teach me frontal lobe in detail for a 20 mark question in psychiatry, but teach in a simplified way that i can remeber,,neuroanatomy, parts, functions of each, disorder, tests, assessment,
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything I need. Let me compile a comprehensive, well-structured, exam-ready answer.
🧠 The Frontal Lobe - Complete Guide for 20 Mark Psychiatry Exam
1. NEUROANATOMY - The Big Picture
Location: Anterior to the central sulcus (Rolandic fissure), the largest lobe of the brain.
Boundary landmarks:
- Posterior: Central sulcus (separates frontal from parietal lobe)
- Inferior: Lateral sulcus (Sylvian fissure) - separates from temporal lobe
- Medial wall: Cingulate sulcus
The frontal lobe = ~1/3 of the entire cerebral cortex. Its massive size compared to other primates is what makes us distinctly human.
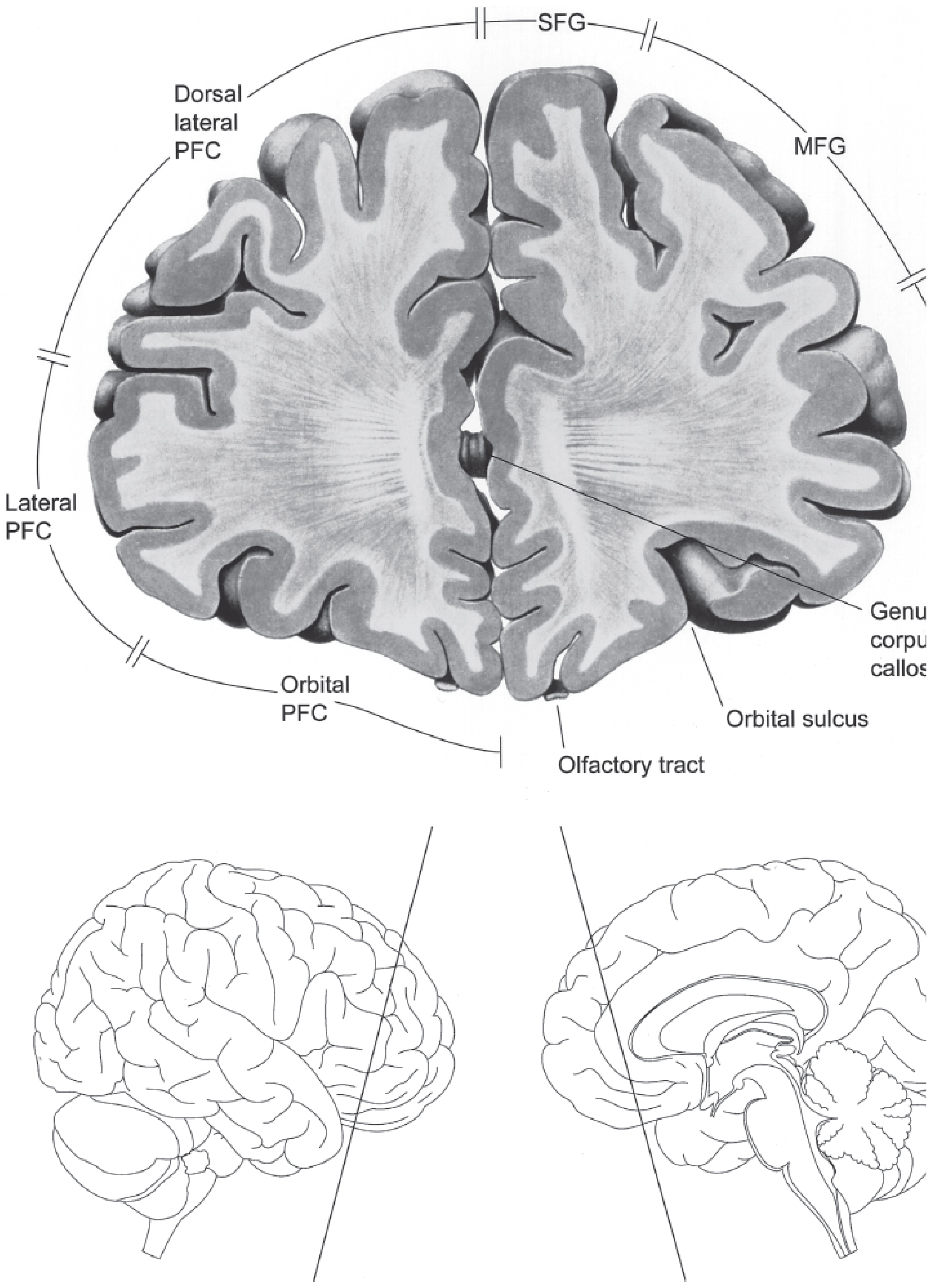
Gyri on the lateral surface (easy to remember: 3 gyri stacked):
- Superior Frontal Gyrus (SFG)
- Middle Frontal Gyrus (MFG) - contains the DLPFC
- Inferior Frontal Gyrus (IFG) - contains Broca's area (dominant hemisphere)
Brodmann areas you MUST know:
| Area | Name | Key Function |
|---|---|---|
| Area 4 | Primary Motor Cortex | Voluntary movement, contralateral body |
| Area 6 | Premotor + Supplementary Motor Area | Motor planning, sequences |
| Area 8 | Frontal Eye Fields (FEF) | Voluntary eye movements |
| Areas 9, 10, 11, 12 | Prefrontal Cortex | Executive function |
| Area 44, 45 | Broca's Area | Expressive speech (dominant) |
| Area 24, 32 | Anterior Cingulate Cortex | Motivation, conflict monitoring |
2. PARTS AND THEIR FUNCTIONS
Think of the frontal lobe as 4 functional regions:
A. Primary Motor Cortex (Area 4) - "The Commander"
- Executes voluntary movement - contralateral body
- Contains giant Betz cells (pyramidal neurons)
- Homunculus - motor map of the body (face and hand have disproportionately large representation)
- Damage: contralateral spastic hemiparesis (UMN pattern)
B. Premotor + Supplementary Motor Area (Area 6) - "The Planner"
- Premotor cortex: externally triggered movements, motor sequences
- SMA (Supplementary Motor Area): internally generated movement plans, bilateral coordination, motor memory sequences
- Damage to SMA: transient mutism, contralateral motor neglect, impaired bimanual coordination
- SMA damage = "alien hand syndrome" (hand acts on its own)
C. Prefrontal Cortex (PFC) - "The CEO of the Brain"
This is THE most important region for psychiatry. Divided into 3 subregions:
i. Dorsolateral PFC (DLPFC) - Areas 9, 10, 46
- Working memory (holding information while doing a task)
- Executive functions: planning, problem solving, cognitive flexibility
- Left DLPFC: verbal working memory; Right DLPFC: nonverbal/spatial working memory
- Shifting cognitive set (mental flexibility)
- Speed of information processing
- Damage: Apathy, abulia, loss of initiative, perseveration, poor working memory
- Psychiatric links: Hypoactivation in schizophrenia (dorsolateral hypofrontality), depression, ADHD
ii. Orbitofrontal Cortex (OFC) - Areas 11, 12, 13
- Impulse control, social behaviour, decision-making
- Integrates emotional signals (from amygdala) into decision-making
- Important for reward processing and emotional weighting of choices
- Has dense connections with amygdala, thalamus (dorsomedial nucleus)
- Damage: Disinhibition, impulsivity, poor judgment, inappropriate sexual behaviour, loss of empathy
- Famous case: Phineas Gage - an iron rod destroyed both frontal lobes in 1848. He survived physically but became "fitful, irreverent, profane, impatient" - his friends said "he was no longer Gage." This is the prototype of frontal lobe syndrome.
- Psychiatric links: OCD (hyperactivity), bvFTD, psychopathy, ASPD
iii. Medial PFC / Anterior Cingulate Cortex (ACC) - Areas 24, 25, 32
- Motivation, drive, initiation of action
- Error monitoring and conflict detection
- Emotional regulation
- Damage: Profound apathy, akinetic mutism, emotional blunting
- Psychiatric links: Depression (subgenual ACC - Area 25 is the DBS target in treatment-resistant depression), schizophrenia
D. Frontal Eye Fields (Area 8) - "The Gaze Controller"
- Voluntary saccades (fast eye movements) to the CONTRALATERAL side
- Damage (destructive lesion): Eyes deviate TOWARD the lesion (ipsilateral), away from the hemiplegia
- Irritative lesion (seizure): Eyes deviate AWAY from the lesion (contraversive)
E. Broca's Area (Areas 44, 45) - "The Speaker"
- Dominant hemisphere (left in ~95% right-handed people)
- Motor programming of speech
- Damage: Broca's (expressive/non-fluent) aphasia - understands but cannot speak fluently; telegraphic speech; often frustrated
3. MNEMONIC FOR FRONTAL LOBE FUNCTIONS
"RIO" (from Neuroanatomy through Clinical Cases):
- R - Restraint (inhibiting inappropriate behaviors - OFC)
- I - Initiative (motivation to act - medial PFC/ACC)
- O - Order (sequencing, planning, working memory - DLPFC)
4. FRONTAL LOBE SYNDROMES (Psychiatric Disorders)
Classic Triad of Frontal Lobe Syndromes
| Syndrome | Region Damaged | Key Features |
|---|---|---|
| Dysexecutive Syndrome | DLPFC | Poor planning, perseveration, poor working memory, impaired set-shifting |
| Disinhibition Syndrome | OFC | Impulsivity, inappropriate behavior, poor judgment, hypersexuality, witzelsucht |
| Apathetic/Abulic Syndrome | Medial PFC / ACC | Profound apathy, loss of drive, akinesia, mutism (severe), emotional blunting |
Specific Psychiatric Disorders with Frontal Involvement
Schizophrenia:
- DLPFC hypoactivation ("hypofrontality") - seen on PET/fMRI
- Explains negative symptoms (flat affect, avolition, alogia)
- OFC/ACC dysfunction links to disorganization
Depression:
- Subgenual ACC (Area 25) hyperactivity
- DBS (Deep Brain Stimulation) targeting Area 25 for treatment-resistant depression (TRD)
- Left prefrontal hypoactivity on neuroimaging
ADHD:
- Frontal lobe and caudate volume smaller than controls
- Cortical thickness matures later (~3 years delay) in DLPFC
- Frontal-striatal loop dysfunction - explains inattention and impulsivity
OCD:
- Orbitofrontal-striatal circuit hyperactivity (OFC → caudate → thalamus → OFC loop)
- PET shows increased OFC glucose metabolism
- Explains intrusive thoughts and compulsive behaviors
Frontotemporal Dementia (bvFTD):
- Degeneration of prefrontal and anterior temporal cortex
- Disinhibition, loss of empathy, apathy, perseveration
- Orbitofrontal/ventromedial damage = disinhibition
- DLPFC damage = executive failure
Antisocial Personality Disorder:
- Reduced prefrontal grey matter volume
- OFC and ACC dysfunction - reduced fear conditioning and empathy
Other associations:
- Left frontal lesion - Depression-like features
- Right frontal lesion - Mania-like features (disinhibition, euphoria)
- Bilateral frontal lesions - Full frontal syndrome, akinetic mutism, pseudobulbar palsy if motor areas involved
5. CLINICAL SIGNS TO LOOK FOR
Frontal Release Signs (Primitive Reflexes)
These are reflexes suppressed by the developing frontal lobe; they re-emerge when the frontal lobe is damaged:
| Sign | How to Elicit | Normal age to disappear |
|---|---|---|
| Grasp reflex | Stroke patient's palm | ~6 months |
| Suck reflex | Stroke the lips | ~1 year |
| Snout reflex | Tap the philtrum | Childhood |
| Rooting reflex | Touch corner of mouth | ~4 months |
| Glabellar tap | Tap between eyebrows | Should stop after 3-4 taps |
| Palmomental | Scratch thenar eminence → chin contracts | Childhood |
Behavioral Signs
- Abulia - passive, apathetic, speaks softly, delayed responses
- Witzelsucht - silly inappropriate jocularity, "making crass jokes"
- Confabulation - fabricates answers without intent to deceive
- Utilization behavior - grabs and uses objects in front of them reflexively (e.g., puts on someone else's glasses)
- Environmental dependency - driven entirely by environmental stimuli
- Perseveration - keeps repeating the same response even when asked to move on
- Gegenhalten (paratonia) - involuntary resistance to passive limb movement that matches the force applied
- Motor impersistence - cannot sustain a position (e.g., cannot hold tongue out for 20 seconds)
- Frontal magnetic gait - small shuffling steps, feet appear "glued" to floor (normal arm swing, flexed posture)
6. ASSESSMENT & TESTS FOR FRONTAL LOBE
Bedside Tests (Quick, Clinical)
| Test | What It Tests | What to Do | Frontal Sign |
|---|---|---|---|
| Digit Span | Attention/working memory | Repeat sequence forward & backward | <7 forward / <5 backward = abnormal |
| Months Backward | Working memory | Recite months in reverse | Should take <15 seconds |
| Go-No-Go Task | Response inhibition | 1 tap = raise finger; 2 taps = keep still | Cannot suppress the response to 2 taps |
| Luria Sequencing Task | Perseveration/set-shifting | Copy alternating pattern (wave/triangle) and continue | Perseveration/closing-in phenomenon |
| Luria Manual Sequencing | Motor sequencing | Fist-palm-side alternating on thigh | Cannot alternate sequence smoothly |
| FAS Word Fluency Test | Verbal fluency (dominant frontal) | Name words starting with F, A, S in 60 sec each | <12 words per letter = abnormal |
| Animal Naming | Fluency/semantic | Name animals in 60 seconds | <15 animals = impaired |
| Verbal Trails B (A-1-B-2...) | Set shifting | Alternate letters/numbers | Cannot shift between sets |
| Proverb Interpretation | Abstract reasoning | "What does 'rolling stone...' mean?" | Concrete interpretation = frontal |
| Similarities | Abstract reasoning | "Apple and orange - what are they?" | Concrete answers = frontal |
| Fire-in-theater question | Judgment | "What would you do if you saw fire in a theater?" | Note: NOT very reliable - patients may answer correctly but act foolishly in real life |
Formal Neuropsychological Tests
| Test | What It Measures |
|---|---|
| Wisconsin Card Sorting Test (WCST) | Cognitive flexibility, set-shifting (DLPFC). Patient sorts cards by rules that change - frontal patients cannot adapt. |
| Stroop Test | Response inhibition. Color-word interference - say the ink color, not the word. Frontal patients cannot suppress reading the word. |
| Trail Making Test Part B (TMT-B) | Set-shifting, divided attention. Alternate between numbers and letters (1-A-2-B-3-C...) |
| Verbal Fluency / FAS | Dominant frontal word generation |
| Figural Fluency (Five-Point Test) | Non-dominant frontal figure generation |
| Gambling Task (Iowa Gambling Task) | OFC function, decision-making under uncertainty |
| Tower of London / Tower of Hanoi | Planning, problem solving |
| Halstead Category Test | Abstraction and concept formation |
| Porteus Maze Test / Reitan Trail Making | Planning, regulation, checking |
| Benton's Verbal Fluency Test | Verbal skill and verbal regulation |
Physical Examination
- Check olfaction (anosmia - OFC tumor, trauma, degenerative dementia)
- Frontal release signs (grasp, suck, snout, rooting, palmomental)
- Gegenhalten (paratonia)
- Motor impersistence (hold arms up / tongue out for 20 seconds)
- Gait - frontal magnetic gait
- Optokinetic nystagmus - impaired saccades away from side of lesion
- Hemiparesis / UMN signs if motor cortex involved
Imaging for Frontal Lobe Assessment
- MRI brain - structural (for atrophy, tumors, strokes, trauma)
- PET/SPECT - metabolic hypofrontality (schizophrenia, depression, FTD)
- fMRI - working memory tasks, DLPFC activation studies
- EEG - for frontal lobe epilepsy (nocturnal, multiple brief episodes, can mimic psychiatric episodes)
7. CAUSES OF FRONTAL LOBE SYNDROME
Mnemonic: "TIMMS-P"
- T - Trauma (most common - orbitofrontal and anterior temporal often affected)
- I - Infarct (ACA territory - medial frontal; MCA - lateral frontal)
- M - Mass (tumor - meningioma, glioma)
- M - Multiple sclerosis
- S - Schizophrenia / psychosurgery (lobotomy - historical)
- P - Pick's disease / FTD
8. QUICK-RECALL CHEAT SHEET
| Region | Function | Damage → |
|---|---|---|
| Primary Motor (Area 4) | Voluntary movement | Contralateral hemiparesis (UMN) |
| SMA (Area 6 medial) | Bilateral motor coordination | Mutism, motor neglect, alien hand |
| Frontal Eye Fields (Area 8) | Saccades contralateral | Ipsilateral gaze deviation (eyes look at lesion) |
| Broca's (44/45) | Expressive speech | Non-fluent aphasia |
| DLPFC (9/46) | Working memory, executive | Apathy, perseveration, poor planning |
| OFC (11/12) | Impulse control, social judgment | Disinhibition, impulsivity, witzelsucht |
| Medial PFC / ACC (24/32) | Motivation, initiation | Apathy, akinetic mutism, depression |
9. THE PHINEAS GAGE PRINCIPLE (For Writing in Exam)
"Damage to both frontal lobes produces the frontal lobe syndrome: slow thinking, poor judgment, decreased curiosity, social withdrawal, apathy that can explode into impulsive disinhibition. Intelligence (IQ) may be preserved because IQ depends more on parietal lobe activation. Frontal lobe pathology becomes apparent only in unstructured, real-life situations - not in the structured examination room." - Kaplan & Sadock's Synopsis of Psychiatry
This is why testing judgment with simple questions (fire in theater) is not reliable - the physician must often diagnose frontal lobe disease from history alone.
10. EXAM ANSWER STRUCTURE (20 Marks)
Write your answer in this order:
- Introduction - Definition, location, size, evolutionary significance (2 marks)
- Anatomy - Gyri, Brodmann areas, 4 subdivisions (3 marks)
- Functions of each part - Use the DLPFC/OFC/Medial PFC/Motor divisions (4 marks)
- Frontal Lobe Syndromes - Dysexecutive/Disinhibition/Apathetic triad + specific disorders (4 marks)
- Clinical signs - Frontal release signs, behavioral signs, gait (3 marks)
- Tests and Assessment - Bedside + formal tests + imaging (4 marks)
Sources: Harrison's Principles of Internal Medicine 22E; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Kaplan & Sadock's Synopsis of Psychiatry; Neuroanatomy through Clinical Cases 3rd Ed; Adams and Victor's Principles of Neurology 12th Ed.
integrate information from the ppt with your information...give a simplfied text that ican remember...easily..include information from both ppt and your text and integrate frontal lobe in detail
Reading File
Running Command
Running Command
Running Command
I have the full PPT content. Now let me integrate everything into a comprehensive, simplified, memorable guide.
🧠 THE FRONTAL LOBE - Complete Integrated Study Guide
(PPT + Textbooks Combined | Simplified for 20-Mark Exam)
Source: Brain & Behaviour (David Clark, Nash Boutons, Mario Mendez, 3rd Ed) + Kaplan & Sadock + Harrison's + Adams & Victor + Neuroanatomy through Clinical Cases
PART 1: ORIENTATION - WHERE IS IT?
Think of the frontal lobe as the "FRONT OFFICE" of the brain - it's the boss.
- Largest lobe of the brain (~1/3 of total cortex)
- Anterior to the central sulcus (separates from parietal lobe)
- Above the lateral sulcus / Sylvian fissure (separates from temporal lobe)
- Most anterior tip = frontal pole
- Also called the "Social Lobe" or "Newest Lobe" (evolutionarily most recent)
Gyri - easy to remember (4 gyri total):
| Gyrus | Where | Key Content |
|---|---|---|
| Precentral Gyrus | Directly anterior to central sulcus | Primary Motor Cortex (Area 4) |
| Superior Frontal Gyrus (SFG) | Top horizontal strip | Higher cognition |
| Middle Frontal Gyrus (MFG) | Middle horizontal strip | DLPFC lives here |
| Inferior Frontal Gyrus (IFG) | Bottom strip, 3 parts: orbital, triangular, opercular | Broca's Area (44 & 45) |
PART 2: THE 6 FUNCTIONAL AREAS + THEIR FUNCTIONS + LESIONS + TESTS
Quick Map - Brodmann Numbers to Memorize:
Area 4 = Primary Motor
Area 6 = Premotor + SMA
Area 8 = Frontal Eye Fields
Area 9,10,46 = DLPFC
Area 10,11 = Orbitofrontal Cortex
Area 44,45 = Broca's Area
Area 24,25,32 = Anterior Cingulate (medial PFC)
🔴 1. PRIMARY MOTOR CORTEX (Area 4) - "The Muscle Commander"
Location: Precentral gyrus
Contains: Giant Betz cells (largest neurons in the body)
Inputs: Thalamus, basal ganglia, premotor cortex, sensory cortex
Output: Motor fibres → brainstem + spinal cord
Functions:
- Contraction of muscles on the OPPOSITE half of the body
- Bilateral control of: upper face, tongue, mandible, larynx, pharynx, axial muscles
- Each body part mapped on motor homunculus (face and hands get huge representation)
If damaged:
- Contralateral hemiparesis (UMN type - increased tone, increased reflexes, Babinski +ve)
- Increased/decreased tone, decreased power, decreased fine motor on opposite side
Bedside Tests:
- Motor Strength of Hand Grip - both hands, should be equal (dominant side slightly stronger). If examiner can easily free fingers = weak
- Finger Tapping (Motor Speed) - tap as fast as possible; does not differentiate from premotor cortex
🟠 2. PREMOTOR CORTEX (Area 6) - "The Motor Programme Store"
Location: Anterior to primary motor cortex, lateral surface
Inputs: Thalamus, basal ganglia, sensory cortex, SMA
Output: → Primary Motor Cortex
Functions:
- Stores motor programmes (learned motor skills)
- Controls coarse postural movements
- Externally triggered sequences
If damaged:
- Weakness in proximal muscles on contralateral side
- Apraxia (cannot perform learned skilled movements despite intact strength)
Bedside Tests:
- Finger-to-thumb succession test - touch each finger to thumb in rapid succession; watch speed and dexterity
- Apraxia tests - "blow a kiss" / "demonstrate use of a shovel"
🟡 3. SUPPLEMENTARY MOTOR AREA - SMA (Medial Area 6) - "The Internal Choreographer"
Location: Medial surface of frontal lobe, Area 6
Inputs: Cingulate gyrus, thalamus, sensory cortex, prefrontal cortex
Output: → Premotor cortex and primary motor cortex
Functions:
- Intentional perception of movement
- Procedural memory (how to do things - riding a bike)
- Internally generated (self-initiated) movements
- Bilateral motor coordination
If damaged:
- Mutism (cannot speak)
- Akinesia (cannot initiate movement)
- Alien hand syndrome
- Contralateral motor neglect
🟢 4. FRONTAL EYE FIELDS (Area 8) - "The Gaze Controller"
Location: Posterior middle frontal gyrus
Inputs: Parietal and temporal cortex
Output: → Caudate nucleus, superior colliculus, PPRF (Paramedian Pontine Reticular Formation)
Functions:
- Voluntary saccadic eye movements to the CONTRALATERAL side
- "Stimulation = eyes look AWAY from the side being stimulated"
If damaged:
- Destructive lesion → eyes deviate TOWARD the lesion (ipsilateral) = AWAY from hemiplegia
- Irritative/seizure → eyes deviate AWAY from lesion (contraversive) = TOWARD hemiplegia
- Easy memory trick: "Destruction = looking at your damage; Irritation = looking away from your damage"
Bedside Tests:
- Ask patient to follow a finger left to right, up and down (smooth pursuit)
- Ask patient to look left and right WITHOUT a finger to follow (tests voluntary saccades)
- Note: any inability to move or jerky movement
🔵 5. PREFRONTAL CORTEX (PFC) - "The CEO" - MOST IMPORTANT FOR PSYCHIATRY
This is the biggest area and the most relevant for your exam. It has 3 subregions:
A. DORSOLATERAL PFC / DLPFC (Areas 9, 10, 46)
Functions - "Executive Functions":
- Integration of sensory information
- Generation of range of responses to challenges
- Selection of most appropriate response
- Working memory (holding info while doing a task)
- Maintenance of task set
- Sequential ordering of data
- Self-evaluation of performance
- Shifting cognitive set (mental flexibility)
- "Formal thought disorder arises from a LACK of executive planning and editing" - PPT
If damaged:
- Poor planning, impaired working memory
- Cannot shift between tasks (perseveration)
- Disoriented thinking, difficulty coping with changing environments
Bedside Tests (from PPT - this is exam gold):
- "Is the patient able to make an appointment and arrive on time?"
- "Is the patient able to give a coherent account of their problems?"
- Digit span - 7 forward, 5 backward (normal); <7 forward = abnormal
- COWAT (Controlled Oral Word Association Test = FAS Test) - words starting with F, A, S in 1 minute each; >10 items normal, <8 = significant deficit. No proper nouns, no suffixed repeats.
- Category fluency - name animals / fruits / vegetables; >10 normal
- Alternating Hand Sequences / Luria Test - one hand palm up, other palm down; reverse as rapidly as possible. Frontal patients perform poorly.
- Wisconsin Card Sorting Test (WCST) - sort cards by colour/form/number; rules change silently. Frontal lobe damage = cannot adapt. Also abnormal in caudate damage and schizophrenia.
- Trail Making Test - connect dots (Part B = alternating numbers and letters). Tests: mental flexibility, executive functioning, speed of processing.
B. ORBITOFRONTAL CORTEX / OFC (Areas 10, 11)
Functions:
- Empathic, civil and socially appropriate behaviour
- Impulse control
- Decision-making (integrates emotional signals from amygdala)
- Reward processing
- Most of the personality change in frontal lobe injury is due to OFC damage
If damaged:
- Irritable and labile mood
- Disinhibition - inappropriate sexual behaviour, poor social judgment
- Witzelsucht - insensitive, crass humor that the patient finds funny but nobody else does
- Failure to respond to conventions of acceptable social behaviour
- No empathy, no concern for feelings of others
Increased OFC activity seen in:
- OCD (OFC + caudate hypermetabolism)
- Huntington's disease
- Globus pallidus lesions
Bedside Tests (from PPT):
- "Does the patient dress or behave in a way suggesting lack of concern for others?"
- Sense of Smell - test with coffee, cloves, etc. (anosmia = OFC tumor, trauma, dementia)
- Go/No-Go Test - "raise finger for 1 tap, keep still for 2 taps." Frontal patients CANNOT suppress the response to 2 taps. Failure = OFC + impaired inhibition. Also seen in ASPD, head injury, schizophrenia.
- Stroop Test - Say the INK COLOR, not the word (e.g., word "RED" printed in green ink → answer "green"). Failure of inhibition = OFC damage, OCD, impulse control disorders.
C. MEDIAL PREFRONTAL CORTEX / ANTERIOR CINGULATE CORTEX (Areas 24, 25, 32)
Functions:
- Motivation and drive
- Error monitoring and conflict detection
- Initiation of action
- Emotional regulation
If damaged:
- Profound apathy (pseudoapathetic state)
- Akinetic mutism (severe end) to mild abulia (mild end)
- Emotional blunting
- Seen in: bilateral ACA occlusion, trauma, hydrocephalus, bilateral thalamic infarction
🟣 6. BROCA'S AREA (Areas 44 & 45) - "The Speaker"
Location: Pars triangularis (Area 45) + Pars opercularis (Area 44) of inferior frontal gyrus
Hemisphere: LEFT (dominant) in most people (right-handed)
Functions:
- Production and formation of expressive speech/vocalization
- Connects with adjacent primary motor area → stimulates muscles of larynx, mouth, tongue, soft palate, respiratory muscles
If damaged - Broca's (Expressive) Aphasia:
- Loss of ability to produce speech = Expressive Aphasia = Motor Aphasia
- Patient CAN: think the words, write them, understand them (comprehension intact)
- Patient CANNOT: express in speech fluently, initiate speech, repeat, dictate
- Speech is non-fluent, laboured, telegraphic
- No paralysis of tongue/lips/vocal cords (purely cortical)
- Increased risk of MDD in these patients (they are aware and frustrated)
PART 3: THE 3 FRONTAL LOBE SYNDROMES (EXAM FAVOURITE - from PPT)
This is the most asked section. Learn these 3 syndromes with their nicknames:
| Syndrome | Other Name | Region | Core Features |
|---|---|---|---|
| Orbitofrontal Syndrome | Pseudopsychopathic state | OFC (Area 10/11) | Impulsiveness, distractibility, hyperkinesis, no empathy, no concern for others, irritable + labile mood, Witzelsucht |
| Medial Frontal Lobe Syndrome (MFLS) | Pseudoapathetic state | Medial PFC / ACC | Predominantly APATHY; spectrum from akinetic mutism → mild abulia |
| Frontal Convexity Syndrome (FCS) | Pseudodepressive state / Lateral frontal lobe syndrome | DLPFC | Executive deficits: perseveration, impersistence, difficulty planning, impaired serial order; release reflexes; soft neurological signs |
Memory trick: "P-P-D" = Pseudo-Psychopathic (OFC) | Pseudo-Apathetic (Medial) | Pseudo-Depressive (DLPFC)
"Schizophrenia is often considered to be a Frontal Convexity Syndrome" - from your PPT (exam line!)
PART 4: FRONTAL RELEASE SIGNS (Primitive Reflexes Re-Emerging)
These are reflexes that the developing frontal lobe suppresses. They return when the frontal lobe is damaged.
| Sign | How to Test | What You See |
|---|---|---|
| Grasp reflex | Stroke palm gently | Hand grasps involuntarily |
| Suck reflex | Stroke the lips | Sucking movement |
| Snout reflex | Tap the philtrum (above lips) | Lips pucker/protrude |
| Rooting reflex | Touch corner of mouth | Head turns toward stimulus |
| Glabellar tap | Tap between eyebrows repeatedly | Normal: blink stops after 3-4 taps; Abnormal: keeps blinking every tap |
| Palmomental reflex | Scratch thenar eminence (palm) | Ipsilateral chin muscle contracts |
| Gegenhalten (paratonia) | Try to passively move limb | Involuntary resistance matching your force |
Other signs to check:
- Motor impersistence - ask to hold tongue out or arms raised for 20 seconds (frontal patients cannot sustain)
- Abulia - passive, apathetic, speaks softly, markedly delayed responses
- Witzelsucht - inappropriate silly jocularity
- Confabulation - fabricates without intent to deceive
- Utilization behavior - picks up/uses random objects in front of them (e.g., wears someone else's glasses)
- Perseveration - keeps repeating same response even after question changes
- Frontal magnetic gait - small shuffling steps, feet "glued" to floor
- Incontinence - typically unconcerned about it
PART 5: COMPLETE TEST BATTERY FOR FRONTAL LOBE ASSESSMENT
I. History and Behavioral Observations
- Get history from family / other contacts - real-world behavior is the BEST test
- Watch for abulia, witzelsucht, confabulation, utilization behavior, perseveration, incontinence, inappropriate comments/touching
II. Mental Status Tests (Bedside - All in One Table)
| Test | What It Tests | Normal Score | Abnormal = |
|---|---|---|---|
| Digit Span (forward + backward) | Attention / working memory | 7 forward, 5 backward | <7 fwd, <5 bkwd |
| Months of year backward | Working memory | <15 seconds | Slow/errors |
| Serial Sevens (100-7-7-7...) | Concentration | Correct, fast | Errors, slow |
| Doubling Threes (2×3=6, ×2=12...) | Concentration (easier version) | Rapid correct answers | Stops early |
| COWAT / FAS Test | Verbal fluency (dominant frontal) | >10-12 words/letter/min | <8 = significant deficit |
| Animal/Category Naming | Frontal-temporal fluency | >15 animals/min or >10/category | <10 abnormal |
| Go-No-Go Test | Response inhibition (OFC) | Correctly holds back on 2 taps | Cannot suppress response |
| Stroop Test | Inhibition, executive function | Names ink color ignoring word | Reads word instead |
| Luria Alternating Hand Sequences | Set shifting / perseveration (DLPFC) | Rapidly alternates palm up/down | Cannot reverse, slow, errors |
| Luria Written/Manual Sequencing | Perseveration | Continues alternating pattern | Perseverates |
| Wisconsin Card Sorting Test (WCST) | Cognitive flexibility | Adapts when rules change | Cannot shift strategy |
| Trail Making Test B | Set shifting, processing speed | A-1-B-2-C-3 without errors | Cannot alternate |
| Proverb Interpretation | Abstract reasoning | Gives abstract meaning | Concrete ("rolling stone... = a stone that rolls") |
| Similarities | Abstract reasoning | "Apple & orange - both fruits" | Concrete ("both round") |
| Gambling Task (Iowa Gambling Task) | OFC decision making | Prefers long-term gains | Keeps picking high-risk |
| Conceptual Series Completion | Executive reasoning | Identifies pattern | Cannot identify |
III. Physical Exam
- Olfaction (coffee, cloves) - anosmia = OFC tumor/trauma/FTD
- Frontal release signs (above)
- Eye movements - voluntary saccades + smooth pursuit
- Gegenhalten / paratonia
- Hemiparesis / UMN signs
- Frontal gait - magnetic, shuffling
- Soft neurological signs (in FCS/schizophrenia)
IV. Formal Neuropsychological Tests
- Halstead Category Test / Milan Sorting Test - abstraction and paradigm shifting
- Porteus Maze / Reitan Trail Making - planning, regulation, checking programs
- Benton's Verbal Fluency Test - verbal skill and verbal regulation
- Figural Fluency (Five-Point Test) - nondominant frontal
V. Imaging
- MRI brain - structural atrophy, tumors, strokes
- PET / SPECT - hypofrontality (schizophrenia, depression, FTD)
- fMRI - DLPFC activation during working memory tasks
- EEG - frontal lobe epilepsy (brief, nocturnal, can mimic psychiatric episodes)
PART 6: PSYCHIATRIC DISORDERS AND FRONTAL LOBE (from PPT)
1. SCHIZOPHRENIA
- Most symptoms = PFC involvement
- Affective symptoms → Ventromedial PFC (VMPFC)
- Cognitive symptoms → DLPFC
- Aggressive symptoms → OFC
- Negative symptoms → Mesocortical areas + PFC
- Left temporal gray matter volume decrease ∝ disease severity
- Treatment: DBS over Nucleus Accumbens and Ventral Striatum
- "Schizophrenia is considered a Frontal Convexity Syndrome"
2. DEPRESSION
- Reduced DA, NE, 5-HT in PFC → cognitive dulling
- Damage to LEFT frontal lobe (stroke/lesion) → increases risk of depression
- rTMS (HIGH frequency) over DLPFC = FDA approved for treatment-resistant depression
- DBS over VMPFC (Area 25 - subgenual ACC)
3. ADHD
- Problems in executive functions of frontal cortex
- Hyperactivity → PFC
- Selective attention deficit → Dorsal Anterior Cingulate Gyrus
- Sustained attention + problem solving → DLPFC
- Impulsivity → OFC
- Frontal-striatal loop dysfunction; cortical thickness matures ~3 years late
4. OCD
- CSTC loop abnormality (Cortico-Striato-Thalamo-Cortical)
- Mainly OFC involved (OFC hypermetabolism)
- Low 5-HT levels in frontal lobe
- rTMS (LOW frequency) over SMA and OFC (not FDA approved)
- Increased OFC + caudate metabolism is characteristic
5. DEPRESSION FROM BROCA'S APHASIA
- Expressive aphasia → patient is aware they cannot speak → increased risk of MDD
6. ALCOHOLISM
- PFC linked to impulse control → PFC damage → increased binge drinking behavior
7. FRONTOTEMPORAL DEMENTIA (FTD)
- Neary criteria core features:
- Early decline in social and personal conduct
- Emotional blunting
- Loss of insight
- Relative sparing of memory and visuospatial function early on
- Executive function affected more than memory
Two variants:
- Behavioural variant (bvFTD): disinhibition, apathy, loss of empathy, perseveration, stereotyped/compulsive behaviour, hyperorality, dietary changes
- Semantic variant: speech production, word finding, object naming, grammar, comprehension affected
8. FRONTAL LOBE EPILEPSY
- Bizarre presentation with physical/emotional aura, tingling, numbness, tension
- Fear on face, tonic posturing, clonic movements
- Can be Simple or Complex partial seizure
- Multiple brief episodes daily, often nocturnal
- Often NO post-ictal deficits - this leads to misdiagnosis as psychiatric/psychogenic episodes!
- 20-30% of operative procedures for intractable epilepsy
- Specific features by area:
- Dorsolateral: contraversive head/eye turning, aphasia (dominant)
- SMA: fencing posture, speech arrest, unusual sounds
- Orbitofrontal/cingulate: elaborate motor automatisms, autonomic changes, olfactory hallucinations
PART 7: ONE-PAGE MEMORY CHEAT SHEET
FRONTAL LOBE = SOCIAL LOBE = NEWEST LOBE
AREA 4 → Primary Motor → Damage = Contralateral hemiparesis
AREA 6 → Premotor/SMA → Damage = Proximal weakness/Apraxia/Akinesia+Mutism
AREA 8 → Frontal Eye Fields → Destructive = Eyes look AT lesion
AREA 44/45 → Broca → Damage = Expressive (non-fluent) aphasia
AREA 9/46 → DLPFC → Damage = Apathy, perseveration, poor working memory
AREA 10/11 → OFC → Damage = Disinhibition, impulsivity, witzelsucht
AREA 24/25 → Medial PFC/ACC → Damage = Akinetic mutism, apathy
THE 3 SYNDROMES:
OFC damage = Pseudo-PSYCHOPATHIC (disinhibited)
Medial damage = Pseudo-APATHETIC (akinetic mutism → abulia)
DLPFC damage = Pseudo-DEPRESSIVE (executive failure)
TESTS TO REMEMBER:
FAS (COWAT) > 10-12 per letter
Go-No-Go = OFC inhibition
WCST = DLPFC flexibility
Stroop = OFC inhibition
Luria = Perseveration
Trail B = Set shifting
Digit span = 7 forward / 5 backward
PSYCHIATRIC LINKS:
Schizophrenia = Hypofrontality (DLPFC)
Depression = Left frontal → rTMS high freq DLPFC (FDA approved)
OCD = OFC hyperactivity → rTMS low freq OFC
ADHD = Frontostriatal circuit
FTD = OFC+DLPFC degeneration
Alcoholism = OFC/PFC damage → impulse loss
PART 8: CLASSIC CASE TO QUOTE IN EXAM (Phineas Gage)
Phineas Gage (1848): A 25-year-old railroad worker had an iron rod driven through both frontal lobes in an explosion. He survived physically, but his personality changed completely. He became "fitful, irreverent, profane, impatient, unable to follow advice, no longer able to follow plans" - his friends said "he was no longer Gage." This is the prototype of orbitofrontal syndrome/disinhibition syndrome.
Reference: Brain & Behaviour, David Clark, Nash Boutons, Mario Mendez, 3rd Edition, Pg 84-121 | Kaplan & Sadock's Comprehensive Textbook of Psychiatry | Harrison's Principles of Internal Medicine 22E | Neuroanatomy through Clinical Cases 3rd Ed | Adams & Victor's Principles of Neurology 12th Ed
This is a shared conversation. Sign in to Orris to start your own chat.