Write a review on metabolic disease of bone. For MD pathology from ? From Robbins. I'm calling for India.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive MD Pathology-level review. Let me compile the full review from Robbins, Cotran & Kumar.
METABOLIC DISEASES OF BONE
A Review for MD Pathology
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease
Metabolic diseases of bone encompass a group of disorders in which bone quantity, quality, or mineralization is abnormal. The major entities are: Osteoporosis, Osteomalacia/Rickets, Hyperparathyroidism (and Renal Osteodystrophy), and Paget Disease of Bone.
1. OSTEOPENIA AND OSTEOPOROSIS
Definition
Osteopenia = decreased bone mass without fracture risk.
Osteoporosis = osteopenia severe enough to significantly increase the risk of fracture.
Radiographically:
- Osteoporosis: bone mass >2.5 SD below mean peak bone mass in young adults (T-score ≤ -2.5)
- Osteopenia: 1 to 2.5 SD below the mean (T-score -1.0 to -2.5)
Classification (Table 26.3)
| Type | Examples |
|---|---|
| Primary | Postmenopausal, Senile, Idiopathic |
| Secondary - Endocrine | Hyperparathyroidism, Hyperthyroidism, Addison disease, Type 1 DM, Hypothyroidism |
| Secondary - GI | Malabsorption, Hepatic insufficiency, Vitamin C deficiency |
| Secondary - Drugs | Corticosteroids, Heparin, Anticonvulsants |
| Secondary - Other | Immobilization, Multiple myeloma, Chronic renal failure |
Pathogenesis
Peak bone mass is achieved in young adulthood, influenced by genetic polymorphisms affecting bone metabolism, physical activity, muscle strength, diet, and hormonal state. After peak mass is attained, bone resorption slightly exceeds formation - average loss of 0.7% per year in both sexes.
Key factors:
-
Age-related changes (Senile Osteoporosis - "low-turnover" form): Osteoblasts show reduced proliferative and biosynthetic capacity and attenuated response to growth factors.
-
Reduced physical activity: Osteocytes act as mechanosensors - reduced mechanical loading decreases WNT signaling, which normally suppresses sclerostin (a WNT inhibitor). With less mechanical stimulation, sclerostin is up-regulated, decreasing WNT signaling and thereby reducing osteoblast activity.
-
Calcium and Vitamin D deficiency: Dietary calcium deficiency and reduced intestinal calcium absorption (partly due to decreased active vitamin D production with aging) stimulate PTH release, which increases bone resorption.
-
Reduced estrogen levels (Postmenopausal Osteoporosis - "high-turnover" form):
- Estrogen normally suppresses osteoclast activity by reducing RANKL production and increasing OPG (osteoprotegerin) by osteoblasts.
- Estrogen also inhibits cytokines (IL-1, TNF, IL-6, M-CSF) that promote osteoclast differentiation.
- Loss of estrogen after menopause increases osteoclast activity disproportionately, causing accelerated bone resorption.
-
Genetics: Polymorphisms in genes encoding the vitamin D receptor, type I collagen, IL-6, and other mediators influence peak bone mass.
Morphology
Microscopically: cortical bone is thinned, haversian canals are widened, and trabeculae are reduced in number and are thin and non-weight-bearing. Importantly, the bone that is present is normally mineralized - this distinguishes osteoporosis from osteomalacia.
Clinical Features
- Vertebral fractures (thoracic and lumbar): pain, loss of height, kyphoscoliosis, lumbar lordosis
- Femoral neck and pelvic fractures: immobilization, pulmonary embolism, pneumonia - responsible for >50,000 deaths/year (US data)
- Blood calcium, phosphorus, and alkaline phosphatase are usually normal
- Plain X-rays cannot reliably detect loss until 30-40% of bone mass is lost
- Best screening: Dual-energy X-ray Absorptiometry (DEXA) and quantitative CT
Treatment
- Exercise, calcium and vitamin D supplementation
- Bisphosphonates (anti-resorptive - first line)
- Denosumab (anti-RANKL antibody) - effective in postmenopausal osteoporosis
- Menopausal hormone therapy (estrogen) - limited use due to DVT/stroke risk
2. OSTEOMALACIA AND RICKETS
Definition
Both represent impaired mineralization of bone matrix (osteoid).
- Rickets - occurs in children; interferes with deposition of bone in growth plates
- Osteomalacia - adult counterpart; bone formed during remodeling is undermineralized, predisposing to fractures
Key distinction from osteoporosis: In osteomalacia, mineralization is defective but bone matrix is present; in osteoporosis, bone mass is decreased but mineralization is normal.
Pathogenesis
Most cases result from abnormal Vitamin D metabolism or Vitamin D deficiency:
- Vitamin D is required for intestinal calcium and phosphate absorption
- Deficiency leads to low serum calcium/phosphate, inadequate mineralization of osteoid
- Causes include: nutritional deficiency (most common in India), malabsorption, renal failure (inability to form active 1,25-(OH)₂-D₃), liver disease, anticonvulsants
In children, insufficient mineralization at the growth plate cartilage leads to:
- Disorganized, widened growth plates
- Softening of bones (craniotabes, rachitic rosary, Harrison sulcus, genu varum/valgum)
Clinical Features of Rickets
- Craniotabes - softening of skull
- Rachitic rosary - costochondral junction enlargement
- Harrison sulcus - indentation along the lower chest (diaphragm pull)
- Frontal bossing, delayed fontanelle closure
- Genu varum (bow legs) or genu valgum (knock knees)
- Tetany from hypocalcemia
3. HYPERPARATHYROIDISM
Definition
Excess PTH (parathyroid hormone) leads to increased osteoclast activity, bone resorption, and osteopenia.
Pathogenesis of Bone Changes
PTH acts via the following mechanisms:
- Osteoclast activation (indirectly via increased RANKL on osteoblasts) → bone resorption and calcium mobilization
- Increased calcium resorption by renal tubules
- Increased urinary phosphate excretion
- Increased synthesis of active Vitamin D (1,25-(OH)₂-D) by renal α-1 hydrolase → increased intestinal calcium absorption and bone calcium mobilization (via RANKL on osteoblasts)
Net result: elevated serum calcium. Normally this provides negative feedback. When PTH is autonomous or compensatory, unrestrained osteoclast activity damages the skeleton.
Types
Primary Hyperparathyroidism:
- Autonomous PTH secretion (usually from parathyroid adenoma)
- Elevated PTH is directly responsible for bone changes
Secondary Hyperparathyroidism:
- Chronic renal failure → low 1,25-(OH)₂-D → hypocalcemia → compensatory ↑PTH
- Combination of elevated PTH + inadequate 1,25-(OH)₂-D + hyperphosphatemia + metabolic acidosis = Renal Osteodystrophy
Morphology (Osteitis Fibrosa Cystica)
In advanced/untreated hyperparathyroidism:
- Increased osteoclastic resorption along all bone surfaces (endosteal, periosteal, intracortical)
- Peritrabecular fibrosis and marrow fibrosis
- Brown tumors (focal collections of osteoclasts, fibrous tissue, and hemosiderin-laden macrophages from repeated microhemorrhages - yellow-brown color due to hemosiderin)
- Cyst formation - as brown tumors degenerate
The combination of osteitis fibrosa cystica (cystic bone destruction), brown tumors, and skeletal pain was the classic presentation of hyperparathyroidism; with early diagnosis now routine in high-income countries, these manifestations are rare.
Renal Osteodystrophy
A constellation of bone abnormalities in chronic renal failure:
- Osteopenia (from secondary hyperparathyroidism)
- Osteomalacia (from deficiency of active vitamin D)
- Growth retardation in children
- Hyperphosphatemia contributes by binding calcium, worsening hypocalcemia
- Metabolic acidosis also promotes bone loss
4. PAGET DISEASE OF BONE (Osteitis Deformans)
Definition
A disorder of increased but disordered and structurally abnormal bone formation. The bone is increased in mass and density but architecturally disorganized and mechanically weak.
Epidemiology
- Usually presents in late adulthood (rare under 40 years)
- ~1% of the US population >40 years
- Common in UK, central Europe, Greece, Australia, USA
- Rare in native Scandinavians, Chinese, Japanese, Africans
- Decreasing incidence over the past 30 years in some countries
Pathogenesis
Cause remains uncertain; both genetic and environmental factors are implicated:
- ~60% of familial cases and 10% of sporadic cases: germline mutations in SQSTM1 gene (encodes sequestosome-1) → increased NF-κB activity → increased osteoclast activity
- Activating mutations in RANK and inactivating mutations in OPG cause some juvenile cases
- Possible viral trigger: chronic infection of osteoclast precursors by measles or other RNA viruses (paramyxovirus hypothesis) - not firmly established
Three Phases of Paget Disease
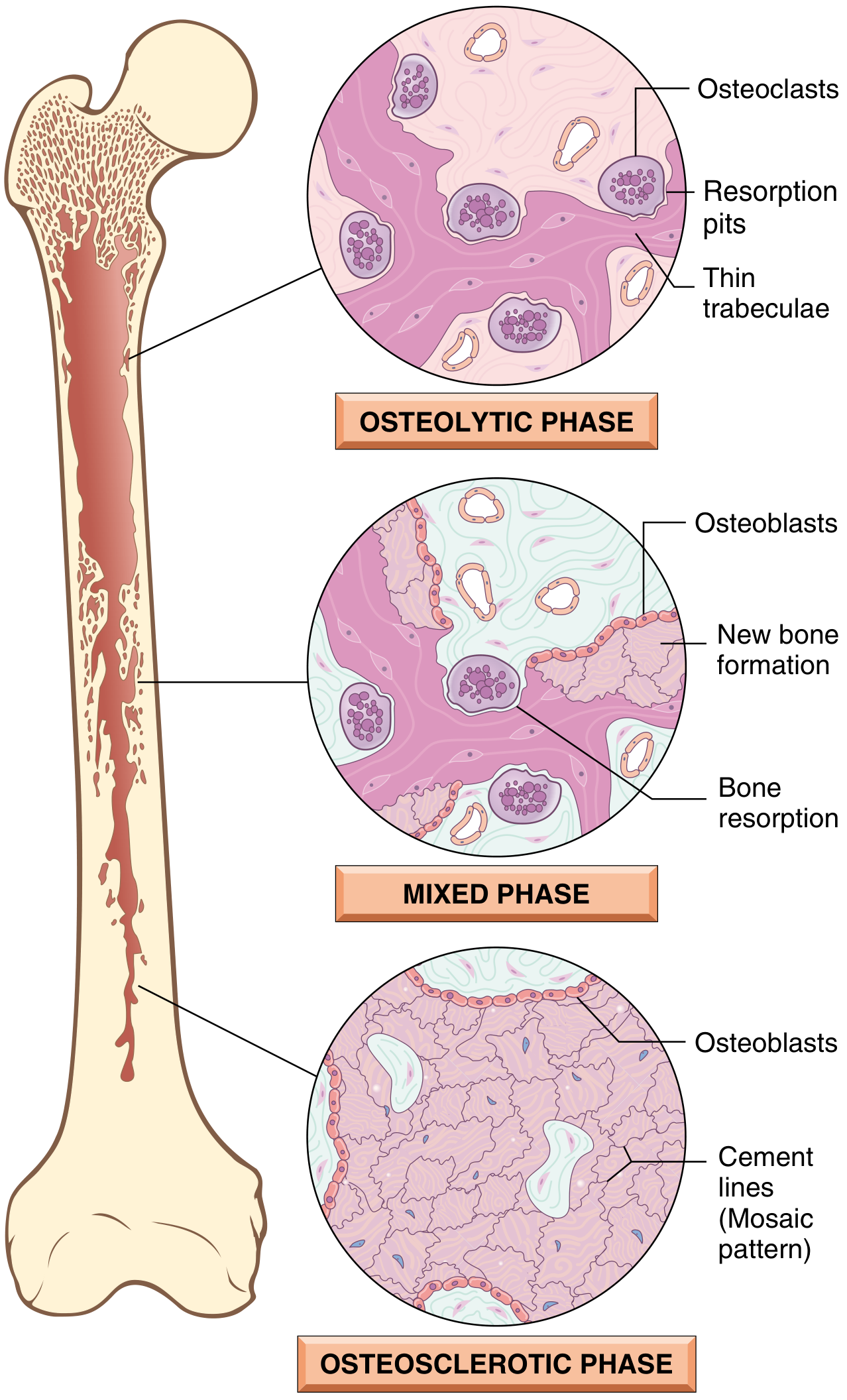
(Fig. 26.12, Robbins Cotran - Three phases of Paget disease)
| Phase | Predominant Activity | Histology |
|---|---|---|
| 1. Osteolytic (Hot) | Osteoclastic | Numerous abnormally large, multinucleated osteoclasts (up to 100 nuclei); resorption pits; thin trabeculae |
| 2. Mixed (Active) | Both osteoclastic + osteoblastic | Active resorption + new woven bone formation simultaneously |
| 3. Osteosclerotic (Burned-out) | Osteoblastic predominance (quiescent) | Thickened trabeculae of woven bone; classic mosaic pattern (irregular cement lines - "jigsaw puzzle" appearance); marrow replaced by fibrovascular tissue |
Morphology
Gross:
- Cortical thickening and trabecular coarsening
- Characteristic "picture frame" vertebra on X-ray
- Bowing of long bones (especially tibia - "sabre shin")
- Skull: thickened, cotton-wool appearance
- Bone is increased in size, hypervascular, and prone to fracture
Microscopy (pathognomonic feature):
- Mosaic pattern of lamellar bone - irregularly shaped pieces of bone separated by prominent cement lines, creating a jigsaw/mosaic appearance
- Abnormally large, multinucleated osteoclasts in active phase
Clinical Features
- Many patients are asymptomatic (incidental finding on imaging or elevated alkaline phosphatase)
- Bone pain (most common symptom)
- Bone deformity: bowing of femur/tibia, frontal bossing (skull)
- Pathologic fractures (chalk-stick fractures in long bones)
- Nerve compression: deafness (VIII nerve), spinal stenosis, cranial nerve palsies
- High-output cardiac failure - due to increased vascularity (AV shunting in bone)
- Elevated serum alkaline phosphatase (ALP) - hallmark biochemical finding
- Normal serum calcium and phosphate (in uncomplicated cases)
Complications
- Osteosarcoma (~1% of Paget cases - most serious complication; high-grade; poor prognosis). Fibrosarcoma and chondrosarcoma are less common.
- Giant cell tumor - develops in pagetic bone
- Pathologic fractures
- Hearing loss (auditory foramen involvement)
- High-output heart failure
Laboratory Findings in Paget Disease
| Parameter | Finding |
|---|---|
| Serum ALP | Markedly elevated |
| Serum calcium | Normal (may rise with immobilization) |
| Serum phosphate | Normal |
| Urinary hydroxyproline | Elevated (resorption marker) |
Treatment
- Bisphosphonates (reduce osteoclast activity) - first-line
- Calcitonin (alternative)
- NSAIDs for pain
SUMMARY TABLE: Metabolic Bone Diseases at a Glance
| Feature | Osteoporosis | Osteomalacia/Rickets | Hyperparathyroidism | Paget Disease |
|---|---|---|---|---|
| Bone mass | Decreased | Normal/increased osteoid | Decreased | Increased (but abnormal) |
| Mineralization | Normal | Defective | Decreased | Abnormal (mosaic) |
| Pathology | ↓ Osteoblast activity / ↑ Osteoclast activity | Vitamin D deficiency | ↑ PTH → ↑ Osteoclasts | Disordered remodeling (SQSTM1/NF-κB) |
| Serum Ca | Normal | Low (or low-normal) | High (primary) | Normal |
| Serum Phosphate | Normal | Low | Low | Normal |
| ALP | Normal | Elevated | Elevated | Markedly elevated |
| PTH | Normal | Elevated (secondary) | Elevated | Normal |
| Key histology | Thin trabeculae, normal mineralization | Excess osteoid (unmineralized matrix) | Brown tumors, osteitis fibrosa cystica | Mosaic (cement lines), giant osteoclasts |
| Key complication | Fracture (hip, vertebra) | Growth failure (rickets) | Osteitis fibrosa cystica | Osteosarcoma, high-output HF |
Reference: Robbins, Cotran & Kumar - Pathologic Basis of Disease, Ch. 26 (Bones, Joints, and Soft Tissue Tumors), pp. 1085-1091.
This is a shared conversation. Sign in to Orris to start your own chat.