Obesity Mangement in 2026: Beyond wight loss - The expanding role of GLP-1 receptor agonist and dual/ trinkincretin therapy. 1. "Introduction / Changing concept of obesity 2. "Pathophysiology of obesity / Why life style therapy alone fails" 3. "Recent advances (2025-2026) / Evolution of anti obesity drugs" Very very super detailed answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"GLP-1 receptor agonist" AND obesity
Searching the Web
GLP-1 dual triple incretin therapy obesity 2025 2026 retatrutide CagriSema tirzepatide advances
Reading File
Reading File
Reading File
Searching PubMed
"incretin" AND "obesity" AND "tirzepatide OR retatrutide"
Reading Web Page
https://www.docwirenews.com/post/ada-2026-obesity-drug-updat…
Reading File
Reading File
Reading File
Reading Article
PMID: 39719170
Reading Article
PMID: 39952695
Reading Article
PMID: 40960239
Reading File
Finding Sources
Reading Article
PMID: 39181597
Reading Article
PMID: 38850440
Searching PubMed
"retatrutide" AND "obesity" AND "weight loss"
Reading File
Reading File
Reading Article
PMID: 40563436
Reading Article
PMID: 39160334
Reading File
Loading Image
Obesity Management in 2026: Beyond Weight Loss
The Expanding Role of GLP-1 Receptor Agonists and Dual/Triple Incretin Therapy
SECTION 1: Introduction / Changing Concept of Obesity
1.1 The Old Paradigm: "A Matter of Willpower"
For most of the 20th century, obesity was framed as a behavioral problem - a personal failure of diet discipline and physical inactivity. Treatment was caloric restriction and "eat less, move more" counseling, and pharmacotherapy was either non-existent or dominated by stimulants (amphetamines) that proved dangerous. This framework produced a culture of stigma: patients internalized blame, clinicians under-treated the condition, and insurers refused coverage on the grounds that obesity was "self-inflicted."
The consequences of this paradigm were devastating. Billions of dollars were spent on dietary programs that failed to produce durable weight loss in the vast majority of patients. The history of antiobesity pharmacotherapy is, as one 2025 systematic review in Pharmacological Reviews notes, "marked by disappointments, often entangled with societal pressure promoting weight loss and the prevailing conviction that excess body weight signifies a lack of willpower."
1.2 The Paradigm Shift: Obesity as a Chronic, Relapsing Neurobiological Disease
Modern science has dismantled the "willpower" paradigm entirely. Obesity is now formally defined as a chronic disease of energy balance driven by dysregulated interactions involving satiety factors and the central nervous system, resulting in increased caloric intake and an excess in adipose tissue mass. The increase in adiposity causes chronic complications conferring increased morbidity and mortality. - Fuster and Hurst's The Heart, 15th Edition, p. 266
This reconceptualization has several critical implications:
A. Obesity is not a lifestyle choice - it is a neurobiological disorder. The hypothalamus, not willpower, is the primary driver of long-term body weight regulation. When patients lose weight through lifestyle measures, compensatory neurobiological mechanisms actively restore that weight: leptin levels fall, NPY/AgRP orexigenic signaling surges, resting metabolic rate drops (metabolic adaptation), and hunger intensifies disproportionately. These are not character flaws; they are hardwired survival responses.
B. The disease is lifelong. Like hypertension or type 2 diabetes (T2D), obesity requires lifelong management. Stopping treatment leads to relapse - a fact now solidly proven by withdrawal studies of semaglutide and tirzepatide showing two-thirds weight regain within one year.
C. Complications define severity, not BMI alone. BMI, while practical, "conveys little information about how excess adiposity adversely affects health." - Fuster and Hurst's The Heart, p. 277
1.3 Adiposity-Based Chronic Disease (ABCD): A New Diagnostic Framework
To move beyond the limitations and stigma of the term "obesity," the concept of Adiposity-Based Chronic Disease (ABCD) has been formally proposed. As detailed in Hurst's The Heart, ABCD is a diagnostic term that:
- Defines what we are treating: Abnormalities in the mass, distribution, or function of adipose tissue (not merely body weight or BMI).
- Defines why we are treating it: As a chronic disease with complications that confer morbidity, mortality, and impaired quality of life.
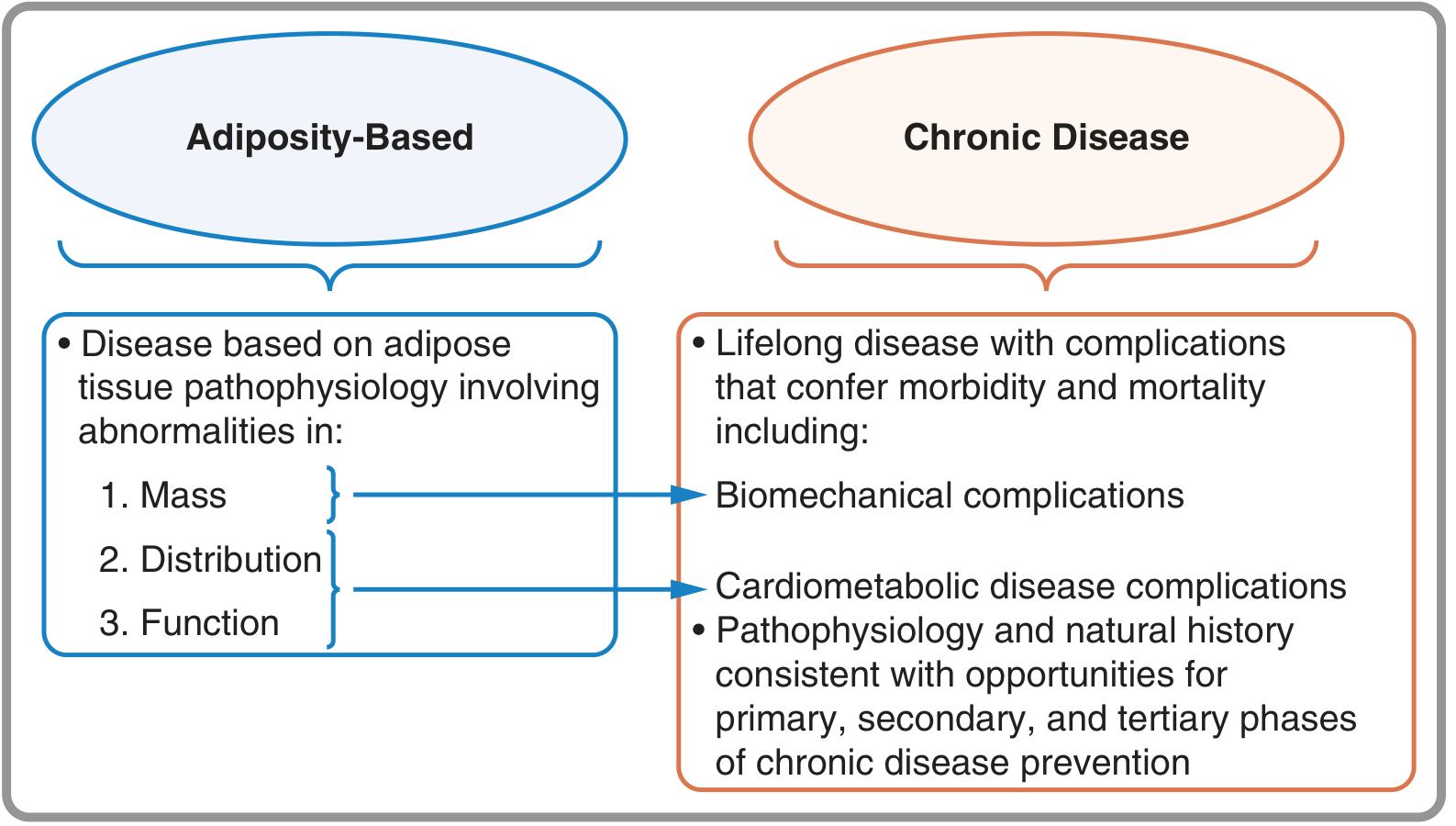
The ABCD framework identifies two axes of complications:
- Biomechanical complications: Due to excess adipose tissue mass - obstructive sleep apnea (OSA), osteoarthritis, stress urinary incontinence, GERD.
- Cardiometabolic complications (CMD): Due to abnormal distribution and function of adipose tissue - T2D, dyslipidemia, hypertension, atherosclerotic cardiovascular disease (ASCVD), non-alcoholic/metabolic steatohepatitis (MASH), polycystic ovary syndrome (PCOS), chronic kidney disease.
Crucially, the ABCD model also explains the paradox of "metabolically healthy obesity" (MHO): some individuals with elevated BMI have insulin-sensitive adipose tissue, do not develop visceral fat, and carry mainly biomechanical but not cardiometabolic risk. Conversely, lean individuals may accumulate dysfunctional visceral/ectopic fat and carry high metabolic risk. This explains why a complications-focused, staging-based approach - not BMI alone - should determine treatment intensity. - Fuster and Hurst's The Heart, 15th Edition, p. 266-267
1.4 The Expanded Goals of Obesity Treatment in 2026
The treatment paradigm has shifted from "weight loss" to "reducing obesity-related complications and improving health outcomes." In 2026, success is no longer measured only in kilograms lost. It is measured in:
- Remission of T2D
- Reduction in MACE (major adverse cardiovascular events)
- Reversal of MASH/hepatic fibrosis
- Resolution of OSA
- Slowing of CKD progression
- Improved quality of life, mobility, and mental health
As reported from the 2026 ADA Scientific Sessions (New Orleans), Dr. Michael Weintraub summarized: "What these sessions demonstrated is the field of obesity has moved beyond GLP-1s as the whole story... We are moving beyond just mean percent weight loss." The presenters discussed treatment success in terms of improvements in metabolic liver disease, obstructive sleep apnea, and T2D - not just scale readings.
SECTION 2: Pathophysiology of Obesity / Why Lifestyle Therapy Alone Fails
2.1 The Central Nervous System Architecture of Energy Balance
Understanding why lifestyle therapy fails requires understanding the neurobiological machinery that defends body weight. The system is ancient, designed for survival in food-scarce environments, and powerfully biased toward weight gain and weight defense.
The central processor of energy balance is the arcuate nucleus of the hypothalamus, which integrates peripheral signals via two populations of first-order neurons:
| Neuron Type | Signal | Function |
|---|---|---|
| POMC/CART neurons | Activated by leptin, insulin, GLP-1, PYY | Catabolic: reduce food intake, increase energy expenditure via α-MSH → MC3/4R |
| NPY/AgRP neurons | Inhibited by leptin, insulin; activated by ghrelin, energy deficit | Anabolic: increase appetite, reduce energy expenditure via Y1/Y5 receptors |
These first-order neurons signal second-order neurons along catabolic (MC3/4R) and anabolic (Y1/Y5) pathways, which in turn modulate the autonomic nervous system, endocrine system, and behavioral outputs. - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 421-422
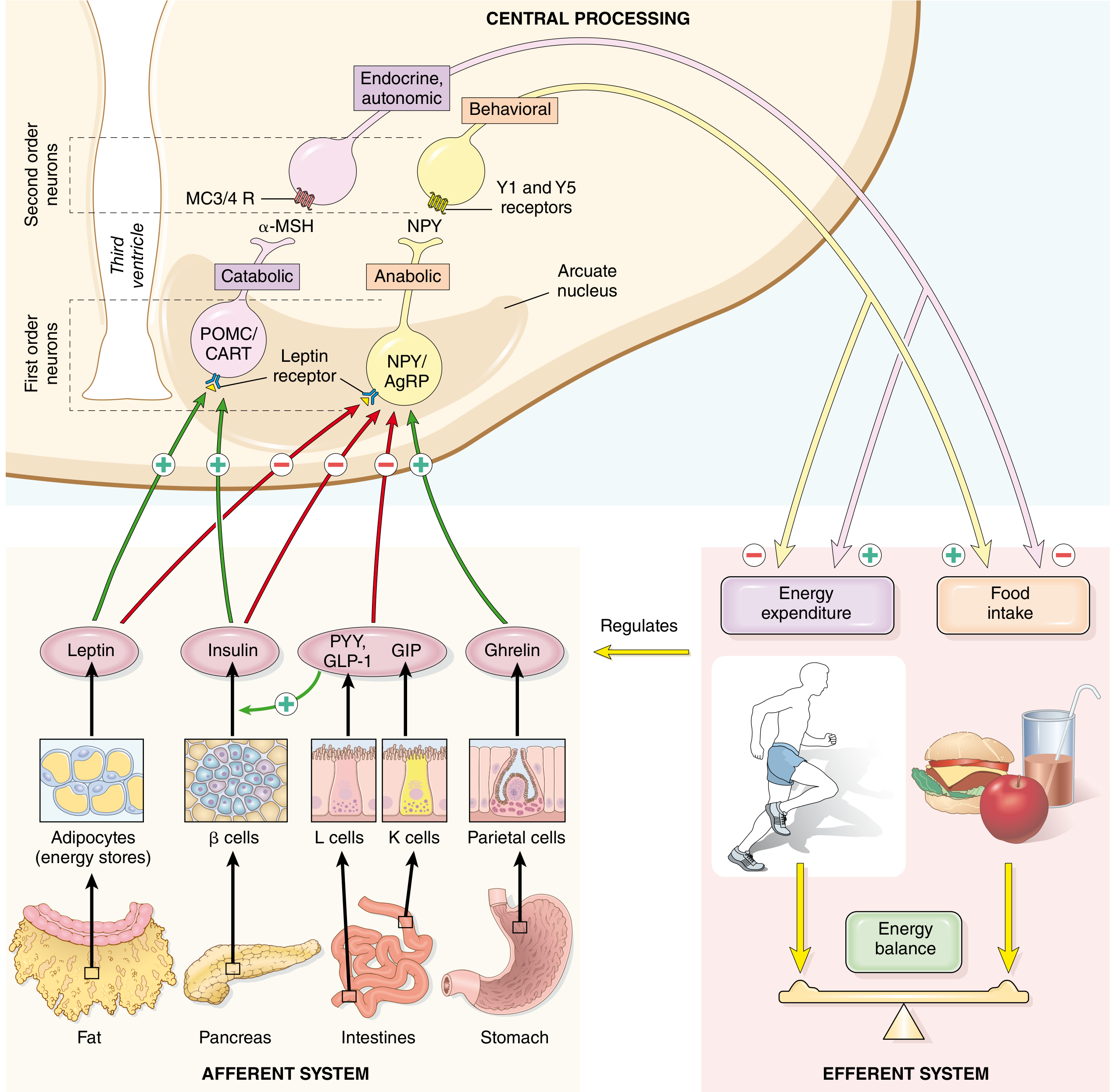
2.2 Key Peripheral Hormones in Energy Regulation
Leptin
- Source: Adipocytes; output is proportional to fat stores.
- Action: Crosses blood-brain barrier to stimulate POMC/CART (appetite-suppressing) neurons and inhibit NPY/AgRP (appetite-promoting) neurons. Also stimulates thermogenesis via sympathetic innervation of adipose tissue.
- In obesity: Despite high circulating leptin levels (proportional to fat mass), leptin resistance develops. This is believed to result from hypothalamic microglial inflammation triggered by excess free fatty acids crossing the blood-brain barrier, impairing leptin receptor signaling. The result: obese individuals have high leptin yet cannot use it to suppress appetite. - Robbins & Kumar Basic Pathology, p. 421-423
- Clinical implication: Injecting leptin into obese humans fails to reduce appetite or body weight - dashing early hopes for leptin therapy.
Ghrelin
- Source: Gastric parietal cells.
- The only known gut hormone that increases food intake (orexigenic).
- Activates NPY/AgRP neurons; levels rise pre-meal and fall 1-2 hours postprandially. Importantly, this post-meal drop is attenuated in obese individuals, prolonging the hunger drive. After bariatric surgery (gastric bypass), ghrelin levels fall dramatically - a mechanism partly responsible for surgery's effectiveness beyond mere restriction.
GLP-1 (Glucagon-Like Peptide-1)
- Source: L-cells of the distal ileum and colon; released after food intake.
- Actions:
- Pancreatic: Glucose-dependent insulin secretion from β-cells; glucagon suppression from α-cells.
- Gastric: Slows gastric emptying → promotes satiety.
- Hypothalamic: Acts via sensory afferents and direct brain GLP-1 receptors to stimulate POMC/CART neurons, suppress NPY/AgRP neurons → reduces food intake and caloric consumption.
- Extra-metabolic: Cardioprotective (reduces MACE), anti-inflammatory, renoprotective, hepatoprotective.
- In obesity: GLP-1 secretion may be impaired, and the hypothalamic response to GLP-1 signals can be blunted by obesity-associated neuroinflammation. This creates a therapeutic window for pharmacological GLP-1 receptor agonism at supraphysiologic doses. - Guyton and Hall Medical Physiology, p. 877-878
GIP (Glucose-Dependent Insulinotropic Polypeptide)
- Source: K-cells of the duodenum and jejunum.
- Primary role: Potentiates glucose-stimulated insulin release (incretin effect).
- In obesity: GIP's role is paradoxical. In obese/T2D states, the direct GIP receptor pathway in hypothalamus becomes resistant. However, dual GLP-1/GIP receptor agonism (tirzepatide) achieves superior weight loss compared to GLP-1 agonism alone. The mechanism may involve GIP-mediated effects on adipocyte function, reduction in visceral fat, and synergistic CNS satiety signaling. - Guyton and Hall Medical Physiology, p. 895
PYY (Peptide YY)
- Source: L-cells (same as GLP-1); released postprandially.
- Acts centrally to inhibit NPY/AgRP neurons → reduces appetite. PYY levels are lower in obese individuals at baseline.
2.3 Adipose Tissue Dysfunction: The Engine of Metabolic Complications
In obesity, adipose tissue undergoes qualitative changes that are as important as quantitative expansion:
1. Visceral vs. Subcutaneous Fat:
Visceral (intraabdominal) adipose tissue is far more metabolically dangerous than subcutaneous fat. It has higher lipolytic activity, is more prone to macrophage infiltration, and secretes larger quantities of pro-inflammatory adipokines (TNF-α, IL-6, resistin, MCP-1) while secreting less adiponectin.
2. Macrophage Infiltration and Chronic Low-Grade Inflammation:
As adipocytes hypertrophy, they release free fatty acids and damage-associated molecular patterns (DAMPs) that recruit macrophages in a "crown-like structure" pattern. This produces a state of chronic low-grade inflammation - a critical mechanism connecting obesity to insulin resistance, T2D, ASCVD, MASH, and even some cancers.
3. Adiponectin Deficiency:
Adiponectin stimulates fatty acid oxidation in skeletal muscle and reduces hepatic glucose production - called the "guardian angel against obesity." Obese individuals have low adiponectin, worsening insulin resistance and atherogenesis. Elevated free fatty acids crossing the blood-brain barrier also promote hypothalamic leptin resistance via microglial activation. - Robbins, Cotran & Kumar Pathologic Basis of Disease
4. Ectopic Lipid Accumulation:
When insulin-resistant adipocytes cannot accommodate excess fuel storage, free fatty acids spill into liver (MASH), skeletal muscle (insulin resistance), heart (lipotoxic cardiomyopathy), and kidney (CKD).
5. Epigenetic Programming:
Parental obesity induces epigenetic changes (DNA methylation, histone modifications, microRNA expression) that predispose offspring to obesity in the absence of DNA sequence changes. These germ cell epigenetic effects may perpetuate obesity risk across generations. - Guyton and Hall Medical Physiology, p. 875
2.4 Genetic and Neurological Underpinnings
- Monogenic obesity: Loss-of-function mutations in leptin, leptin receptor, POMC, PCSK1, MC4R gene - the last found in 4-5% of patients with massive obesity. These directly impair the hypothalamic satiety circuit.
- Polygenic obesity: Hundreds of common variants each contribute small effects; these interact with obesogenic environments (high caloric density food, sedentary behavior, sleep disruption, stress).
- Prader-Willi syndrome: Deletion of chromosome 15q causing extreme hyperphagia from hypothalamic dysfunction - the archetypal model of neurogenic obesity.
- Neurogenic abnormalities: Hypothalamic lesions, tumors compressing the ventromedial nucleus, and functional dysregulation of feeding circuits all cause obesity independent of caloric intake.
2.5 Why Lifestyle Therapy Alone Fails: The Adaptations Against Weight Loss
This is perhaps the most clinically important concept in obesity medicine. When a patient with obesity restricts calories and loses weight:
| Adaptive Response | Mechanism | Effect |
|---|---|---|
| Metabolic adaptation | Suppression of resting metabolic rate beyond what fat mass loss alone would predict | Caloric deficit narrows; weight loss stalls |
| Compensatory hyperphagia | Leptin drops, ghrelin rises, NPY/AgRP signaling surges | Intense, persistent hunger - more powerful than in lean individuals |
| Reduced satiety hormone response | Lower postprandial GLP-1, PYY release | Food feels less satiating |
| Reduced thermogenesis | Leptin-mediated sympathetic drive diminishes | Less passive energy expenditure |
| Psychological drive | Hedonic reward circuits activated by food cues | Food becomes more appealing and rewarding |
An obese person who has reduced to normal weight "develops intense hunger demonstrably far greater than that of a normal person. Also, diet-induced weight loss in obese people is associated with substantial metabolic adaptation." - Guyton and Hall Medical Physiology, p. 876
These are not temporary - they persist for years after weight loss, which is why clinical studies consistently show that lifestyle-only interventions produce average weight losses of only 3-5% at 1 year and substantial regain thereafter. Pharmacotherapy is not an adjunct to lifestyle therapy - it is a pharmacological correction of a dysfunctional neurobiological setpoint.
2.6 The Insulin Resistance-Adiposity Loop
In insulin-resistant individuals, weight gain creates a vicious cycle:
- Visceral fat expands asymmetrically → more FFA → worsens insulin resistance → β-cells overwork → eventual T2D
- Insulin resistance + elevated FFA → hepatic de novo lipogenesis → MASH → cirrhosis
- Chronic hyperinsulinemia + dyslipidemia → accelerated atherosclerosis → ASCVD
Crucially, insulin resistance in muscle impairs glucose uptake, forcing skeletal muscle to rely on fat oxidation, depleting lean mass over time and further worsening metabolic rate. This muscle-fat interplay is one reason why muscle preservation during pharmacological weight loss is now a major clinical concern - particularly relevant as we discuss GLP-1 agonist-associated lean mass loss. - Fuster and Hurst's The Heart, p. 272-275
SECTION 3: Recent Advances (2025-2026) / Evolution of Anti-Obesity Drugs
3.1 Historical Context: The Drug Development Timeline
| Era | Agent | Mechanism | Outcome |
|---|---|---|---|
| 1950s-70s | Amphetamines, diethylpropion | CNS stimulants, dopamine/NE release | Short-term only; abuse risk |
| 1990s | Fenfluramine/phentermine ("fen-phen") | Serotonergic + NE | Withdrawn 1997 - cardiac valve disease |
| 1999 | Orlistat | Pancreatic lipase inhibitor | 30% fat absorption reduction; ~3-4% weight loss; GI side effects |
| 2012 | Phentermine/topiramate (Qsymia) | NE release + GABA modulation | ~8-10% weight loss |
| 2012 | Bupropion/naltrexone (Contrave) | NE/DA + opioid antagonist | ~5-6% weight loss |
| 2014 | Liraglutide 3.0 mg (Saxenda) | GLP-1 RA | ~6-8% weight loss |
| 2021 | Semaglutide 2.4 mg sc (Wegovy) | GLP-1 RA (long-acting) | ~15% weight loss - paradigm shift |
| 2023 | Tirzepatide (Zepbound) | GLP-1 + GIP dual RA | ~21-22.5% weight loss |
| 2025-26 | Oral GLP-1s, triple agonists | Expanding mechanisms | 20-30%+ weight loss - surgery range |
3.2 GLP-1 Receptor Agonists: The First Transformation
Mechanism of Action (Detailed)
GLP-1 RAs are synthetic analogs of native GLP-1, engineered for prolonged half-life. They activate the GLP-1 receptor (GLP-1R) - a G-protein coupled receptor linked to adenylate cyclase/cAMP signaling - in multiple tissues simultaneously:
1. Pancreas:
- β-cells: Glucose-dependent ↑ insulin secretion (self-limiting - no hypoglycemia at euglycemia)
- α-cells: ↓ glucagon secretion
- β-cell preservation: May reduce apoptosis and promote β-cell neogenesis
2. Brain (Central - the key for weight loss):
- Hypothalamic arcuate nucleus: Activates POMC/CART → suppresses appetite
- Inhibits NPY/AgRP neurons
- Vagal afferents relay GLP-1 signals from gut to nucleus tractus solitarius (NTS) in brainstem → satiety
- Reduces hedonic (reward-based) eating by modulating mesolimbic dopamine circuits (nucleus accumbens, ventral tegmental area)
- Area postrema (circumventricular organ): Directly senses circulating GLP-1, contributes to nausea at high doses
3. Gastrointestinal:
- Slows gastric emptying → prolonged satiety, reduced postprandial glucose excursions
- Reduces gastrointestinal motility (explains nausea/vomiting/constipation side effects)
4. Cardiovascular:
- Direct cardiac GLP-1R: Modest chronotropy, improved left ventricular function
- Anti-atherosclerotic: Reduced endothelial inflammation, improved lipid profile
- Blood pressure lowering (mild)
- The SELECT trial (NEJM 2023, Lancet 2024 HF sub-analysis): Semaglutide 2.4 mg reduced MACE by 20% (HR 0.80) in 17,604 patients with established CVD and obesity - the first time an obesity drug had proven cardiovascular outcome benefit independent of T2D. In those with coexistent heart failure, semaglutide reduced MACE (HR 0.72), composite HF outcomes (HR 0.79), and cardiovascular death (HR 0.76). - Deanfield et al., Lancet 2024, PMID 39181597
5. Kidney:
- Reduces glomerular hyperfiltration, albuminuria, inflammatory pathways in podocytes
- GLP-1R expression in tubular cells: Reduces oxidative stress and inflammation
6. Liver:
- Reduces hepatic steatosis, de novo lipogenesis
- Weight-loss mediated and possibly direct anti-inflammatory effects on hepatic stellate cells (being studied in MASH trials)
Semaglutide 2.4 mg (Wegovy) - The Reference Standard
- STEP 1 trial: 68-week treatment → -14.9% mean body weight vs -2.4% placebo (68% achieved ≥5% weight loss)
- STEP 10 trial (Lancet Diabetes Endocrinol 2024): Semaglutide 2.4 mg in patients with obesity and prediabetes → -15.3% weight loss; critically, 79.7% of participants had normoglycemia at 68 weeks vs 27.5% placebo. This suggests GLP-1 RA therapy may prevent T2D at a population scale. - McGowan et al., Lancet Diabetes Endocrinol 2024, PMID 39089293
- A 2025 systematic review and meta-analysis confirmed semaglutide's favorable cardiovascular safety and outcome profile.
3.3 Tirzepatide (Zepbound/Mounjaro) - The Second Transformation: GLP-1 + GIP Dual Agonism
Tirzepatide is the first approved dual incretin receptor agonist (GIP/GLP-1 RA), a single synthetic peptide that acts on both GIP receptor and GLP-1R.
Why GIP Addition Matters
GIP alone has a paradoxical relationship with obesity (its direct receptor may be resistant in obese states), but when combined with GLP-1R agonism:
- GIP reduces GLP-1R agonist-associated nausea, improving tolerability
- GIP has direct effects on adipocyte lipolysis and fat distribution - promotes fat oxidation, reduces visceral adiposity
- GIP receptors in the CNS (hippocampus, hypothalamus) may complement GLP-1 satiety pathways
- The combination achieves "synergistic" weight loss far beyond either alone
Clinical Data (SURMOUNT Program + Meta-Analysis)
A 2024 meta-analysis including SURMOUNT-2 (PMID 38850440) confirmed dose-dependent weight loss:
- Tirzepatide 5 mg: -8.07% body weight vs placebo
- Tirzepatide 10 mg: -10.79%
- Tirzepatide 15 mg: -11.83% (absolute: -11.5 kg)
- In non-diabetic patients (SURMOUNT-1): up to 22.5% mean weight loss at 72 weeks; 36.2% achieved ≥25% weight loss at highest dose
A landmark 2025 network meta-analysis (Karakasis et al., Metabolism, PMID 39719170) including 22 RCTs (2,258 participants) revealed:
- GLP-1 RAs reduce total body weight (-3.55 kg), fat mass (-2.95 kg), and lean mass (-0.86 kg)
- Lean mass loss constitutes ~25% of total weight lost - raising sarcopenia concerns
- Tirzepatide 15 mg achieved the greatest fat mass reduction but also among the greatest lean mass reduction
- Important clinical implication: concurrent resistance exercise training is now recommended to mitigate lean mass loss during incretin therapy
Non-Weight Cardiometabolic Benefits of Tirzepatide (2025-2026)
- SURPASS-CVOT (2026): Tirzepatide significantly reduced major kidney events compared to dulaglutide in T2D - the first kidney outcome benefit demonstrated for a dual incretin
- OSA improvement: Clinical trials show improvement in AHI (apnea-hypopnea index) with tirzepatide, independent of weight loss
- MASH: Dedicated trials showing histological improvement in hepatic steatosis and fibrosis
3.4 The 2025-2026 Frontier: Drugs That Are Rewriting What Is Medically Achievable
A. CagriSema (Semaglutide + Cagrilintide) - GLP-1 + Amylin Dual Agonism
Mechanism:
- Semaglutide (GLP-1 RA): Central appetite suppression, satiety, slowed gastric emptying
- Cagrilintide (long-acting amylin analog): Amylin is a peptide co-secreted with insulin from β-cells. It promotes satiety via area postrema, reduces glucagon, slows gastric emptying. Amylin and GLP-1 act on complementary, non-overlapping pathways in the brainstem and hypothalamus - providing additive and potentially synergistic satiety.
CagriSema targets entirely different receptor biology from tirzepatide (no GIP component), representing a distinct pharmacological strategy.
REDEFINE Phase 3 Trial Results:
- ~20-23% average weight loss at 68 weeks
- Over 40% of participants lost ≥25% body weight - approaching bariatric surgery outcomes
- Favorable metabolic profile with significant glycemic benefit
- FDA submission filed: December 2025
- Potential approval: Late 2026 / Early 2027
B. Retatrutide - Triple Receptor Agonism (GLP-1 + GIP + Glucagon): The Paradigm Redefiner
Retatrutide (Eli Lilly) is the most potent pharmacological weight loss agent in clinical development. It is a unimolecular triple receptor agonist - a single peptide acting simultaneously at three receptors.
Molecular Mechanism:
| Receptor | Effect |
|---|---|
| GLP-1R | Appetite suppression, slower gastric emptying, glucose-dependent insulin release |
| GIPR | Enhanced insulin secretion, adipocyte lipolysis, reduced GI side effects, CNS satiety |
| Glucagon receptor (GCGR) | ↑ Energy expenditure, ↑ hepatic fat oxidation, ↑ thermogenesis, ↑ lipolysis in adipose tissue, ↑ basal metabolic rate |
The addition of glucagon receptor agonism is the key innovation. Glucagon increases energy expenditure through several pathways:
- Stimulates hepatic glycogenolysis and gluconeogenesis (raises basal metabolic rate)
- Activates brown adipose tissue (BAT) thermogenesis
- Promotes hepatic fatty acid β-oxidation (anti-steatotic)
- Increases ureagenesis (protein turnover signaling)
Normally, glucagon receptor agonism would be hyperglycemic - but the simultaneous GLP-1R and GIPR agonism provides potent counter-regulatory glucose lowering, making the glycemic balance net neutral or beneficial.
Clinical Data:
Phase 2 (NEJM 2023):
- 96 mg dose: -24.2% body weight at 48 weeks (non-diabetic patients with obesity) - highest weight loss ever reported in a pharmacological obesity trial at that time
Phase 3 TRIUMPH Program (Eli Lilly):
- 4 trials, >5,800 participants
- Enrolling: obesity/weight management, OSA, knee osteoarthritis, cardiovascular outcomes
- TRANSCEND trial (weight management, Phase 3, presented ADA 2026 Scientific Sessions):
- Primary outcome: weight change at 80 weeks
- ~20% weight loss in intent-to-treat; >30% weight loss in the per-protocol (on-drug) extension arm at 104 weeks - fully in the bariatric surgery range
- TRANSCEND-T2D: Robust HbA1c reduction of ~2.0% - comparable to semaglutide and tirzepatide T2D trials
- A 2025 systematic review and network meta-analysis (Yan et al., Acta Diabetologica) confirmed retatrutide achieved greatest weight reduction among all agents, while tirzepatide showed greater glycemic control
- Potential FDA submission: Late 2026 - Early 2027
A detailed 2025 review (Katsi et al., Biomolecules, PMID 40563436) characterized retatrutide's unique molecular structure and confirmed phase 2 findings of dose-dependent weight loss, HbA1c reduction, liver steatosis improvement, and renoprotective effects. Common adverse effects are GI (nausea, vomiting, diarrhea) and dose-dependent - consistent with the class.
C. Oral Small-Molecule GLP-1 Receptor Agonists: Democratizing Access
The biggest practical barrier to GLP-1 RA use globally has been the requirement for subcutaneous injection. Several oral agents are now clinical reality:
1. Oral Semaglutide 50 mg (Rybelsus escalated dose):
- The first approved oral GLP-1 RA (at 7/14 mg for T2D)
- The 50 mg dose for obesity completed Phase 3: -15.1% body weight at 68 weeks - nearly equivalent to injectable semaglutide
- Requires fasting administration, specific absorption conditions (sodium N-[8-(2-hydroxybenzoyl)aminocaprylate] - SNAC carrier)
2. Orforglipron (Eli Lilly) - Phase 3 ATTAIN-1 Trial (NEJM 2025):
- A small-molecule, nonpeptide, oral GLP-1 RA - not a peptide and does not require fasting
- Phase 3 (3,127 patients, 72 weeks, PMID 40960239 - NEJM 2025):
- Orforglipron 6 mg: -7.5% body weight vs -2.1% placebo
- Orforglipron 12 mg: -8.4%
- Orforglipron 36 mg: -11.2% (54.6% achieved ≥10% loss; 18.4% achieved ≥20%)
- Significant improvements in waist circumference, systolic BP, triglycerides, non-HDL cholesterol
- Adverse events: GI (nausea, vomiting - mostly mild/moderate), consistent with the GLP-1 RA class
- This represents a once-daily pill for obesity - potentially far more accessible than injectables, especially in lower-income countries and patients with needle phobia
3. ECC5004/AZD5004 (AstraZeneca):
- Novel once-daily oral small-molecule GLP-1 RA
- First-in-human characterization published (Haggag et al., Diabetes Obes Metab 2025, PMID 39495140)
- Phase 1/2 data showing favorable pharmacokinetics and early weight loss signals
4. Ecnoglutide (biased GLP-1 RA):
- A "biased" agonist - selectively activates specific downstream GLP-1R signaling pathways (preferentially cAMP vs. β-arrestin pathways) to potentially achieve weight loss with reduced GI side effects
- Phase 3 (Ji et al., Lancet Diabetes Endocrinol 2025, PMID 40555243): significant weight loss in Chinese patients with overweight/obesity; positive efficacy with favorable safety profile
D. Survodutide (GLP-1 + Glucagon Dual Agonist)
- Unlike retatrutide (triple), survodutide (Boehringer Ingelheim/Zealand) is a GLP-1 + glucagon receptor dual agonist (no GIP component).
- Phase 3 results (June 2026): Two phase 3 trials confirmed weight loss with improvement in metabolic health and MASLD (Metabolic dysfunction-Associated Steatotic Liver Disease).
- Mean weight loss: ~14.9% at 49 weeks in Phase 2.
- Particularly strong MASH/MASLD data - hepatic fat reduction and histological improvement.
- The glucagon component promotes hepatic fat oxidation - potentially making this a dual-purpose obesity + liver disease drug.
E. Amycretin - Unimolecular GLP-1 + Amylin Dual Agonist
- Where CagriSema is a combination of two separate molecules (semaglutide + cagrilintide), amycretin is a single unimolecular peptide fusing GLP-1 and amylin agonism in one molecule.
- Phase 2 data: remarkable weight loss signal (~13.1% in 12 weeks - implying projected losses exceeding any approved agent over full course)
- Phase 3 underway as of 2026
- Potential advantage: simpler manufacturing, single administration, potentially optimized receptor co-activation pharmacokinetics
F. Non-Incretin Mechanisms in the Pipeline
Beyond incretin biology, a diverse array of mechanisms is advancing:
| Agent/Class | Mechanism | Status (2026) |
|---|---|---|
| Setmelanotide | MC4R agonist | Approved for MC4R-deficiency related monogenic obesity; Phase 2 for polygenic obesity |
| Bimagrumab | Anti-ActRII (activin receptor) | Preferentially reduces fat mass, increases lean mass - complementary to GLP-1 RAs |
| Mazdutide | GLP-1 + GCGR dual agonist | Phase 3 ongoing (Chinese population); similar mechanism to survodutide |
| Melanocortin-4 receptor agonists | Central appetite suppression | Multiple agents in Phase 1/2 |
| NASH/MASH combinations | GLP-1 + FGF21 analog (efruxifermin) | Phase 2 data: MASH resolution with combination (Harrison et al., Clin Gastroenterol Hepatol 2025, PMID 38447814) |
| Peptide YY analogs | PYY3-36 analogs | Early phase |
| Mitochondrial uncouplers | ↑ basal thermogenesis | Preclinical/early phase |
3.5 Comparative Efficacy: The Weight Loss Hierarchy (2026)
Based on current evidence, approximate weight losses (mean % from baseline) in head-to-head or indirect comparisons:
Retatrutide (Phase 3, on-drug) ~30%+ at 2 years
CagriSema (Phase 3) ~20-23%
Tirzepatide 15 mg (Phase 3) ~22.5% (non-diabetic)
Semaglutide 2.4 mg sc (Phase 3) ~15%
Oral semaglutide 50 mg ~15%
Survodutide ~14.9%
Orforglipron 36 mg (Phase 3) ~11.2%
Liraglutide 3 mg (Phase 3) ~6-8%
─────────────────────────────────────────
Bariatric surgery (RYGB) ~25-35%
The frontier agents (retatrutide, CagriSema) are now overlapping with bariatric surgery outcomes - a medical milestone that was unthinkable a decade ago.
3.6 Beyond Weight Loss: Organ-Specific Benefits Emerging in 2025-2026
Cardiovascular
- SELECT trial (semaglutide): 20% MACE reduction in obesity + established CVD (no T2D required)
- HF benefit: HR 0.72 for MACE in patients with coexistent HF; both HFpEF and HFrEF benefited
- SURMOUNT-CVOT (tirzepatide, 2026): Significant reduction in major kidney events vs dulaglutide; eGFR decline slowed
- Emerging: retatrutide cardiovascular outcomes trial (part of TRIUMPH program) ongoing
Obstructive Sleep Apnea (OSA)
- Tirzepatide: Phase 3 OSA trials (SURMOUNT-OSA 1 & 2) demonstrated >50% reduction in AHI
- Retatrutide OSA trial: Part of TRIUMPH program
- GLP-1 RAs appear to reduce OSA partly through fat mass reduction (pharyngeal fat), and possibly through direct respiratory neural effects
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD/MASH)
- Semaglutide Phase 3 (ESSENCE trial): MASH resolution in ~62% vs 34% placebo; fibrosis improvement in ~37% vs 22%
- Survodutide: Two Phase 3 trials showing MASLD improvement (June 2026)
- GLP-1 + FGF21 (efruxifermin) combination: Phase 2 results (PMID 38447814) showing MASH resolution in 79% at 24 weeks
Chronic Kidney Disease
- GLP-1 RAs reduce urinary albumin-creatinine ratio, slow eGFR decline
- Tirzepatide: SURPASS-CVOT kidney data (2026) - first dedicated evidence
- FLOW trial (semaglutide in T2D + CKD): 24% reduction in kidney disease progression
Osteoarthritis and Musculoskeletal
- Retatrutide knee osteoarthritis trial (TRIUMPH program): Hypothesis that weight loss + possible direct anti-inflammatory effects of incretin agonism reduce joint disease
3.7 Critical Challenges and Unresolved Questions
1. Lean Mass Loss:
All GLP-1 RAs cause lean mass loss (~25% of total weight lost is muscle). This is particularly concerning in older adults at risk for sarcopenia. Ongoing research evaluates:
- Concurrent resistance training protocols
- Bimagrumab (anti-ActRII) as an adjunct to preserve/build muscle during weight loss
- Optimal protein intake during incretin therapy
- Mechanick et al., Obes Rev 2025 (PMID 39295512) provides specific strategies for minimizing muscle loss during incretin-mimetic drug use.
2. Weight Regain After Discontinuation:
Two-thirds of lost weight returns within 1 year of stopping medication. This fundamentally establishes that these are maintenance medications, not cures - analogous to antihypertensives for BP control.
3. Long-Term Safety:
- Thyroid C-cell tumors: Rodent signal with GLP-1 RAs (contraindicated in MEN2/medullary thyroid Ca history); human relevance unclear
- Pancreatitis: Small signal; caution in those with prior pancreatitis
- GI adverse events: Class effect - nausea, vomiting, diarrhea, constipation; usually transient; ~5-10% discontinuation rate
- Bone density effects: Under-studied, especially with profound weight loss
- Muscle quality (not just quantity): Adipose infiltration of muscle, fiber type changes - long-term functional implications unknown
4. Access, Equity, and Cost:
Injectable semaglutide/tirzepatide cost ~$800-1,300/month without insurance. Oral options (orforglipron, oral semaglutide) may dramatically improve access. Insurance coverage remains inconsistent globally. The 2025 systematic review by Kokkorakis et al. (PMID 39952695) specifically highlights "drug availability and cost-effectiveness assessments" as critical gaps.
5. "Quality" of Weight Loss:
As the 2026 ADA conference discussions noted - achieving 30% weight loss pharmacologically raises the question of whether all the cardiometabolic benefits of surgical weight loss (e.g., microvascular disease reduction, durable T2D remission) will translate. Early evidence is encouraging but not yet definitive.
6. Glycemic Control vs. Weight Loss Trade-offs:
Interestingly, despite retatrutide's superiority for weight loss over tirzepatide in indirect comparisons, the HbA1c reduction appears similar (~2%). A 2025 network meta-analysis suggests tirzepatide may optimize glycemic control more effectively while retatrutide maximizes weight reduction - implying different drugs for different primary goals.
3.8 Clinical Treatment Algorithm in 2026
The modern treatment algorithm, informed by ABCD staging:
STEP 1: Diagnose and Stage
├── Anthropometric: BMI + waist circumference + body composition
└── Clinical: Complication severity (CMD, biomechanical, psychosocial)
STEP 2: Lifestyle Therapy (ALWAYS as foundation)
├── Dietary: Caloric deficit, protein-adequate, Mediterranean/low-glycemic
├── Physical activity: 150-300 min/week moderate; resistance training (preserves muscle)
└── Behavioral: CBT, sleep optimization, stress management
STEP 3: Pharmacotherapy (based on BMI ≥30, or ≥27 + complication)
├── GLP-1 RA first line: Semaglutide 2.4 mg sc / tirzepatide 15 mg
├── Oral option: Orforglipron or oral semaglutide (access, preference)
└── Emerging (2026-27): CagriSema or retatrutide for highest-risk, highest BMI patients
STEP 4: Surgical/Procedural (BMI ≥40, or ≥35 + complications, or failed pharmacotherapy)
├── Roux-en-Y Gastric Bypass (RYGB)
├── Sleeve Gastrectomy
└── GLP-1 RA post-surgery for inadequate loss or recurrence
STEP 5: Combination (future)
└── Pharmacotherapy + bimagrumab (muscle preservation) + structured exercise
As the Sabiston Textbook of Surgery (7th edition) notes, incretin-mimetics are also being used as a bridge to surgery in very high BMI patients, and as adjuvant therapy in postoperative patients with inadequate weight loss (semaglutide: ~10% additional loss post-bariatric surgery).
Summary Table: Key 2025-2026 Agents at a Glance
| Agent | Class | Route | Approx. Weight Loss | Key Trial | Status (July 2026) |
|---|---|---|---|---|---|
| Semaglutide 2.4 mg | GLP-1 RA | sc weekly | ~15% | STEP 1-10, SELECT | Approved |
| Tirzepatide 15 mg | GLP-1+GIP | sc weekly | ~22.5% | SURMOUNT | Approved |
| Oral semaglutide 50 mg | GLP-1 RA | Oral daily | ~15% | OASIS | Near-approved |
| Orforglipron 36 mg | Small-mol GLP-1 RA | Oral daily | ~11.2% | ATTAIN-1 (NEJM 2025) | Phase 3 complete |
| CagriSema | GLP-1 + Amylin | sc weekly | ~20-23% | REDEFINE | Phase 3 complete; FDA submission Dec 2025 |
| Retatrutide | GLP-1+GIP+GCGR triple | sc weekly | ~20-30%+ | TRIUMPH (Phase 3) | Phase 3 ongoing; results ADA 2026 |
| Survodutide | GLP-1+GCGR | sc weekly | ~14.9% | Phase 3 complete (June 2026) | Pre-registration |
| Amycretin | GLP-1+Amylin (unimol.) | sc | ~13.1% (12 wks) | Phase 2 | Phase 3 ongoing |
| Ecnoglutide | Biased GLP-1 RA | sc | Significant | Phase 3 (Lancet 2025) | Phase 3 complete |
Conclusion
The field of obesity medicine in 2026 bears no resemblance to what it was a decade ago. Three conceptual revolutions are occurring simultaneously:
1. Disease recognition: Obesity has been re-established as a chronic neurobiological disease (ABCD) requiring long-term pharmacological management - not a willpower failure treatable with dietary advice alone.
2. Pharmacological efficacy: The weight losses achievable with retatrutide (>30%), CagriSema (~20-23%), and tirzepatide (~22.5%) are now overlapping with bariatric surgery outcomes - a threshold that fundamentally changes the risk-benefit calculus of medical vs. surgical management for many patients.
3. Organ-specific benefit: GLP-1 RA-based therapies are demonstrating proven benefits in cardiovascular disease, heart failure, OSA, MASH, CKD, and now potentially osteoarthritis - transforming obesity drugs into broad cardiometabolic disease-modifying agents.
As Dr. Holst summarized in his landmark 2024 Nature Metabolism review: "With normalisation of glycated haemoglobin levels and weight losses around 15-25%, therapeutic goals that were previously unrealistic are now within reach, and clinical trials have documented that these effects are associated with reduced risk of cardiovascular events and premature mortality."
The coming 12-24 months, with expected approvals of CagriSema, retatrutide, and oral GLP-1 options, will likely represent the most significant expansion of obesity pharmacotherapy in history.
Key Sources:
- Fuster and Hurst's The Heart, 15th Edition - Adiposity-Based Chronic Disease, p. 266-277
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Energy Balance Circuitry, p. 421-423
- Guyton and Hall Textbook of Medical Physiology - Obesity, GLP-1, Metabolic Adaptation, p. 875-878
- Sabiston Textbook of Surgery, 7th Edition - GLP-1 RAs in Surgical Practice
- Lippincott Illustrated Reviews: Pharmacology - Drugs for Obesity, p. 753-755
- Holst JJ, Nat Metab 2024 (PMID 39160334) - GLP-1 physiology and incretin drug development
- Kokkorakis et al., Pharmacol Rev 2025 (PMID 39952695) - Emerging pharmacotherapies for obesity: systematic review
- Karakasis et al., Metabolism 2025 (PMID 39719170) - Body composition network meta-analysis
- Wharton et al., NEJM 2025 (PMID 40960239) - Orforglipron Phase 3 (ATTAIN-1)
- Deanfield et al., Lancet 2024 (PMID 39181597) - SELECT trial HF sub-analysis
- Qin et al., Endocrine 2024 (PMID 38850440) - Tirzepatide systematic review + SURMOUNT-2
- Katsi et al., Biomolecules 2025 (PMID 40563436) - Retatrutide review
- ADA 2026 Scientific Sessions - Weintraub MD, Docwire News (July 6, 2026)
This is a shared conversation. Sign in to Orris to start your own chat.