy: Ape thumb deformity (thenar wasting), loss of opposition; sensory loss over lateral 3.5 fingers (palmar surface).
Ulnar Nerve (C7, C8, T1)
- Passes behind the medial epicondyle (palpable/vulnerable here), then through Guyon's canal (between pisiform and hook of hamate).
- Test: Abduction of fingers (dorsal interossei), adduction (palmar interossei), little finger abduction (abductor digiti minimi).
- Palsy: Claw hand (more pronounced in ring and little fingers - ulnar paradox), wasting of hypothenar eminence and interossei, Froment's sign (IP flexion when pinching paper = FPL compensating for weak adductor pollicis).
Musculocutaneous Nerve (C5, C6)
- Pierces the coracobrachialis and runs between biceps and brachialis.
- Becomes the lateral cutaneous nerve of the forearm below the elbow.
- Test: Elbow flexion with supination (biceps).
6. Reflexes
| Reflex | Tendon | Spinal Level |
|---|---|---|
| Biceps jerk | Biceps tendon in cubital fossa | C5, C6 |
| Supinator/Brachioradialis jerk | Brachioradialis tendon (just above radial styloid) | C5, C6 |
| Triceps jerk | Triceps tendon (just above olecranon) | C7 |
7. Lymph Nodes
- Axillary lymph nodes (5 groups): Palpable only when enlarged. The central group is felt highest in the axilla. Drains the entire upper limb, breast, and lateral thoracic wall.
- Cubital (supratrochlear) lymph node: 1-2 nodes just above the medial epicondyle; drain the medial forearm and hand. Enlarged in secondary syphilis.
- Deltopectoral (infraclavicular) nodes: Along the cephalic vein; drain the cephalic territory.
8. Key Clinical Correlations (BDC-style)
| Injury | Nerve/Structure | Deformity/Sign |
|---|---|---|
| Crutch palsy / Saturday night palsy | Radial nerve (spiral groove) | Wrist drop |
| Supracondylar fracture humerus | Anterior interosseous nerve / brachial artery | Volkmann's ischemic contracture |
| Medial epicondyle fracture | Ulnar nerve | Claw hand (ring + little) |
| Carpal tunnel syndrome | Median nerve | Ape thumb, Tinel's/Phalen's +ve |
| Shoulder dislocation | Axillary nerve | Loss of shoulder abduction + sensory badge area |
| Colles' fracture | Dinner fork deformity | Radial styloid displaced dorsally |
| Scaphoid fracture | Radial artery at snuff box | Avascular necrosis (proximal fragment) |
Source note: BD Chaurasia's Human Anatomy, Vol. 1 (Upper Limb & Thorax) is not in the available textbook library. The above content is based on the BDC curriculum standard for Indian MBBS. Textbook cross-reference: Gray's Anatomy for Students (library, block4, lines 3557-3760) covers the same topics and confirms the anatomical landmarks described above. - Gray's Anatomy for Students, pp. 941-955.
Give me living anatomy of lower limb from vishram Singh with pictures
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have excellent content and image URLs. Let me compile everything into a thorough, well-illustrated response.
Living Anatomy of the Lower Limb
Note: Vishram Singh's Textbook of Anatomy is not available in the textbook library. The content below follows the Vishram Singh curriculum structure as taught in Indian MBBS, with anatomical content sourced from Gray's Anatomy for Students (available in the library). Images are from the textbook library.
- Gray's Anatomy for Students, surface anatomy chapter (block3, pp. 770-778)
Overview
Living anatomy of the lower limb involves identifying bony landmarks, muscles, tendons, vessels, and nerves on the living body through inspection and palpation. It has direct clinical importance for:
- Locating pulses and vessels for catheterization/BP measurement
- Safe injection sites (avoiding the sciatic nerve)
- Testing reflexes and nerve function (L1-S3 levels)
- Diagnosing fractures, dislocations, and nerve injuries
1. Bony Landmarks
Hip Region
- Iliac crest: The curved superior border of the ilium, palpable from the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS). The PSIS lies at the level of the S2 vertebra and is marked by a skin dimple.
- ASIS: Palpable at the anterior end of the iliac crest; lateral attachment of the inguinal ligament; origin of sartorius.
- Greater trochanter: Palpable ~1 hand's width below the midpoint of the iliac crest on the lateral thigh. The tip of the greater trochanter lies at the same level as the center of the femoral head. Used to locate the sciatic nerve (see below).
- Ischial tuberosity: The "sitting bone," palpable just above the gluteal fold. Marked by the sciatic nerve passing midway between it and the greater trochanter.
- Pubic tubercle: Palpable at the medial end of the inguinal ligament; medial attachment of the inguinal ligament. The femoral canal (and femoral hernia) lies immediately lateral to it.
Knee Region
- Patella: The largest sesamoid bone, palpable and mobile when the knee is extended and relaxed.
- Tibial tuberosity: Bony bump on the anterior tibia below the knee; the patellar ligament attaches here. Site of Osgood-Schlatter disease in adolescents.
- Medial and lateral femoral condyles: Palpable on either side of the knee.
- Medial and lateral tibial condyles (plateaus): Just below the femoral condyles.
- Head of fibula: Prominent bony point on the posterolateral knee. The common fibular (peroneal) nerve winds around the neck of fibula just below it and can be felt as a cord.
- Adductor tubercle: On the medial femoral condyle; insertion of adductor magnus; palpable above the medial epicondyle.
Leg and Foot
- Anterior border (shin) of tibia: Subcutaneous and palpable throughout its length - fractured in "shin splints" / tibial stress fractures.
- Medial malleolus: Medial bony prominence at the ankle; the posterior tibial artery and nerve pass in the groove behind it (tarsal tunnel).
- Lateral malleolus (fibula): More distal than the medial malleolus by ~1 cm; the peroneal tendons pass behind it.
- Sustentaculum tali: A shelf on the medial calcaneus, palpable 1 cm below the medial malleolus; the flexor hallucis longus tendon grooves its undersurface.
- Calcaneal tuberosity (heel): The posterior prominence of the calcaneus; the Achilles tendon inserts here.
- Head of 1st metatarsal: Medial prominence on the sole/plantar surface; gout most commonly affects the 1st MTP joint here.
- 5th metatarsal base: Lateral foot; styloid process is palpable; avulsion fracture common with ankle inversion injuries.
2. Safe Intramuscular Injection Site (Gluteal Region)
The sciatic nerve must be avoided when giving IM injections in the buttock.
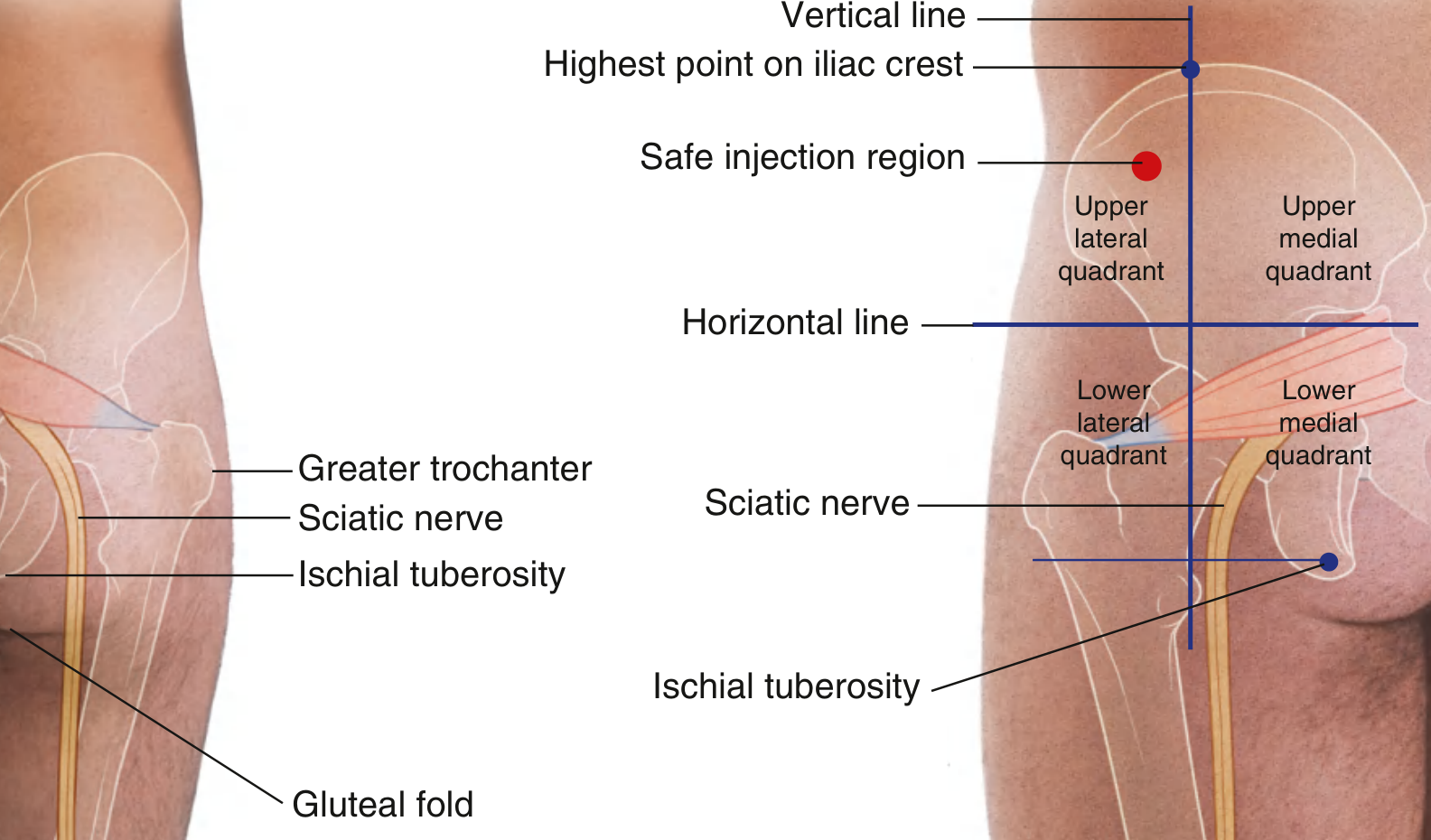
Fig. 6.131 - Avoiding the Sciatic Nerve. The sciatic nerve passes midway between the greater trochanter and ischial tuberosity. The gluteal region is divided into four quadrants by two lines. The safe injection site is the upper outer (superolateral) quadrant of the buttock.
Technique: Divide the buttock into 4 quadrants using:
- A vertical line from the highest point of the iliac crest
- A horizontal line midway between the iliac crest and ischial tuberosity
Inject in the upper lateral quadrant (anterior corner) - this avoids the sciatic nerve, superior and inferior gluteal vessels, and pudendal nerve.
3. Femoral Triangle and Femoral Artery
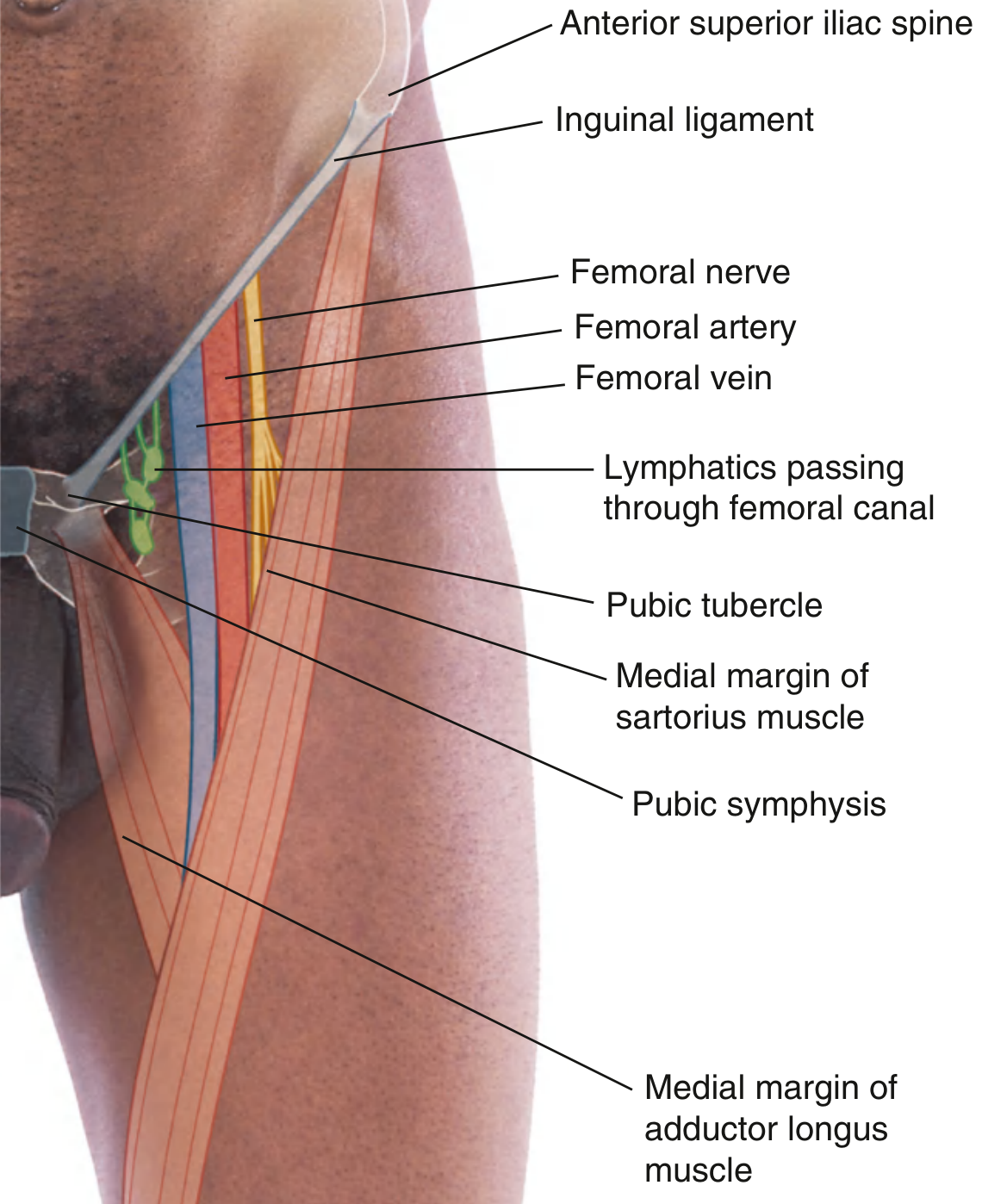
Fig. 6.132 - Position of the Femoral Artery in the Femoral Triangle.
Femoral triangle boundaries:
| Boundary | Structure |
|---|---|
| Superior (base) | Inguinal ligament |
| Medial | Medial border of adductor longus |
| Lateral | Medial border of sartorius |
| Floor | Iliopsoas (lateral) + pectineus (medial) |
| Roof | Fascia lata + cribriform fascia |
Contents (lateral to medial) - mnemonic NAVY:
- Nerve (femoral nerve) - most lateral
- Artery (femoral artery) - midpoint between ASIS and pubic symphysis
- Vein (femoral vein) - medial to artery
- Y - empty space = femoral canal (lymphatics + deep inguinal lymph node of Cloquet)
Femoral pulse: Felt just below the midpoint of the inguinal ligament (mid-inguinal point), halfway between the ASIS and the pubic symphysis.
- Femoral vein lies medial to the femoral artery - used for central venous cannulation.
- Femoral hernia passes through the femoral canal, immediately lateral to the pubic tubercle.
4. Muscles and Tendons
Anterior Thigh
- Quadriceps femoris (rectus femoris + 3 vasti): Bulk of the anterior thigh. The patellar reflex (L2,L3,L4) tests this group. Wasting is visible with femoral nerve palsy.
- Sartorius: Runs obliquely from ASIS to medial tibia (pes anserinus), forming the lateral wall of the femoral triangle and the roof of the adductor canal.
- Iliotibial (IT) band/tract: Visible and palpable on the lateral thigh as a flat vertical band; most prominent with knee extended. Forms a sharp anterior skin fold when extended. Tightness causes IT band syndrome (lateral knee pain in runners).
Medial Thigh (Adductors)
- Adductor longus: Its tendon is palpable as a cord below the pubic tubercle; forms the medial border of the femoral triangle.
- Gracilis: A flat straplike muscle on the medial thigh; part of pes anserinus; used as a tendon graft.
Posterior Thigh (Hamstrings)
- Biceps femoris: Forms the prominent lateral hamstring tendon, felt at the posterolateral knee; its tendon leads to the head of fibula.
- Semitendinosus: Prominent round medial hamstring cord; inserts with gracilis and sartorius at pes anserinus (medial tibial surface).
- Semimembranosus: Flat, lies deep to semitendinosus; the popliteal (Baker's) cyst lies between semimembranosus and medial gastrocnemius.
Leg
- Gastrocnemius + Soleus = Triceps surae: Forms the calf bulk; joins as the Achilles tendon (calcaneal tendon) - the strongest and thickest tendon in the body; inserts on the posterior calcaneus.
- Ankle jerk (S1, S2): Tap the Achilles tendon; absent in S1 radiculopathy, sciatic nerve palsy, peripheral neuropathy.
- Thompson's (Simmonds') test: Squeeze calf - if Achilles tendon is intact, the foot plantarflexes. No movement = rupture.
- Tibialis anterior: Palpable as a prominent tendon on the anteromedial ankle; tested by dorsiflexion and inversion.
- Extensor hallucis longus: Tendon visible on the dorsum of the foot medial to tibialis anterior; extends the great toe.
- Peroneus (fibularis) longus and brevis: Tendons palpable posterior to the lateral malleolus; evert the foot; tested in common fibular nerve assessment.
5. Peripheral Pulses of the Lower Limb
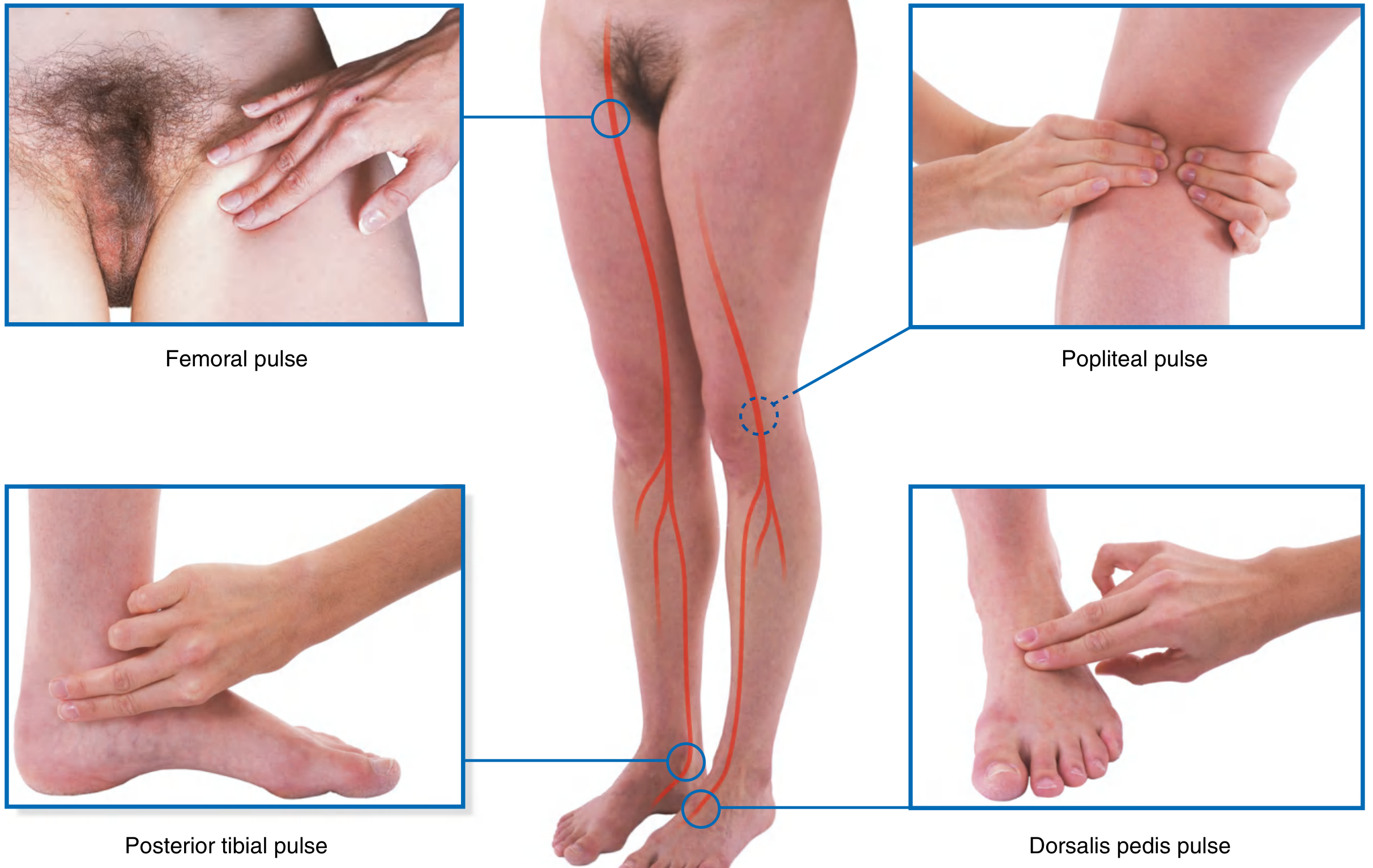
Fig. 6.140 - Where to Feel Peripheral Arterial Pulses in the Lower Limb.
| Pulse | Site | Clinical Use |
|---|---|---|
| Femoral | Mid-inguinal point (midway ASIS to pubic symphysis), below inguinal ligament | Peripheral vascular disease assessment, cardiac catheterization |
| Popliteal | Deep in the popliteal fossa, with knee slightly flexed; compress against popliteal surface of femur | Difficult to feel; absent = popliteal artery occlusion |
| Posterior tibial | Posteroinferior to medial malleolus, in groove between medial malleolus and calcaneum | Most reliable LL pulse for PVD |
| Dorsalis pedis | On the dorsum of the foot between extensor hallucis longus and extensor digitorum longus to 2nd toe, over the tarsal bones | Absent in ~8% of normal people (anatomical variant) |
Clinical pearl: In peripheral vascular disease (PAD), pulses are lost distal to the block. Absent dorsalis pedis but present posterior tibial = tibial artery disease below the knee.
6. Veins
-
Great (long) saphenous vein: The longest vein in the body. Begins at the medial end of the dorsal venous arch → passes anterior to the medial malleolus (reliably found here for surgical cutdown) → ascends the medial leg and thigh → pierces the cribriform fascia at the saphenous opening → drains into the femoral vein 3.5 cm below and lateral to the pubic tubercle (saphenofemoral junction = SFJ).
- The saphenofemoral junction is the site of saphena varix (variceal dilatation) and the saphenous nerve accompanies it in the leg.
- Used for coronary artery bypass grafting (CABG).
-
Small (short) saphenous vein: Begins posterior to the lateral malleolus → ascends the midline of the calf → pierces deep fascia in the popliteal fossa → drains into the popliteal vein (saphenopopliteal junction = SPJ).
-
Dorsal venous arch: On the dorsum of the foot; drains into great saphenous (medially) and small saphenous (laterally); used for IV cannulation.
7. Nerves - Surface Landmarks and Testing
Sciatic Nerve (L4, L5, S1, S2, S3)
- Leaves the pelvis through the greater sciatic foramen, below piriformis.
- Passes midway between the greater trochanter and ischial tuberosity.
- Divides at the upper angle of the popliteal fossa into tibial (medial) and common fibular (lateral) nerves.
- Lasègue's straight leg raise test: With the patient supine, raise the leg with knee extended. Pain radiating down the posterior thigh and leg at <60° = sciatic nerve root irritation (prolapsed intervertebral disc, most commonly L4/5 or L5/S1).
Common Fibular (Peroneal) Nerve (L4, L5, S1)
- Winds around the neck of fibula (just below fibular head) - can be rolled here.
- Most commonly injured nerve in the lower limb - susceptible to compression (tight plaster cast, crossing legs habitually).
- Palsy: Foot drop (loss of dorsiflexion and eversion) + sensory loss over lateral leg and dorsum of foot.
- Test: Dorsiflexion and eversion of foot.
Tibial Nerve (L4, L5, S1, S2, S3)
- Passes through the popliteal fossa (lateral to popliteal vessels), then through the tarsal tunnel behind the medial malleolus.
- Tarsal tunnel syndrome: Tibial nerve compression behind medial malleolus → burning/tingling in the sole (analogous to carpal tunnel in the hand).
- Test: Plantarflexion and toe flexion; ankle jerk (S1).
Femoral Nerve (L2, L3, L4)
- Lies lateral to the femoral artery in the femoral triangle.
- Test: Knee extension (quadriceps); patellar reflex (L2, L3, L4).
- Femoral nerve stretch test (reverse straight leg raise): Patient prone, flex knee - pain in anterior thigh = L2/3/4 root irritation (upper lumbar disc).
- Sensory: medial leg and foot via saphenous nerve.
Obturator Nerve (L2, L3, L4)
- Sensory: medial thigh (small patch).
- Test: Hip adduction.
8. Reflexes Summary
| Reflex | Method | Spinal Level |
|---|---|---|
| Knee (patellar) jerk | Tap patellar tendon (tibial tuberosity to patella) | L2, L3, L4 |
| Ankle jerk | Tap Achilles tendon with foot in slight dorsiflexion | S1, S2 |
| Plantar reflex | Stroke lateral sole from heel to ball of foot | L5, S1 |
| ↑ Babinski | Extension of hallux + fanning of toes | Upper motor neuron lesion |
9. Knee Joint - Living Anatomy and Clinical Tests
- Patellar ligament: From inferior pole of patella to tibial tuberosity; site of patellar reflex tap.
- Joint line: Palpable medially and laterally with knee at 90° flexion; tenderness here = meniscal tear.
- Medial collateral ligament (MCL): Palpable along medial joint line.
- Lateral collateral ligament (LCL): A cord-like structure between the lateral femoral epicondyle and fibular head; palpable with the leg crossed (figure-4 position).
- Anterior cruciate ligament (ACL): Intracapsular; not directly palpable. Tested by anterior drawer test and Lachman's test (anterior tibial translation on femur with knee at 30° flexion). Torn in knee valgus + rotation injuries (skier's knee, unhappy triad).
- McMurray's test: Rotation + extension of knee with pressure on joint line = click/pain = meniscal tear.
- Ballottement/fluctuation: Palpate fluid in the knee (suprapatellar pouch and joint cavity) - indicates effusion.
10. Ankle and Foot - Living Anatomy
- Medial malleolus: Palpate medial ankle; the posterior tibial artery pulse and tibial nerve pass behind it in the tarsal tunnel (posterior tibial tendon, flexor digitorum longus, vessels, tibial nerve, flexor hallucis longus - mnemonic Tom Dick And Very Nervous Harry).
- Lateral malleolus: Peroneus (fibularis) longus and brevis tendons pass behind it, held by superior and inferior peroneal retinacula.
- Anterior talofibular ligament (ATFL): Most commonly torn in ankle inversion sprains; runs from anterior fibula to talus neck.
- Achilles tendon: Palpable and visible along the posterior heel; gap on palpation = complete rupture. Thompson's test confirms.
- Plantar fascia: Origin on the medial calcaneal tuberosity; tenderness here = plantar fasciitis (heel pain).
Source: Content follows Vishram Singh's Textbook of Anatomy - Lower Limb, Abdomen & Pelvis curriculum. Vishram Singh is not in the available textbook library. Anatomical text and images sourced from Gray's Anatomy for Students in the library (block3, lines 6084-6294). - Gray's Anatomy for Students, Surface Anatomy chapter, pp. 770-778.
This is a shared conversation. Sign in to Orris to start your own chat.