Tell me about theory of endometriosis
Reading File
Finding Sources
Searching PubMed
endometriosis pathogenesis theory
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive textbook content from Robbins & Kumar and Bailey & Love. Here is the full answer:
Theory of Endometriosis
Endometriosis is defined as the presence of endometrial glands and stroma outside the uterus. It affects approximately 5-10% of women of reproductive age and nearly half of women with infertility. The exact pathogenesis remains elusive, but several well-established theories attempt to explain how ectopic endometrial tissue arises. These fall into two broad categories: theories proposing origin from uterine endometrium, and theories proposing origin from non-uterine cells.
The Four Major Theories
1. Regurgitation (Retrograde Menstruation) Theory
Most widely accepted - Sampson's Theory (1927)
This theory proposes that during menstruation, endometrial tissue flows retrograde through the fallopian tubes into the peritoneal cavity, where it implants on pelvic structures (ovaries, pouch of Douglas, uterosacral ligaments, fallopian tubes).
Supporting evidence:
- Retrograde menstruation occurs in up to 90% of women with patent tubes
- Lesions are most common in dependent pelvic sites (consistent with gravitational flow)
- Women with outflow obstruction (e.g., cervical stenosis) have higher rates of endometriosis
Limitation: Most women have retrograde menstruation, yet not all develop endometriosis - suggesting host immune factors and genetic susceptibility are also required for implants to survive.
2. Benign Metastasis Theory (Vascular/Lymphatic Dissemination)
This theory holds that endometrial tissue can "spread" from the uterus to distant sites - including bone, lung, brain, and umbilicus - via blood vessels and lymphatic channels, analogous to the spread of cancer cells.
Supporting evidence:
- Endometriosis has been documented in the lungs (causing catamenial haemoptysis and recurrent pneumothorax), brain, and even men on estrogen therapy
- Bailey & Love notes "distant sites such as the lungs are occasionally affected, resulting in symptoms such as recurrent haemoptysis at the time of menstruation or recurrent pneumothoraces"
3. Coelomic Metaplasia Theory
This theory proposes that the coelomic epithelium (mesothelium lining the pelvic/abdominal cavity) undergoes metaplastic transformation into endometrial tissue. This is biologically plausible because both the peritoneal mesothelium and the Mullerian ducts (which give rise to the uterus and endometrium) share a common embryological origin - the coelomic epithelium.
Additionally, mesonephric (Wolffian) remnants may also undergo endometrial differentiation and give rise to ectopic foci.
Supporting evidence:
- Explains endometriosis in sites unreachable by retrograde flow (e.g., pleura, pericardium)
- Explains rare cases in men and prepubertal girls
- Explains the distribution of lesions along embryological lines
4. Extrauterine Stem/Progenitor Cell Theory
This newer theory proposes that bone marrow-derived stem cells or circulating progenitor cells can home to ectopic sites and differentiate into functional endometrial tissue under the influence of hormonal signals (primarily estrogen).
Supporting evidence:
- Bone marrow transplant studies in animal models have shown donor-derived endometrial cells at ectopic sites
- Explains endometriosis in rare anatomical locations
- Supported by findings of endometrial tissue in patients with Mayer-Rokitansky-Kuster-Hauser (MRKH) syndrome who have no uterus - a 2025 systematic review (Vercellini et al., Hum Reprod, PMID 40246293) found a small but real prevalence of endometriosis in MRKH variants, lending support to non-uterine origins
Molecular Mechanisms Sustaining Implants
Once established (by whatever route), endometriotic implants are not simply misplaced endometrium - they have distinct biological characteristics that allow them to survive and grow:
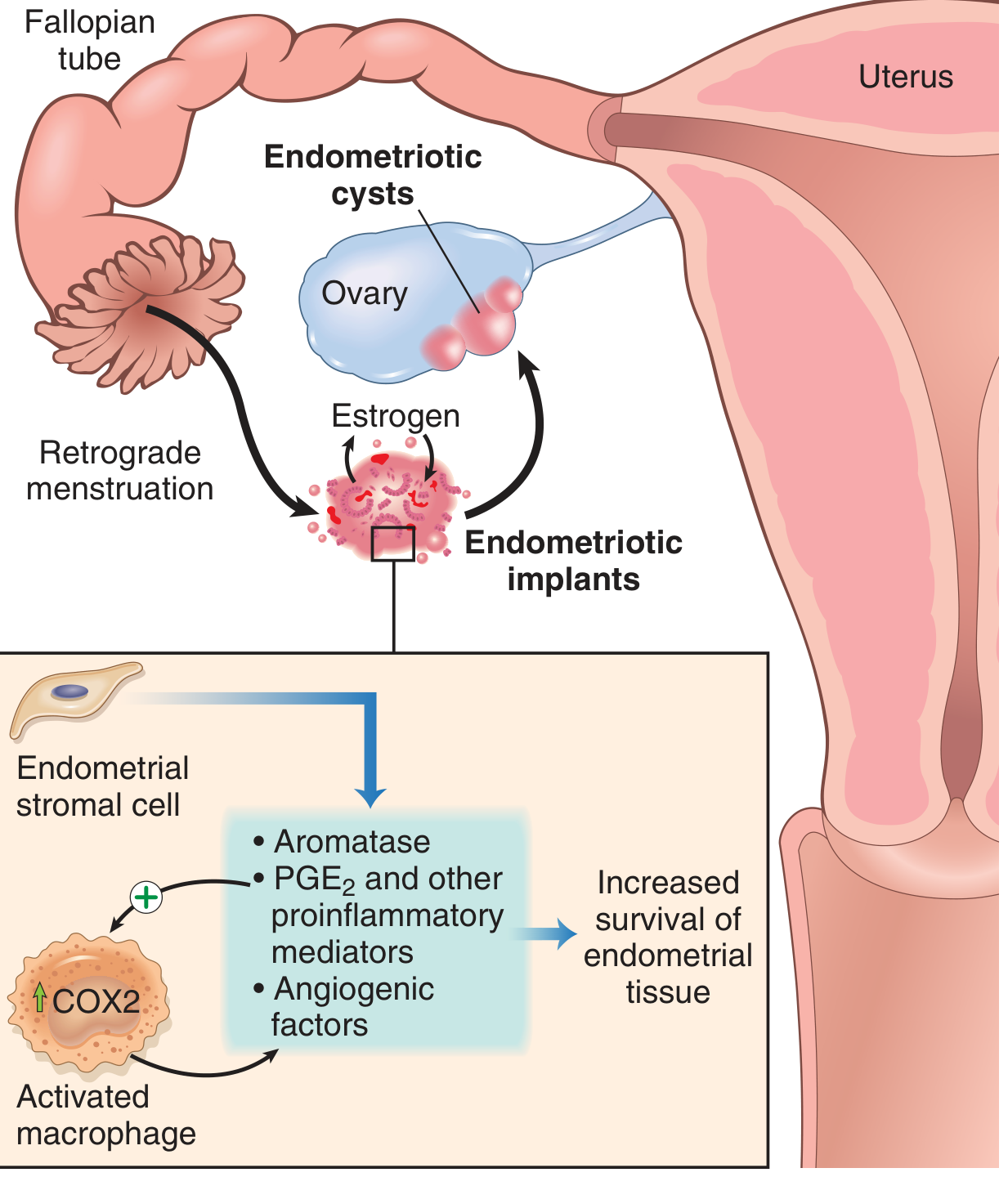
Fig. 17.9 from Robbins & Kumar Basic Pathology - Pathogenesis of endometriosis. COX2 = Cyclooxygenase 2; PGE2 = Prostaglandin E2
| Mediator | Role |
|---|---|
| Aromatase | Overexpressed in stromal cells; converts androgens to estrogen locally, creating an estrogen-rich microenvironment that sustains growth |
| PGE2 (Prostaglandin E2) | Proinflammatory; stimulates aromatase in a positive feedback loop; induces pain |
| VEGF | Promotes angiogenesis, allowing implants to develop a blood supply |
| Matrix Metalloproteinases (MMPs) | Break down extracellular matrix; facilitate invasion and implantation |
| Activated Macrophages | Recruited to implants; upregulate COX2, release further inflammatory mediators, perpetuating the cycle |
| TGF-β superfamily | A 2025 systematic review (Xu et al., Front Immunol, PMID 40873582) highlights TGF-β as a key driver of immune evasion, fibrosis, and implant survival |
The net result is a self-sustaining pro-inflammatory, pro-estrogenic, pro-angiogenic microenvironment that allows implants to evade immune clearance and persist.
Types of Endometriosis
Three distinct subtypes are recognized (Robbins & Kumar):
| Type | Description |
|---|---|
| Superficial peritoneal endometriosis | Small implants on peritoneal surfaces; appear as "powder burn" / "gunshot" black-brown lesions or subtle red/clear vesicles |
| Ovarian endometriosis (endometrioma) | Cystic ovarian masses (3-5 cm) filled with dark "chocolate" fluid (old haemorrhage); "chocolate cysts" |
| Deep infiltrating endometriosis (DIE) | Tissue >5 mm below peritoneal surface; involves uterosacral ligaments, vagina, bowel, bladder, ureters. Highest risk of malignant transformation |
Why Not Everyone With Retrograde Menstruation Develops Endometriosis?
This is the central unsolved question. Current thinking points to:
- Immune dysfunction - impaired peritoneal NK cell and T-cell clearance of ectopic cells
- Genetic susceptibility - polygenic predisposition affecting implantation, immune response, and steroid metabolism
- Epigenetic changes - aberrant methylation of progesterone receptor and HOXA genes in endometriotic cells, causing progesterone resistance
- Volume/composition of retrograde flow - more reflux, longer menstrual cycles, and obstructed outflow increase risk
Sources:
- Robbins & Kumar Basic Pathology, p. 689 (pathogenesis and molecular mechanisms)
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1603 (clinical features and subtypes)
- Recent evidence: TGF-β role in endometriosis - Xu et al. 2025, Front Immunol | Endometriosis in MRKH - Vercellini et al. 2025, Hum Reprod
This is a shared conversation. Sign in to Orris to start your own chat.