Detailed information about total abdominal hysterectomy, its clinically important points and detaled procedure for neet pg resident
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Searching the Web
total abdominal hysterectomy steps complications NEET PG surgery clinical points
I now have comprehensive content from Sabiston Textbook of Surgery, Berek & Novak's Gynecology, and supporting web sources. Let me compile the complete, detailed answer.
Total Abdominal Hysterectomy (TAH) - Complete Guide for NEET PG Residents
Sources: Sabiston Textbook of Surgery, Berek & Novak's Gynecology
Definition
A Total Abdominal Hysterectomy (TAH) is the surgical removal of both the uterine corpus AND the cervix through an abdominal incision. It is distinguished from:
- Subtotal/Supracervical hysterectomy - uterine corpus removed, cervix left in situ
- TAH + BSO - total hysterectomy with bilateral salpingo-oophorectomy
- Radical hysterectomy (Wertheim's) - removes uterus, cervix, upper vagina, parametria, and pelvic lymph nodes
Indications (Clinically Important for NEET PG)
| Category | Specific Conditions |
|---|---|
| Benign | Symptomatic uterine leiomyomas (fibroids), adenomyosis, DUB/menorrhagia not responding to medical therapy, uterine prolapse, chronic pelvic pain (with documented pathology) |
| Pre-malignant | Recurrent high-grade CIN (after failed conservative treatment), microinvasive cervical carcinoma |
| Malignant | Endometrial cancer, cervical cancer (early stage), uterine sarcoma/leiomyosarcoma |
| Obstetric emergencies | Intractable PPH (Caesarean hysterectomy), uterine rupture, placenta accreta/increta/percreta |
| Others | Endometriosis (requiring BSO), pelvic inflammatory disease with tubo-ovarian abscess |
NEET PG Key Point: Hysterectomy is the treatment of last resort for CIN. It is only done when: (1) microinvasion is confirmed, (2) there is histologically confirmed recurrent high-grade CIN after LLETZ/conization, or (3) coexisting gynecologic pathology requiring hysterectomy (fibroids, prolapse). - Berek & Novak's Gynecology
Types of Hysterectomy - Classification (Exam Favorite)
By extent of removal:
- Total hysterectomy - uterus + cervix
- Subtotal/Supracercival hysterectomy - uterus only (cervix preserved)
- Radical hysterectomy (Wertheim's/Type III) - uterus + cervix + upper 1/3 vagina + parametria + pelvic LN
- TAH + BSO - adds bilateral salpingo-oophorectomy
By route:
- Abdominal (TAH) - open
- Vaginal (VH)
- Laparoscopically-assisted vaginal hysterectomy (LAVH)
- Total laparoscopic hysterectomy (TLH)
- Robotic-assisted hysterectomy
NEET PG Key Point: ACOG recommends preferring vaginal or laparoscopic route over abdominal when feasible (less morbidity, shorter hospital stay). TAH is chosen when: large uterus, expected extensive adhesions, need for concurrent abdominal surgery, or surgeon/patient preference.
Preoperative Workup
- Complete history and examination, Pap smear, endometrial biopsy if indicated
- Pelvic USG (assess uterine size, adnexa)
- CBC, coagulation profile, renal/liver function, urine routine
- Group and crossmatch blood (2 units)
- Informed consent - including permanent sterility, menopause if BSO, bowel/bladder injury risk
- Bowel preparation (usually mechanical bowel prep night before)
- DVT prophylaxis: TED stockings + LMWH
- Antibiotic prophylaxis: single dose IV cefazolin 1g (or metronidazole + gentamicin) at induction
- Foley catheterization before incision
- Patient positioning: supine, Trendelenburg
Anesthesia
- General endotracheal anesthesia (preferred for abdominal approach)
- Combined spinal-epidural (CSE) can be used
- Epidural catheter (T8-T11 level for TAH) for postoperative pain management
Surgical Anatomy - Clinically Critical
Before performing TAH, the resident must have a thorough understanding of:
| Structure | Relevance |
|---|---|
| Ureter | Most commonly injured pelvic structure (0.5-1%). Crosses under the uterine artery at the level of the internal os ("water passes under the bridge"). Identify BEFORE ligating uterine vessels |
| Uterine artery | Branch of internal iliac artery; runs in the base of the broad ligament; ligated at the level of internal os |
| Infundibulopelvic (IP) ligament | Contains ovarian artery and vein; ligated when doing oophorectomy; ureter runs just below/medial to it |
| Broad ligament | Peritoneal fold containing fallopian tube (in upper margin), round ligament (anteriorly), ovarian ligament, uterine vessels, and ureter |
| Cardinal ligament (Mackenrodt's) | Main support of uterus; connects cervix to pelvic sidewall; ligated in serial steps |
| Uterosacral ligaments | Posterior support from cervix to sacrum; incorporated in vaginal cuff closure for apical support |
| Bladder | Anteriorly placed; must be dissected off the lower uterine segment before ligating uterine vessels |
Step-by-Step Procedure (TAH)
Incision
An abdominal incision is made either as:
- Pfannenstiel (low transverse) - preferred cosmetically, used for benign disease, smaller uteri
- Vertical midline subumbilical - used for malignancy, large uteri, anticipated adhesions, need for lymph node dissection
Step 1 - Enter Abdomen and Exploration
Open abdomen in layers: skin → subcutaneous fat → anterior rectus sheath → rectus muscles separated → posterior sheath/peritoneum entered. Explore the abdomen - note uterine size, adnexa, adhesions, bowel. Place a self-retaining retractor (Balfour or O'Connor-O'Sullivan). Pack bowel superiorly with moist packs. Place patient in Trendelenburg.
Step 2 - Round Ligament Division
The uterus is grasped with a heavy clamp (Kocher or Bonney) and elevated. The round ligaments are identified on each side, grasped laterally with a clamp, and divided between clamps either with electrocautery or by ligating with a delayed absorbable suture (0-Vicryl) then dividing medial to the suture.
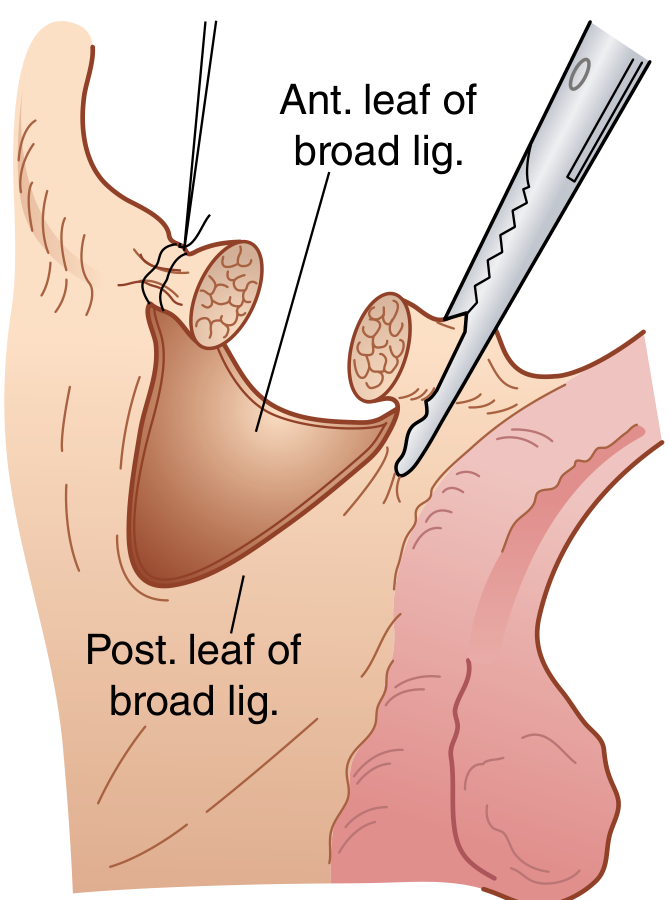
Step 3 - Broad Ligament Incision and Bladder Flap
The anterior leaf of the broad ligament is incised medially toward the internal cervical os. This facilitates development of the bladder flap - separating the bladder from the lower uterine segment and allowing it to retract inferiorly. This is a critical step to avoid bladder injury during subsequent steps.
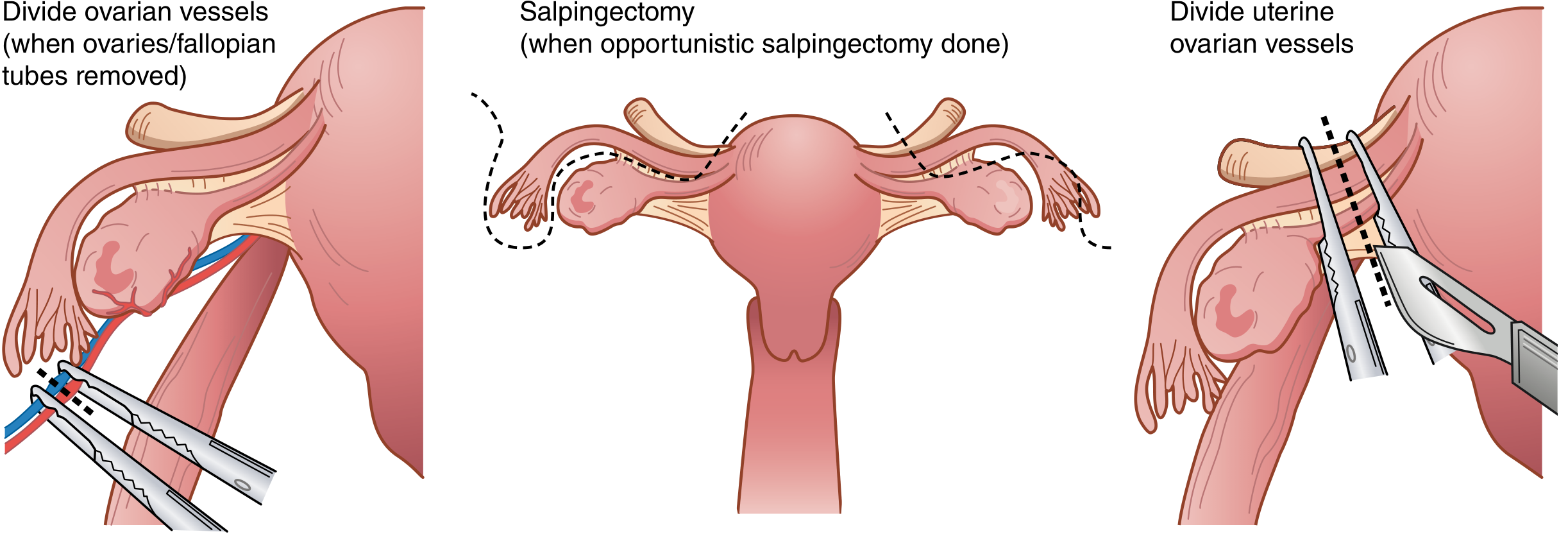
Step 4 - Adnexal Management (Decision Point)
If ovaries and tubes are to be REMOVED (oophorectomy):
- Incise posterior leaves of broad ligament on each side
- Identify the ureter by palpation/visualization through the peritoneum (it lies medial and posterior to the IP ligament)
- Doubly clamp the infundibulopelvic (IP) ligament with curved Heaney or Zeppelin clamps
- Divide between clamps with curved Mayo scissors
- Doubly ligate remaining pedicles with 0-Vicryl (specimen side ligated to prevent back-bleeding)
If ovaries are to be PRESERVED (opportunistic salpingectomy only or conservation):
- Two curved Kelly or Heaney clamps placed across the utero-ovarian ligament (ovarian ligament + proximal fallopian tube)
- Divide and doubly ligate
- Salpingectomy can be performed along the mesosalpinx
NEET PG Key Point: The ureter must be identified BEFORE clamping the IP ligament. The ureter crosses the common iliac artery at the pelvic brim, then runs along the medial leaf of the broad ligament, and passes under the uterine artery at the level of the internal os ("water under the bridge").
Step 5 - Uterine Vessel Ligation (Critical Step)
- Remaining leaves of posterior broad ligament are incised inferiorly to skeletonize the uterine vessels as they travel along the lateral edge of the uterus
- A curved Heaney or Zeppelin clamp is placed across the uterine vessels perpendicular to the uterus at the level of the internal cervical os
- The pedicle is cut and suture ligated (transfixion stitch with 0-Vicryl)
- The ureter should be identified again at this point as it lies just medial and inferior to where the clamp is placed
NEET PG Key Point: This is the most common step where ureteric injury occurs. The ureter at this point is only about 1-2 cm from the uterine vessels. Always dissect the bladder flap fully and identify the ureter before clamping.
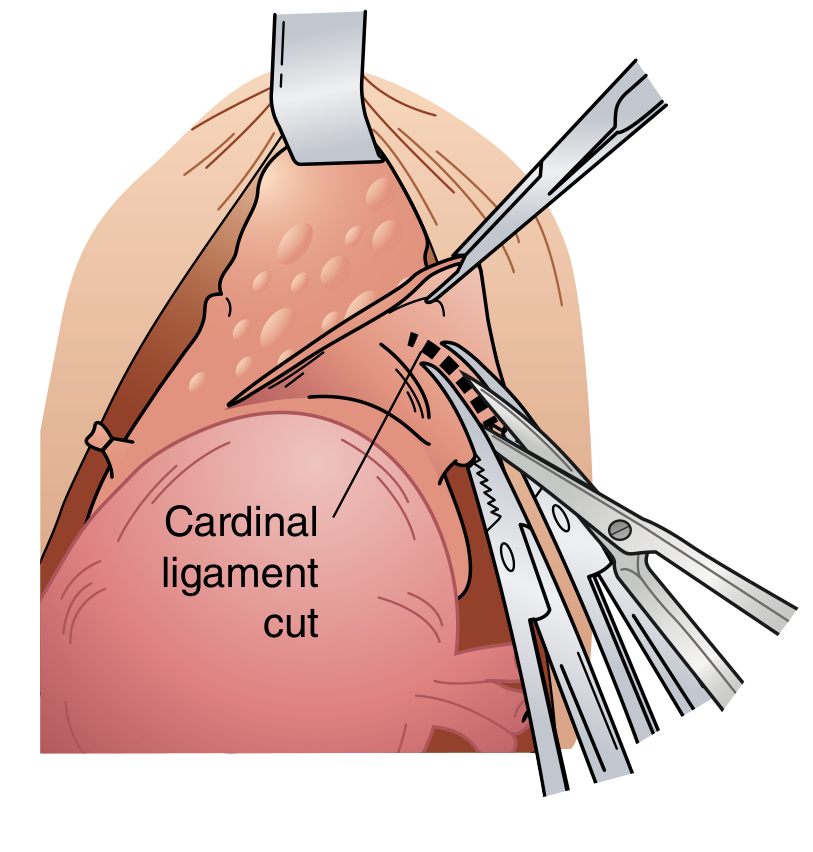
Step 6 - Cardinal and Uterosacral Ligament Division
- Bladder is further dissected completely below the level of the cervix
- A straight Heaney or Zeppelin clamp is placed serially on the cardinal ligaments and uterosacral ligaments bilaterally, in a stepwise fashion, working downward
- Each pedicle is cut and suture ligated
- Continue until both sides are clear of tissue at the level of the external cervical os
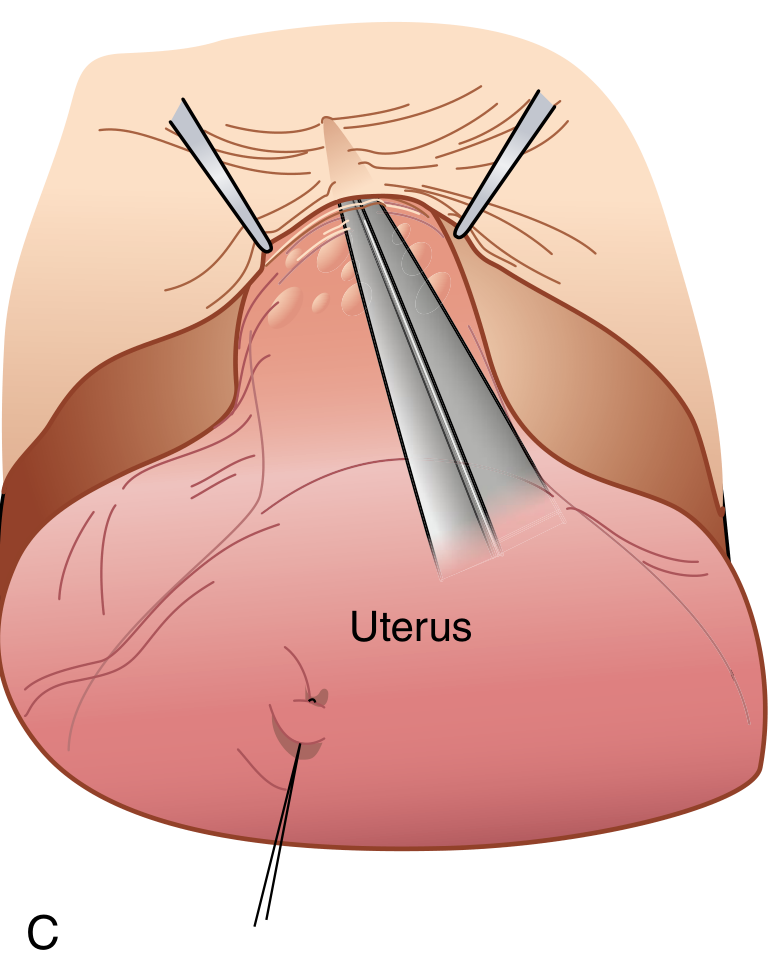
Step 7 - Colpotomy and Specimen Excision
Method 1 (Clamp technique): Curved clamps are placed across the vagina medial to the prior pedicles, just below the cervix, meeting in the midline. Curved scissors cut just above the clamps separating the uterus and cervix from the vagina.
Method 2 (Direct incision): A direct sharp incision is made into the vagina just below the cervix, extended around the cervix with curved scissors until the cervix is completely freed and the specimen removed.
- Edges of upper vagina grasped with Allis clamps for visualization
- The uterus and cervix are sent as a single specimen for histopathology
Step 8 - Vaginal Cuff Closure
- Heaney transfixion stitches placed beneath the two angle clamps to ligate vaginal corners
- Vaginal cuff closed with interrupted figure-of-eight sutures or running suture
- The lateral apex sutures incorporate the ipsilateral uterosacral ligament - this provides apical support and prevents future vaginal vault prolapse
- An alternative: running suture, interrupted sutures, or figure-of-eight sutures
Step 9 - Hemostasis Check and Closure
- Inspect all pedicles for hemostasis
- Irrigate pelvis with warm saline
- Count instruments, needles, and swabs (mandatory)
- Peritoneum may be left open (current evidence shows no benefit to closing parietal peritoneum)
- Anterior rectus sheath closed with loop PDS or 1-Vicryl
- Skin closed with subcuticular suture or staples
Clinically Important Points for NEET PG
Ureter Injuries (Most Exam-Important Complication)
- Incidence: 0.5-1% of TAH
- Most common site of injury: At the level of the uterine artery (where ureter passes under the uterine artery - "water under the bridge")
- Second most common site: As ureter enters bladder trigone / near IP ligament
- Types: Ligation, kinking, transection, thermal injury
- Timing of detection: 75% detected intraoperatively (give IV methylene blue or indigo carmine and check for spillage); 25% postoperatively (flank pain, fever, urinary fistula)
- Prevention: Always identify ureters bilaterally before each clamping step
Other Intraoperative Complications
| Complication | Details |
|---|---|
| Bladder injury | Most common visceral injury (~1-2%); occurs during bladder flap creation; recognized by seeing catheter/urine; repair in 2 layers |
| Bowel injury | Less common; usually small bowel or sigmoid; always palpate bowel pre/post dissection |
| Hemorrhage | Primary source: uterine artery pedicle slipping; treat with pressure, re-clamp, suture |
Postoperative Complications
| Early (<48 hours) | Late (>48 hours) |
|---|---|
| Hemorrhage (reactionary) | Wound infection |
| DVT/PE | Vault hematoma |
| Ileus | Vaginal vault dehiscence |
| Urinary retention | Ureterovaginal fistula (10-21 days post-op) |
| Atelectasis/pneumonia | Vesicovaginal fistula (VVF) |
| Bowel obstruction (adhesions) | |
| Vault granulations | |
| Ovarian remnant syndrome (if BSO) |
NEET PG Key Point on Fistulas: VVF (vesico-vaginal fistula) after TAH typically presents 10-21 days postoperatively with continuous painless leakage of urine per vaginum. Ureterovaginal fistula presents similarly. 3-dye test or cystoscopy can differentiate. The "3-swab test" with oral phenazopyridine + intravesical methylene blue helps localize the fistula level.
Menopause After Hysterectomy
- TAH alone (ovaries preserved): no menopause; ovaries continue functioning
- TAH + BSO: immediate surgical menopause; HRT should be discussed for women <50 years
- Ovaries conserved in TAH may fail earlier due to disruption of blood supply (ovarian blood supply partly from uterine artery via utero-ovarian anastomosis)
Opportunistic Salpingectomy
- Strongly recommended at time of hysterectomy when ovaries are conserved
- Evidence shows most "ovarian" high-grade serous carcinomas actually originate in the fallopian tube (fimbrial end)
- Salpingectomy at TAH reduces lifetime risk of ovarian cancer without increasing surgical morbidity
Route Selection (TAH vs VH vs TLH)
| Factor | Favors TAH | Favors VH | Favors TLH |
|---|---|---|---|
| Uterine size | Very large (>16 weeks) | Small/normal | Small to moderate |
| Adhesions | Extensive adhesions | Minimal | Mild-moderate |
| Malignancy | Staging required | Generally avoided | Selected cases |
| Prolapse | Not indicated | Ideal | Less ideal |
| Access | Limited vaginal access | Good descent | Any |
| Morbidity | Higher | Lowest | Low |
Contraindications to TAH (or favoring other routes)
- Significant uterovaginal prolapse (vaginal route preferred)
- Patient desires fertility preservation (consider myomectomy instead)
- Very small uterus with good vaginal access (vaginal or laparoscopic preferred)
Key Sutures and Instruments Used
| Step | Clamp/Instrument | Suture |
|---|---|---|
| Round ligament | Kocher/Mayo clamp | 0-Vicryl delayed absorbable |
| IP ligament (ovarian vessels) | Curved Heaney/Zeppelin | 0-Vicryl (double ligature) |
| Uterine vessels | Curved Heaney | 0-Vicryl transfixion |
| Cardinal/uterosacral | Straight Heaney | 0-Vicryl |
| Vaginal cuff | Allis clamps (traction) | 0-Vicryl interrupted/running |
| Fascia closure | - | Loop PDS/1-Vicryl |
High-Yield NEET PG Summary Points
- TAH = uterine corpus + cervix removed (vs subtotal = corpus only)
- Most common injury in TAH = ureter (passes under uterine artery at internal os)
- Second most common = bladder (during bladder flap creation)
- VVF after TAH presents at 10-21 days postoperatively
- Round ligament is the FIRST structure divided in TAH
- Bladder flap must be fully developed before ligating uterine vessels
- Uterine artery ligated at level of internal os - always identify ureter first
- Cardinal ligament = Mackenrodt's ligament - main uterine support
- Uterosacral ligaments incorporated in vaginal cuff closure for apical support
- TAH + BSO → immediate surgical menopause (discuss HRT for women <50 years)
- Opportunistic salpingectomy recommended when conserving ovaries (reduces ovarian cancer risk)
- Anesthesia level for TAH: T8-T11 (epidural) - as per Miller's Anesthesia
- Antibiotic prophylaxis: Single dose cefazolin at induction
- DVT prophylaxis: Mandatory (LMWH + TED stockings)
- IP ligament contains ovarian artery and vein - ureter runs medial/below it
References: Sabiston Textbook of Surgery (The Biological Basis of Modern Surgical Practice), pp. 2799-2800; Berek & Novak's Gynecology; Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.