MAC and and everything I need to know as a Anesthesiology resident.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-structured MAC reference. Let me compile the full answer.
MAC (Minimum Alveolar Concentration) - Complete Anesthesiology Resident Reference
1. Definition
MAC is the alveolar concentration of an inhaled anesthetic (expressed as % of 1 atmosphere) that prevents movement in 50% of patients in response to a standardized noxious stimulus (classically, a surgical skin incision).
- It is the ED50 (median effective dose) for the immobility endpoint
- It reflects brain partial pressure at steady state, since alveolar and brain partial pressures equilibrate
- It allows potency comparisons between agents
- It is a population median - has limited utility in managing individual patients, especially during rapidly changing concentrations (induction/emergence)
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 294
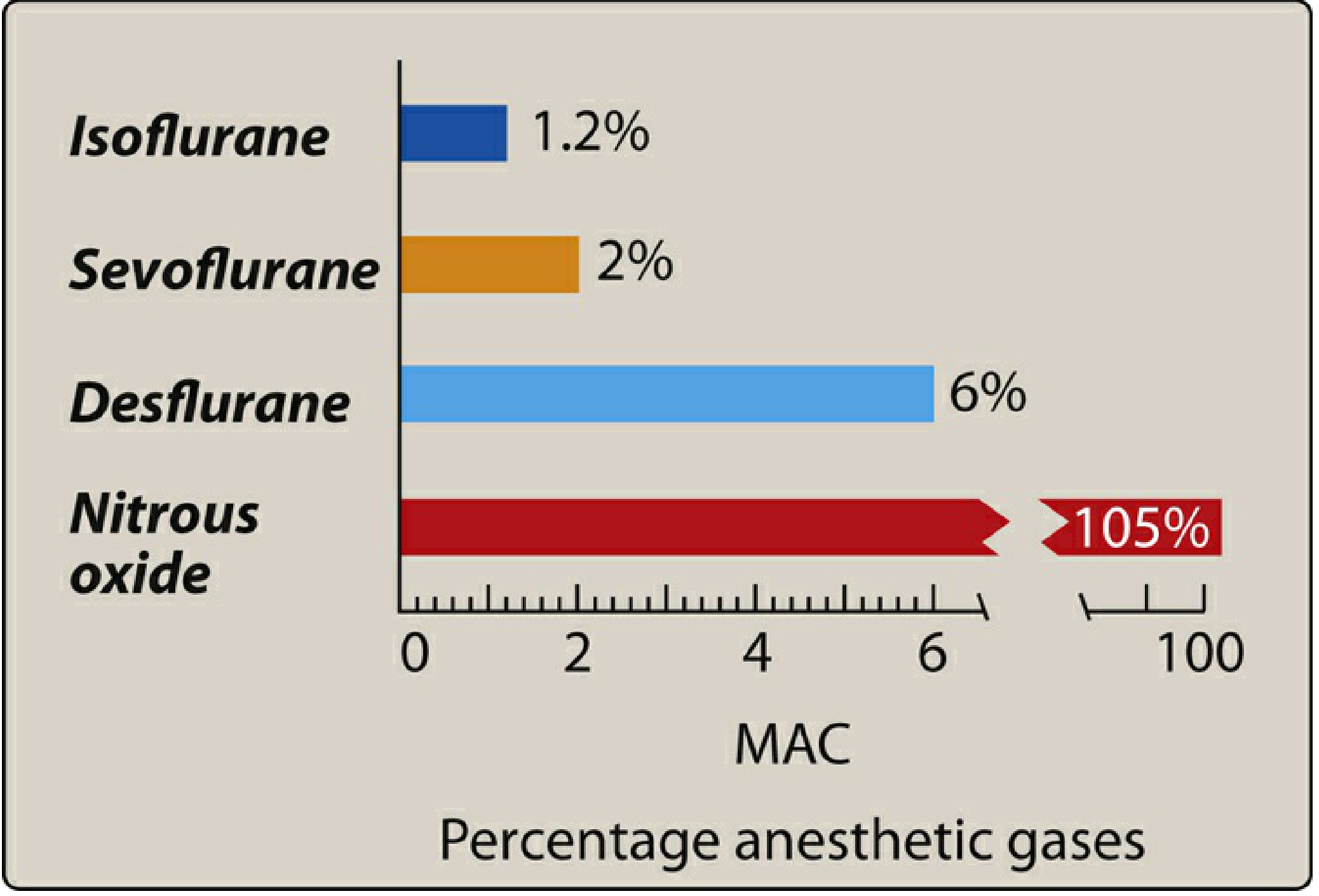
2. MAC Values for Common Agents
| Agent | MAC (%) | Vapor Pressure (mmHg at 20°C) | Blood/Gas Partition Coeff. |
|---|---|---|---|
| Nitrous oxide (N₂O) | 105 | - (gas) | 0.47 |
| Halothane | 0.75 | 243 | 2.4 |
| Isoflurane | 1.2 | 240 | 1.4 |
| Sevoflurane | 2.0 | 160 | 0.65 |
| Desflurane | 6.0 | 681 | 0.42 |
- Nitrous oxide's MAC >100% means it cannot produce surgical anesthesia alone at normobaric conditions (any N₂O:O₂ mixture that allows survival cannot reach 105%)
- High MAC = low potency (more drug needed); Low MAC = high potency
- The inverse of MAC is an index of potency
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 294-295; Lippincott Pharmacology, p. 668
3. Key MAC Multiples (Clinically Critical)
| Multiple | Clinical Meaning |
|---|---|
| 0.3-0.4 MAC | MAC-awake: 50% of patients open eyes on command (emergence) |
| 1.0 MAC | 50% of patients don't move at skin incision (ED50) |
| 1.3 MAC | ~95% of patients don't move (approximates ED95) |
| 1.5 MAC | Hemodynamic suppression becomes clinically significant |
MAC-BAR (block adrenergic response): ~1.5-1.7 MAC - the concentration that blunts autonomic responses (tachycardia, hypertension) to surgical stimulation in 50% of patients. Higher than standard MAC.
4. MAC Additivity
MAC values from different agents are additive:
0.5 MAC N₂O + 0.5 MAC isoflurane = 1.0 MAC equivalent effect on immobility
Important caveat: Myocardial depression is NOT equivalent at the same MAC across agents. For example, 0.5 MAC halothane causes significantly more myocardial depression than 0.5 MAC N₂O, even though both have the same immobility effect.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 295
5. Factors That Modify MAC
Increase MAC (patient more resistant - need more drug)
| Factor | Notes |
|---|---|
| Young age | Infants have highest MAC; decreases ~6% per decade |
| Hyperthermia | Above normal; decreases if >42°C |
| Chronic alcohol abuse | CNS tolerance (chronic ethanol ↑ MAC; acute intoxication ↓ MAC) |
| Hypernatremia | Via CSF osmolality changes |
| Sympathomimetics (acute) | e.g., cocaine, ephedrine - increase CNS catecholamines |
| Chronic opioid use | Via opioid tolerance |
Decrease MAC (patient more sensitive - need less drug)
| Factor | Notes |
|---|---|
| Increasing age | Elderly patients need significantly less |
| Hypothermia | Each 1°C drop reduces MAC ~5% |
| Pregnancy | ↓ by one-third at 8 weeks' gestation; normalizes by 72h postpartum |
| Sepsis / critical illness | |
| Acute alcohol intoxication | |
| Severe hypotension | MAP <40 mmHg |
| Severe anemia | Hematocrit <10% |
| Hypoxia | PaO₂ <40 mmHg |
| Severe hypercarbia | PaCO₂ >95 mmHg (via CSF pH) |
| Hyponatremia | |
| Hypercalcemia | |
| IV anesthetics | Opioids, propofol, ketamine, benzodiazepines, barbiturates |
| Alpha-2 agonists | Clonidine, dexmedetomidine (significant MAC-sparing effect) |
| Local anesthetics | Except cocaine |
| Verapamil, lithium |
Does NOT affect MAC
- Thyroid disease (hyper or hypothyroid)
- Sex
- Duration of anesthesia
- Hyper/hypokalemia
- PaCO₂ in the normal range
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Table 8-4, p. 296; Lippincott Pharmacology, p. 668
6. Meyer-Overton Correlation (Basis of MAC / Potency)
MAC correlates inversely with lipid solubility (oil/gas partition coefficient). More lipid-soluble agents partition into CNS membranes more avidly → lower concentration needed → lower MAC → higher potency.
- This is the Meyer-Overton rule: anesthetic potency correlates with lipid solubility
- Likely mechanism: anesthetics dissolve into hydrophobic domains of ligand-gated ion channels, particularly GABA-A receptors (enhanced) and NMDA receptors (inhibited)
- Glycine receptor α1-subunit and nicotinic ACh receptors are also implicated
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 290-291
7. Partition Coefficients (Critical for Understanding Kinetics)
| Agent | Blood/Gas | Brain/Blood | Muscle/Blood | Fat/Blood |
|---|---|---|---|---|
| Nitrous oxide | 0.47 | 1.1 | 1.2 | 2.3 |
| Halothane | 2.4 | 2.9 | 3.5 | 60 |
| Isoflurane | 1.4 | 2.6 | 4.0 | 45 |
| Desflurane | 0.42 | 1.3 | 2.0 | 27 |
| Sevoflurane | 0.65 | 1.7 | 3.1 | 48 |
Key principle: Low blood/gas coefficient = faster induction and emergence (less uptake into blood, faster rise of alveolar partial pressure toward inspired concentration). Desflurane and N₂O have the fastest kinetics; halothane the slowest.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Table 8-1, p. 281
8. Factors Affecting Uptake (FA/FI Rise)
The speed at which alveolar concentration (FA) approaches inspired concentration (FI) determines induction speed:
- Solubility in blood - Low blood/gas coefficient → FA/FI rises fast (desflurane, N₂O)
- Cardiac output - High CO → more uptake → slows FA/FI rise → slows induction. Low CO states (e.g., heart failure, shock) → rapid rise → risk of overdose with soluble agents
- Alveolar-venous partial pressure gradient - Tissue uptake drives this; larger gradient = more uptake = slower FA rise
- Alveolar ventilation - Higher MV accelerates FA/FI equilibration (more so for soluble agents)
- Functional residual capacity (FRC) - Larger FRC → slower washout and wash-in (more volume to fill)
Overpressure strategy: Giving a higher inspired concentration than target MAC initially speeds induction by overcoming uptake, but raises the risk of overdose - monitor carefully.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 281-282; Lippincott Pharmacology, p. 669
9. Levels of Sedation Context
MAC sits within the broader continuum of CNS depression:
| Level | Mentation | Airway | Cardiovascular |
|---|---|---|---|
| Minimal (anxiolysis) | Responds normally to verbal | Unaffected | Unaffected |
| Moderate sedation | Responds purposefully to verbal/tactile | Adequate | Usually maintained |
| Deep sedation | Responds to repeated verbal or pain | May need intervention | Usually maintained |
| General anesthesia (1 MAC) | Unarousable to pain | Usually requires intervention | May be impaired |
- Lippincott Pharmacology, Figure 20.3, p. 665
10. Practical Clinical Pearls for the OR
- At induction: FA is far below target MAC; use overpressure and IV co-induction agents (propofol, opioids) to reach effective depth fast
- At 0.5 MAC: N₂O + 0.5 MAC volatile is a common and effective combination
- MAC-awake (0.3-0.4): Patients may move, open eyes, but are still at risk for awareness if this is the sole agent
- MAC-BAR (~1.5): Needed to blunt sympathetic responses in high-stimulus moments (laryngoscopy, sternotomy)
- Age adjustment: A 70-year-old needs roughly 20-25% less volatile anesthetic than a 40-year-old
- Dexmedetomidine: Provides significant MAC reduction (useful opioid/volatile sparing strategy)
- Low-flow anesthesia: Using low fresh gas flow requires accurate end-tidal agent monitoring since inspired and alveolar concentrations diverge from vaporizer dial setting
- Desflurane caution: Its high vapor pressure (681 mmHg at 20°C) requires a heated pressurized vaporizer; rapid increases in desflurane concentration cause sympathetic stimulation and airway irritation (contraindicated for mask induction)
- Sevoflurane advantage: Low blood/gas coefficient + non-pungent smell = ideal for inhalation induction in children
11. Additional MAC Concepts (Advanced)
- MAC-EI (endotracheal intubation): The MAC that prevents response to laryngoscopy/intubation - higher than skin incision MAC (~1.3 MAC for most agents) because intubation is a stronger stimulus
- MAC-hour: Cumulative anesthetic exposure dose (1.0 MAC × 1 hour = 1 MAC-hour). Used in PONV risk scoring (Apfel score) and in tracking exposure
- Context-sensitive half-time of volatiles: Unlike IVAs, wash-out of volatiles from tissues is not highly context-sensitive for agents with low blood/gas coefficients (desflurane, sevoflurane recover predictably)
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 8, pp. 281-296
- Miller's Anesthesia, 10e - Inhaled Anesthetics chapters
- Lippincott Illustrated Reviews: Pharmacology - Chapter 20, pp. 665-669
- Barash Clinical Anesthesia, 9e - Neuropharmacology of Inhaled Anesthetics
How is blood gas coefficient related,simple explanation and also factors affecting uptake-explain properly.
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Perfect - I have everything needed. Here's the full, clear explanation:
Blood/Gas Partition Coefficient - Simple Explanation
The Core Idea: Blood as a "Sponge"
Think of blood as a sponge sitting between the alveoli and the brain.
- The goal of inhalational anesthesia is to get the anesthetic from the alveolus → into the blood → into the brain
- The brain only responds to partial pressure, not total amount
- So you need to build up partial pressure in the alveolus fast - and whatever "steals" the drug away from the alveolus slows that build-up
The blood/gas partition coefficient tells you how greedily the blood sponge soaks up the drug.
What the Number Actually Means
Blood/gas partition coefficient = concentration in blood / concentration in gas, at equilibrium (equal partial pressures)
| Agent | Blood/Gas Coefficient |
|---|---|
| Isoflurane | 1.4 |
| Sevoflurane | 0.65 |
| Nitrous oxide | 0.47 |
| Desflurane | 0.42 |
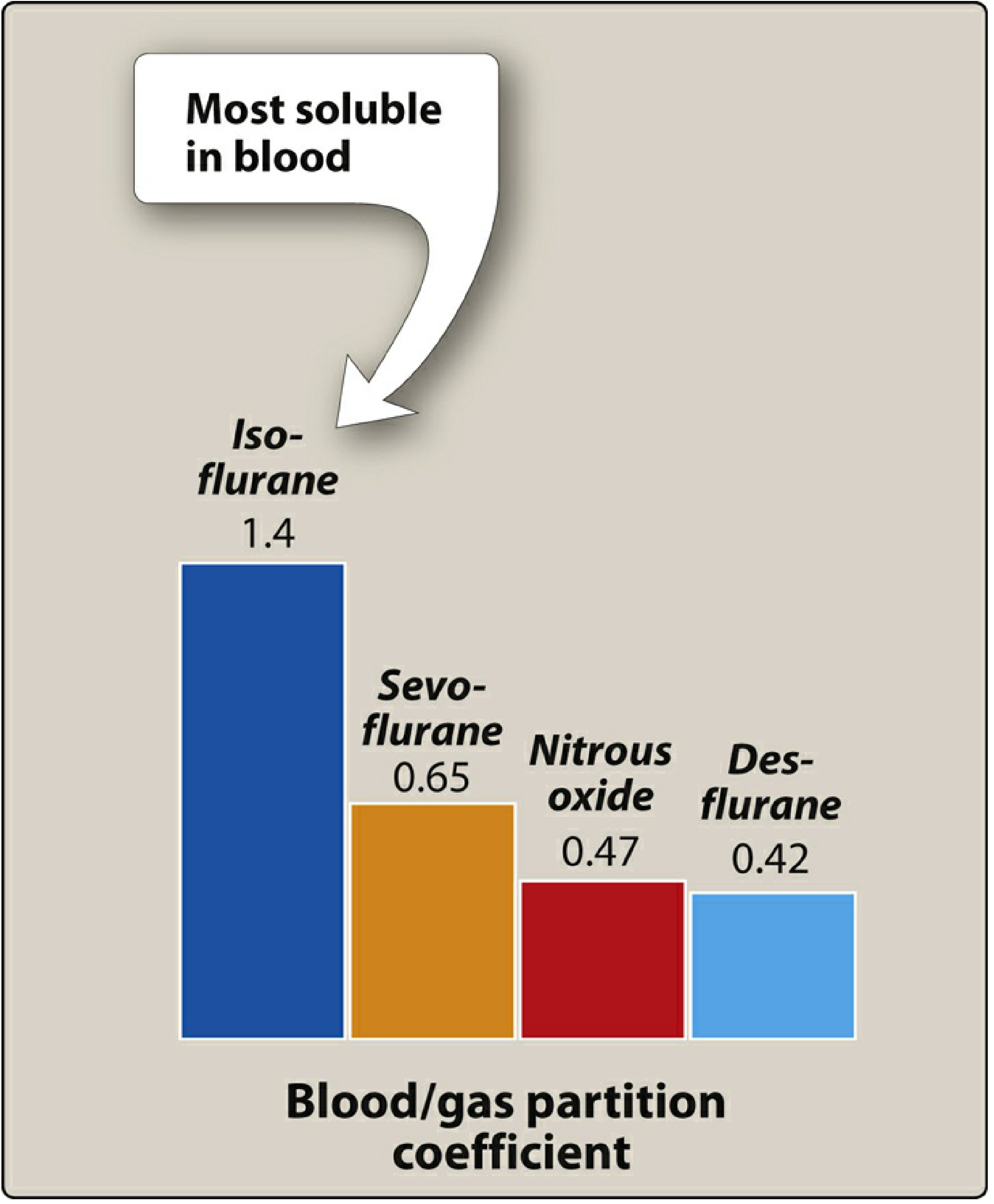
Take N₂O (0.47): at equilibrium, 1 mL of blood holds only 0.47x as much N₂O as 1 mL of alveolar gas. The blood doesn't absorb much - so partial pressure in the alveolus rises quickly.
Take isoflurane (1.4): blood holds 1.4x more per mL. Blood soaks up far more drug before equilibrating, draining the alveolus and delaying the rise in alveolar (and therefore brain) partial pressure.
The Golden Rule
High blood/gas coefficient = HIGH blood solubility = HIGH uptake = SLOW induction (and slow emergence) Low blood/gas coefficient = LOW blood solubility = LOW uptake = FAST induction (and fast emergence)
Simple Analogy:
Imagine filling a bucket (alveolus) from a tap (vaporizer), but there's a leak (blood uptake).
- Desflurane/N₂O = tiny leak. Bucket fills fast → brain partial pressure rises fast → fast induction.
- Isoflurane = big leak. Water keeps draining out → bucket takes ages to fill → slow induction.
The same logic works in reverse for emergence: agents with high blood solubility "store" more in the blood/tissues, so they take longer to wash out.
Induction & Emergence Curves (FA/FI)
This graph shows FA (alveolar concentration) rising as a fraction of FI (inspired concentration) over time:
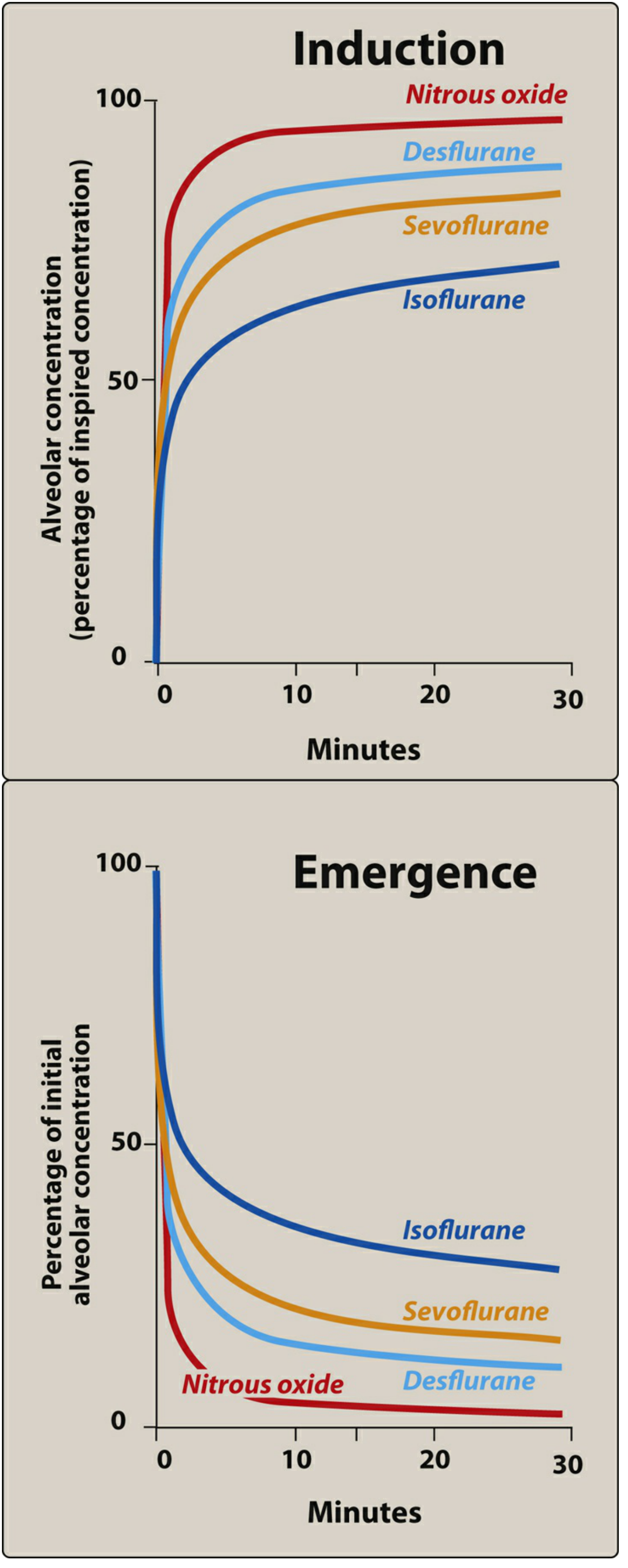
- N₂O and desflurane - FA/FI shoots up rapidly (low blood solubility, not "stolen" by blood)
- Isoflurane - FA/FI rises slowly (high solubility, blood keeps absorbing it)
- Emergence mirrors induction: the same agents that induce slowly also have prolonged recovery
- Lippincott Pharmacology, pp. 669-671; Morgan & Mikhail 7e, p. 281
Factors Affecting Uptake - Full Explanation
The key formula to remember:
Uptake = Solubility (λ b/g) × Cardiac Output × (Alveolar PP - Venous PP)
Three primary factors drive uptake. Each one understood properly will help you predict every clinical scenario.
Factor 1: Solubility in Blood (Blood/Gas Coefficient)
Already explained above. The higher the solubility:
- The more drug blood "steals" from the alveolus per unit time
- The slower FA rises
- The slower induction proceeds
Clinical implication: Postprandial lipemia increases blood/gas solubility (fat in blood makes it absorb more). Anemia decreases it (less protein/lipid in blood → less uptake → slightly faster induction).
Factor 2: Cardiac Output (Alveolar Blood Flow)
This one confuses many residents. Think it through carefully.
High Cardiac Output → Slower Induction
- More blood per minute flows through the lungs
- More drug is picked up from the alveolus each minute
- FA/FI rise is slowed (more drug "drained away")
- Brain gets drug at a dilute concentration for a longer time
- Induction is delayed
Low Cardiac Output → Faster Induction (but DANGER)
- Less blood passes the alveolus per minute
- Less drug is removed → FA builds up rapidly
- But crucially: the brain is also perfused less, so there's a competing effect
- Net result: for soluble agents (isoflurane), low CO dramatically accelerates alveolar build-up → risk of overdose
- For insoluble agents (desflurane, N₂O), CO matters much less because very little is taken up anyway regardless
Danger scenario: A patient in cardiogenic shock getting isoflurane. The low CO causes rapid FA rise → accidental overdose → further BP drop → disaster. This is why sick patients need much lower dial settings.
Effect of CO is most pronounced for soluble agents; least pronounced for insoluble ones.
- Morgan & Mikhail 7e, p. 282
Factor 3: Alveolar-to-Venous Partial Pressure Gradient (A-V Gradient)
- Blood returning from the tissues (venous blood) has been giving up anesthetic to the organs
- The more the tissues take up, the lower the venous partial pressure
- A large A-V gradient means tissues are hungry for drug → they keep pulling it out of the blood → blood keeps pulling it from the alveolus → FA rises slowly
What drives this gradient?
Tissue uptake depends on three analogous sub-factors:
| Sub-factor | Effect |
|---|---|
| Tissue/blood solubility coefficient | Higher = tissues absorb more = larger gradient maintained |
| Tissue blood flow | Higher flow = more drug delivered/removed = larger gradient |
| Arterial-tissue partial pressure difference | Larger difference = more uptake = larger gradient |
The Four Tissue Compartments:
| Group | Examples | % Body Weight | % Cardiac Output | Behaviour |
|---|---|---|---|---|
| Vessel-rich | Brain, heart, liver, kidney | 10% | 75% | Saturates quickly (minutes); first to equilibrate |
| Muscle | Skeletal muscle, skin | 50% | 19% | Moderate flow, large volume; uptake sustained for hours |
| Fat | Adipose tissue | 20% | 6% | Poor flow but enormous capacity (fat/blood solubility very high); would take days to equilibrate |
| Vessel-poor | Bone, ligament, cartilage | 20% | ~0% | Negligible uptake - clinically irrelevant |
The initial steep rise in FA/FI is due to unopposed filling of alveoli before much tissue uptake has occurred. The rate of rise slows as the vessel-rich group equilibrates and begins returning drug-laden venous blood (reducing the A-V gradient), and then slows again as the muscle group gradually saturates.
Fat never fully equilibrates during clinical anesthesia - it acts as an infinite sink for prolonged cases, especially relevant for highly lipid-soluble agents (halothane, isoflurane) in long or obese patients.
- Morgan & Mikhail 7e, pp. 282-283; Lippincott Pharmacology, pp. 671-672
Additional Factors Affecting Alveolar Concentration (FA)
4. Alveolar Ventilation
This affects the delivery side (how fast FI fills the alveolus), not purely uptake:
- Higher minute ventilation → faster wash-in → faster FA rise toward FI
- Ventilation matters most for soluble agents (because they are rapidly "drained" - so you need to push more in)
- For insoluble agents, the effect of increased ventilation is minor (FA already rises fast)
- Hypoventilation (opioid respiratory depression) slows induction of soluble agents considerably
5. Functional Residual Capacity (FRC)
- Large FRC = large reservoir of non-anesthetic gas in the lungs at the start
- Takes more breaths to "wash in" the agent → slower initial rise of FA
- This is why pre-oxygenation/denitrogenation is important and why obese/FRC-reduced patients have faster wash-in
6. Concentration Effect
When you deliver a high inspired concentration of a gas (especially N₂O), the rapid uptake of large volumes of that gas creates a slight vacuum effect that:
- Concentrates the remaining gas in the alveolus (raises FA)
- Draws in more fresh gas from the airways (increases effective ventilation)
Both effects accelerate the FA/FI rise beyond what simple calculations would predict. This is the concentration effect - clinically relevant mainly for N₂O at high concentrations.
7. Second Gas Effect
If you deliver N₂O alongside a volatile agent (e.g., isoflurane), the rapid uptake of N₂O:
- Concentrates the volatile agent in the alveolus
- Simultaneously augments ventilation (drawing in more volatile)
Net effect: the FA of the second gas (isoflurane) rises faster than it would if given alone. This is the second gas effect - the mechanism behind why N₂O + volatile combinations speed induction.
Summary: The Big Picture
FA/FI rises FASTER when: FA/FI rises SLOWER when:
- Low blood/gas coefficient - High blood/gas coefficient
- Low cardiac output - High cardiac output
- Small A-V gradient - Large A-V gradient
- High minute ventilation - Low minute ventilation
- Small FRC - Large FRC
- High inspired concentration - Low inspired concentration
(concentration effect)
And remember: emergence is the exact reverse of induction. All the same factors apply, but now the alveolus is empty (agent turned off) and drug flows from tissues → blood → alveolus → exhaled.
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 281-284; Lippincott Illustrated Reviews Pharmacology, pp. 669-673
This is a shared conversation. Sign in to Orris to start your own chat.