Clinical presentation of glaucoma for ophthalmologist
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
Searching PubMed
glaucoma clinical features diagnosis optic nerve
I now have all the necessary information to write a comprehensive, clinician-level answer. Let me compile it.
Clinical Presentation of Glaucoma
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.
Definition
Glaucoma is a group of conditions sharing a common chronic progressive optic neuropathy, characterized by:
- Morphological changes at the optic nerve head (ONH) and retinal nerve fibre layer (RNFL)
- Progressive retinal ganglion cell (RGC) death via apoptosis
- Associated visual field loss
- IOP as the key modifiable risk factor
Glaucomatous RGC death occurs predominantly through apoptosis (not necrosis). The preterminal event is calcium ion influx and increased intracellular nitric oxide, followed by glutamate toxicity, astrocyte/glial proliferation, extracellular matrix alteration in the lamina cribrosa, and optic nerve head remodelling.
Classification Overview
| Type | Mechanism | Key Feature |
|---|---|---|
| Primary Open-Angle (POAG) | Trabecular outflow resistance | Silent, insidious, bilateral |
| Normal-Tension (NTG) | Vascular/mechanical, IOP ≤21 mmHg | Deeper disc cupping, paracentral fields |
| Primary Angle-Closure (PACG) | Pupillary block / iris apposition | Anatomically predisposed eye |
| Acute Angle-Closure | Sudden trabecular occlusion | Emergency with pain, red eye |
| Secondary Glaucomas | Identifiable cause | Varied presentation |
| Congenital/Developmental | Trabeculodysgenesis | Buphthalmos in infants |
1. Primary Open-Angle Glaucoma (POAG)
Epidemiology
- Most common type in European and African populations
- Prevalence ~6% in White and ~16% in Black populations over age 70
- Affects both genders equally
- POAG is 4x more common, develops earlier, and is harder to control in Black patients
Risk Factors
- IOP elevation - single most important; asymmetry ≥4 mmHg is significant
- Age (increases with each decade)
- Race (Black > White > Asian)
- Family history (4x risk in siblings, 2x in offspring)
- Myopia
- Low CCT (central corneal thickness)
- Low ocular perfusion pressure
- Large optic disc area
- Vascular disease (hypertension, cardiovascular disease, vasospasm)
- Systemic calcium-channel blockers (meta-analysis: higher glaucoma prevalence)
- Anti-VEGF therapy (repeated intravitreal injections - significant IOP risk, especially bevacizumab)
Symptoms
- Usually asymptomatic until advanced - the key clinical trap
- Visual symptoms are absent unless damage is advanced
- Occasionally, symptomatic central field defects occur early despite a relatively normal peripheral field
- Patients rarely notice peripheral field loss due to binocular overlap
- Discovery is typically incidental on routine eye exam
Signs on Examination
IOP:
- Elevated (>21 mmHg) in most cases, but not mandatory for diagnosis
- Diurnal variation is important - peak IOP may be missed on single measurement
Optic Disc Changes (the most critical examination finding):
| Feature | Description |
|---|---|
| Cup:Disc ratio (C:D) | Increased >0.6; asymmetry >0.2 between eyes is suspicious |
| Vertical elongation of cup | More specific for glaucoma than generalized enlargement |
| Inferior/superior notching | Loss of neuroretinal rim, worst infero-temporally (ISNT rule violation) |
| Rim thinning | Violates ISNT rule (Inferior > Superior > Nasal > Temporal normal order) |
| Disc haemorrhage | "Splinter" or "flame-shaped" haemorrhage on disc margin - strongly predictive of progression |
| Pallor | Disproportionate pallor compared to cup size |
| Bayonetting of vessels | Vessels disappear at the disc margin then reappear |
| Nasal shifting of vessels | Central retinal vessels displaced nasally |
| Laminar dot sign | Visualization of the fenestrations of the lamina cribrosa in a deep cup |
RNFL Changes:
- Diffuse or localised thinning, especially in arcuate bundles (superior and inferior)
- Best seen with red-free fundus photography or OCT
- Slit-lamp biomicroscopy under red-free illumination can show wedge-shaped defects
Visual Field Defects
Visual field defects correspond directly to patterns of RGC loss. Most important defects occur within the central 30° of fixation.
| Field Defect | Description |
|---|---|
| Baring of blind spot | Early change |
| Paracentral scotoma | Often first identifiable defect in arcuate area |
| Arcuate (Bjerrum) scotoma | Follows nerve fibre bundle path from blind spot to nasal horizontal raphe |
| Nasal step | Scotoma stops at horizontal midline - due to arcuate fibres respecting the horizontal raphe |
| Double arcuate scotoma | Ring scotoma from both superior and inferior arcuate defects |
| Advanced loss | Temporal island + central island - "tubular" vision |
| End-stage | Loss of central vision (late finding - patients may retain central fixation until very late) |
Automated perimetry (Humphrey 24-2 or 30-2) is the standard. The 10-2 pattern is used for central field monitoring in advanced disease with split fixation.
Gonioscopy
- Open angle (Grade 3-4 by Shaffer system)
- No peripheral anterior synechiae (PAS)
- Normal angle anatomy
2. Normal-Tension Glaucoma (NTG)
NTG (also: low-tension/normal-pressure glaucoma) is characterized by glaucomatous optic neuropathy with IOP consistently ≤21 mmHg. It accounts for 30-65% of open-angle glaucoma depending on ethnicity.
Distinct Clinical Features vs POAG
| Feature | NTG | POAG |
|---|---|---|
| IOP | ≤21 mmHg | Usually elevated |
| Optic disc | Larger, shallower cups; focal notches; more disc haemorrhages | More concentric cupping |
| Visual fields | More paracentral scotomas close to fixation; steeper edge; more superiorly located defects | Arcuate pattern |
| Age | Tends to be older at diagnosis | Younger |
| Race | More common in Japanese | Black > White |
| Gender | Slight female predominance | Equal |
| Vascular associations | Migraine, Raynaud phenomenon, nocturnal hypotension | Less common |
Risk Factors Specific to NTG
- Nocturnal blood pressure dips >20% (especially in those on antihypertensives)
- Abnormal vasoregulation (Raynaud, migraine)
- Obstructive sleep apnoea
- Autoantibodies
- Low CCT
- Larger translaminar pressure gradient
Differential Diagnosis for NTG
Must always exclude:
- Previous acute IOP elevation (old angle closure, steroid response)
- Intermittent IOP elevation (diurnal or postural)
- Low CCT falsely lowering applanation readings
- Non-glaucomatous optic neuropathies: anterior ischaemic optic neuropathy (AION), compressive lesions (pituitary, craniopharyngioma), Leber hereditary optic neuropathy, demyelination
3. Primary Angle-Closure Glaucoma (PACG)
Overview
PACG may account for up to half of all glaucoma globally and is especially prevalent in Asia. It progresses more rapidly and causes more visual loss than POAG.
Anatomical predispositions:
- Shallow anterior chamber
- Short axial length (hypermetropia)
- Thick, anteriorly positioned lens
- Narrow anterior chamber angle
- More common in females and older patients
Spectrum of Presentations
| Stage | Clinical Features |
|---|---|
| Primary angle-closure suspect | Narrow angle on gonioscopy; no ITC, no raised IOP, no disc/field damage |
| Primary angle-closure (PAC) | ITC in ≥3 quadrants; no glaucomatous optic neuropathy |
| PACG | ITC + glaucomatous optic nerve damage |
Acute Angle-Closure Attack - Classic Emergency Presentation
Symptoms:
- Sudden, severe unilateral ocular pain
- Frontal headache, nausea, vomiting (may mimic a GI or neurological emergency)
- Coloured halos around lights (corneal oedema causing prismatic effects)
- Sudden blurring of vision
- Occasionally abdominal pain
Signs:
- Markedly elevated IOP (may be 40-80 mmHg)
- Corneal epithelial oedema - diffuse cloudiness ("steamy" cornea)
- Ciliary injection (perilimbal flush)
- Semi-dilated, fixed pupil - mid-dilated, oval, non-reactive
- Shallow anterior chamber
- Closed angle on gonioscopy
- Decreased visual acuity
- Conjunctival injection
- Relative afferent pupillary defect (RAPD) may be present
Precipitating Factors:
- Dim illumination (pupil dilation)
- Emotional stress
- Mydriatic drugs
- Anticholinergic medications
- Prolonged reading (near work)
Sub-Acute / Intermittent Angle Closure
- Recurrent episodes of mild/moderate IOP elevation that spontaneously resolve
- Symptoms: transient blurring, halos, mild periorbital ache
- Resolves in bright light or on sleeping (miosis)
- Anterior chamber angle opens spontaneously
- Easy to miss - requires gonioscopy at time of symptoms or provocative testing
Chronic Angle Closure
- Insidious, similar to POAG
- Progressive PAS formation
- Gradual IOP elevation
- Glaucomatous disc and field changes
- Often asymptomatic
4. Congenital / Developmental Glaucoma
Primary Congenital Glaucoma (PCG) - trabeculodysgenesis:
| Sign | Description |
|---|---|
| Buphthalmos | Enlarged globe ("ox eye") due to raised IOP in a young, distensible sclera |
| Corneal enlargement | Horizontal corneal diameter >12 mm in newborns |
| Haab striae | Breaks in Descemet's membrane from corneal stretching - seen as curvilinear lines |
| Corneal oedema/cloudiness | Epithelial and stromal oedema |
| Photophobia | Often first symptom noticed by parents |
| Epiphora | Excessive tearing |
| Blepharospasm | Protective reflex |
| Optic cupping | May regress with IOP normalization in infants |
| Myopia | Progressive axial elongation |
5. Key Examination Framework for Glaucoma
Clinical Assessment Tools
IOP measurement:
- Goldmann applanation tonometry (gold standard)
- CCT must always be measured and used to interpret IOP (thin CCT underestimates; thick CCT overestimates)
Optic disc evaluation:
- Slit-lamp biomicroscopy with 78D/90D lens
- OCT of ONH and RNFL (quantitative, reproducible monitoring)
- Fundus photography for documentation and progression analysis
Gonioscopy:
Angle grading by Shaffer system:
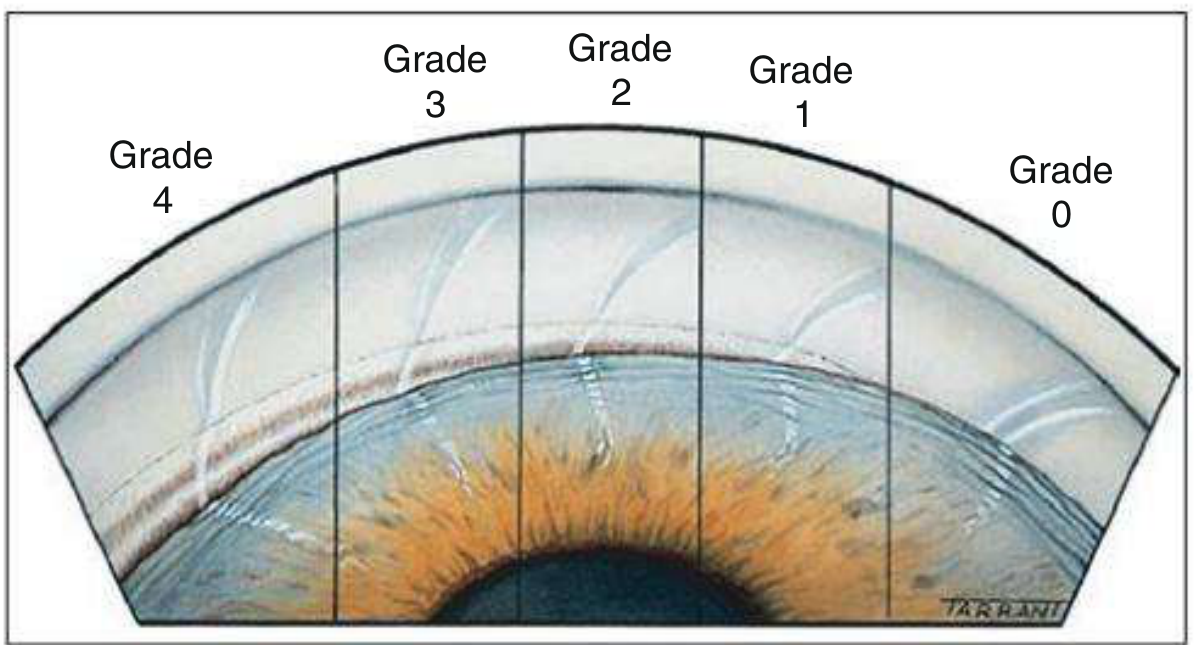
| Grade | Degrees | Angle Status |
|---|---|---|
| 4 | 35-45° | Wide open, ciliary body visible |
| 3 | 25-35° | Open, scleral spur visible |
| 2 | 20° | Trabeculum visible only, not scleral spur |
| 1 | 10° | Schwalbe line ± top of trabeculum only |
| 0 | 0° | Closed, iridocorneal contact |
Van Herick method (slit lamp only): peripheral AC depth as a fraction of corneal thickness - ratio <1/4 suggests dangerously narrow angle requiring urgent gonioscopy.
Visual field assessment:
- Standard automated perimetry (SAP): Humphrey 24-2 or 30-2 (standard)
- 10-2 for central field preservation monitoring in advanced disease
- GHT (Glaucoma Hemifield Test), MD, PSD, VFI as progression indices
6. Diagnostic Criteria Summary
POAG Diagnosis Requires:
- Characteristic glaucomatous optic neuropathy
- Corresponding visual field loss (when present)
- Open angle on gonioscopy
- No identifiable secondary cause
Note: Raised IOP alone is NOT required (NTG exists); raised IOP alone is NOT diagnostic (ocular hypertension without damage exists).
Pre-perimetric Glaucoma:
Structural changes on disc or RNFL (suspicious optic disc, RNFL defects on OCT) without detectable visual field loss on standard automated perimetry. Up to 50% of RGC may be lost before a field defect appears on SAP - hence structural assessment is paramount.
Key Pearls for the Ophthalmologist
- Glaucoma is primarily a structural diagnosis - disc and RNFL changes precede detectable field loss
- The "ISNT rule" violation (rim loss worst infero-temporally) is the earliest reliable clinical sign
- Disc haemorrhages are a powerful predictor of progression - flag them every visit
- Asymmetric cupping (C:D asymmetry >0.2) should trigger detailed glaucoma workup even when IOP is normal
- Acute angle closure mimics migraine, GI emergencies - keep a high index of suspicion for any patient with red eye + headache + nausea
- IOP is neither sufficient nor necessary for the diagnosis of glaucoma
- CCT is mandatory to interpret IOP correctly
Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Chapter 11 - Glaucoma
This is a shared conversation. Sign in to Orris to start your own chat.