Lung cancer Explain everything under it using images Refer mbbs final year
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching the Web
lung cancer types squamous adenocarcinoma small cell large cell histology gross pathology images MBBS
Loading Image
Loading Image
Searching the Web
lung cancer pancoast tumor superior sulcus chest xray CT scan TNM staging diagram
Loading Image
Searching the Web
lung cancer TNM staging 8th edition table diagram NSCLC SCLC paraneoplastic syndromes Horner syndrome
Loading Image
Loading Image
Searching the Web
lung cancer clinical features superior vena cava syndrome Pancoast Horner syndrome diagram anatomy
Loading Image
Loading Image
Loading Image
🫁 Lung Cancer — Complete MBBS Final Year Notes
Sources: Robbins & Kumar Basic Pathology, Mulholland & Greenfield's Surgery (7e), Fishman's Pulmonary Diseases, Harrison's Principles of Internal Medicine 22e
1. INTRODUCTION & EPIDEMIOLOGY
- Leading cause of cancer-related death in both men and women worldwide
- ~237,000 new cases / year (USA 2022); ~130,000 deaths/year
- Peak incidence: 5th-6th decade of life
- >50% of patients already have distant metastases at diagnosis
- Overall 5-year survival: ~20% (all stages combined); ~50% if localized
- Adenocarcinoma has now replaced squamous cell carcinoma as the most common primary lung tumor (as tobacco use has declined)
2. ETIOLOGY & RISK FACTORS
| Risk Factor | Notes |
|---|---|
| Cigarette smoking | 90% of lung cancers. Risk 60x higher in heavy smokers (2 packs/day × 20 yrs) |
| Passive smoking | Modestly elevated risk |
| Asbestos | 5x alone; 55x combined with smoking |
| Radon gas | Second leading cause of lung cancer in non-smokers |
| Uranium / radioactive dust | Occupational |
| Arsenic, chromium, nickel, vinyl chloride | Occupational carcinogens |
| P-450 polymorphisms | Genetic susceptibility |
Smoking is the dominant risk factor for all histologic types. Women are more susceptible to tobacco carcinogens than men.
- Robbins & Kumar Basic Pathology, p.485
3. WHO CLASSIFICATION (2021) — HISTOLOGIC TYPES
| Category | Types |
|---|---|
| Adenocarcinoma | Acinar, papillary, micropapillary, solid, lepidic, mucinous |
| Squamous cell carcinoma | Keratinizing, non-keratinizing |
| Large cell carcinoma | Undifferentiated |
| Neuroendocrine | Small cell carcinoma, Carcinoid tumor |
| Mixed / Others | Adenosquamous, Sarcomatoid, Giant cell, Spindle cell |
4. THE FOUR MAJOR TYPES — IN DETAIL
🔬 Histology of all four types:

A. ADENOCARCINOMA (Most common — ~40% of all lung cancers)
Key facts:
- Most common type overall; most common in women, non-smokers, and age <45
- Peripheral location (subpleural) — arises from bronchioalveolar duct junction
- Grows more slowly but metastasizes early
- Grows along alveolar walls ("lepidic spread")
Precursor sequence:
Atypical adenomatous hyperplasia (AAH) → Adenocarcinoma in situ (AIS) → Minimally invasive → Invasive adenocarcinoma
Molecular markers:
- EGFR mutations (common in non-smoking women, East Asians — ~20%) → sensitive to gefitinib/erlotinib
- KRAS mutations (~30%) — mutually exclusive with EGFR
- ALK fusions (4-6%) → respond to crizotinib
- ROS1, HER2, MET, BRAF V600E — targetable mutations
- TTF-1 positive on IHC — relatively specific for lung adenocarcinoma
Morphology: Gland-forming (acinar); papillary; mucinous; solid patterns; mucin present
B. SQUAMOUS CELL CARCINOMA (~25-30%)
Key facts:
- Strongly linked to smoking (strongest among NSCLC)
- Central location — arises from major bronchi
- Spreads first to hilar lymph nodes, then mediastinal
- Metastasizes later than adenocarcinoma
- Large lesions may undergo central cavitation
Precursor sequence:
Squamous metaplasia → Squamous dysplasia → Carcinoma in situ → Invasive carcinoma
Histology: Keratin pearls + intercellular bridges (well-differentiated); may be poorly differentiated with minimal squamous features
Key paraneoplastic association: Hypercalcemia via PTH-rP secretion
C. SMALL CELL LUNG CARCINOMA (SCLC — ~13-15%)
Key facts:
- Most aggressive — almost always widely metastasized at diagnosis
- Central location, near major bronchi/hilar regions
- Neuroendocrine origin — derived from Kulchitsky (APUD) cells
- NOT surgically resectable in most cases
- Responds well to chemotherapy + radiotherapy but invariably recurs
Histology (hallmark features):
- Small cells with scant cytoplasm
- "Oat-shaped" nuclei — dark, hyperchromatic, fine chromatin ("salt and pepper")
- Indistinct nucleoli
- Diffuse sheets (no glandular/squamous architecture)
- Neuroendocrine markers: chromogranin A, synaptophysin, CD56, dense core granules on EM
Genetics: ~90% TP53 mutations, ~90% RB mutations, ~90% 3p deletions
Paraneoplastic syndromes (SCLC is the classic cause):
- SIADH (ADH secretion) → hyponatremia
- Ectopic ACTH → Cushing's syndrome
- Lambert-Eaton Myasthenic Syndrome (anti-VGCC antibodies)
- Limbic encephalitis (anti-Hu antibodies)
- Gastrin-releasing peptide, calcitonin secretion
Staging (SCLC — Veterans Administration system):
- Limited stage (LS): Confined to one hemithorax + regional nodes (can fit in one radiation portal). Response rate 85-90%; median survival 18-24 months; 2-yr survival 40-50%
- Extensive stage (ES): Beyond LS. Response rate 75-85% to chemo; median survival 7-11 months; 2-yr survival <5%
D. LARGE CELL CARCINOMA (~10%)
- Undifferentiated — diagnosis of exclusion
- No glandular, squamous, or neuroendocrine features
- Peripherally located
- Highly aggressive with early metastasis
- Responds poorly to all treatment
5. SCLC vs NSCLC — COMPARISON TABLE
(from Robbins & Kumar Basic Pathology, p.488)
| Feature | SCLC | NSCLC (Adenocarcinoma / SCC) |
|---|---|---|
| Microscopy | Scant cytoplasm; small hyperchromatic nuclei; indistinct nucleoli; diffuse sheets | Abundant cytoplasm; pleomorphic nuclei; prominent nucleoli; glandular or squamous architecture |
| Neuroendocrine markers (chromogranin, synaptophysin, CD56) | Present | Absent |
| Mucin | Absent | Present (adenocarcinoma) |
| TP53 mutations | ~90% | ~50% |
| RB mutations | ~90% | ~20% |
| KRAS mutations | Rare | ~30% (adenocarcinoma) |
| EGFR mutations | Absent | ~20% (adenocarcinoma) |
| ALK fusions | Absent | 4-6% (adenocarcinoma) |
| Response to chemo/RT | Often complete response but recurs | Incomplete |
| Response to checkpoint inhibitors | Less responsive | Responsive |
| Surgery | Rarely curative | Potentially curative (early stages) |
| Prognosis | Very poor (median survival ~1 year) | Moderately poor; improving with targeted therapy |
6. PATHOGENESIS & MOLECULAR BIOLOGY
Sequential mutation model (analogous to adenoma-carcinoma in colon):
- 3p deletion (very early event — seen in benign bronchial epithelium of smokers) — "field effect"
- KRAS/EGFR mutations — occur relatively late
- TP53 + RB mutations — near-universal in SCLC
- p16/CDKN2A mutations — more in NSCLC (~50%)
Key molecular targets for personalized therapy (NSCLC):
| Target | Frequency | Drug |
|---|---|---|
| EGFR mutation | ~20% (adenocarcinoma) | Gefitinib, erlotinib, osimertinib |
| ALK fusion | 4-6% | Crizotinib, alectinib |
| ROS1 fusion | 1-2% | Crizotinib |
| KRAS G12C | ~13% | Sotorasib |
| BRAF V600E | 1-3% | Dabrafenib + trametinib |
| PD-L1 expression | Variable | Pembrolizumab (checkpoint inhibitor) |
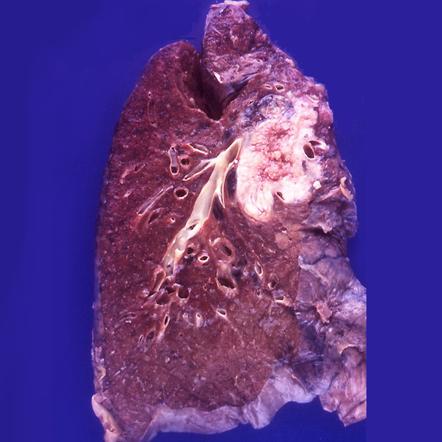
7. GROSS MORPHOLOGY
Gross specimen of lung carcinoma showing a large central hilar mass with surrounding consolidation:
8. CLINICAL FEATURES
A. Local/Primary Tumor Effects
| Symptom | Mechanism |
|---|---|
| Cough (persistent, progressive) | Bronchial irritation |
| Hemoptysis | Tumor erosion into bronchial vessels |
| Dyspnea / wheezing | Airway obstruction |
| Chest pain | Pleural invasion |
| Post-obstructive pneumonia | Obstruction of bronchus → recurrent infections |
| Stridor | Tracheal compression |
| Hoarseness | Left recurrent laryngeal nerve compression |
B. Local Spread Effects
| Structure invaded | Consequence |
|---|---|
| Phrenic nerve | Diaphragmatic paralysis |
| Esophagus | Dysphagia |
| SVC | Superior Vena Cava (SVC) syndrome |
| Pericardium | Pericarditis / tamponade |
| Horner's syndrome | Ptosis, miosis, anhidrosis (sympathetic chain invasion — Pancoast) |
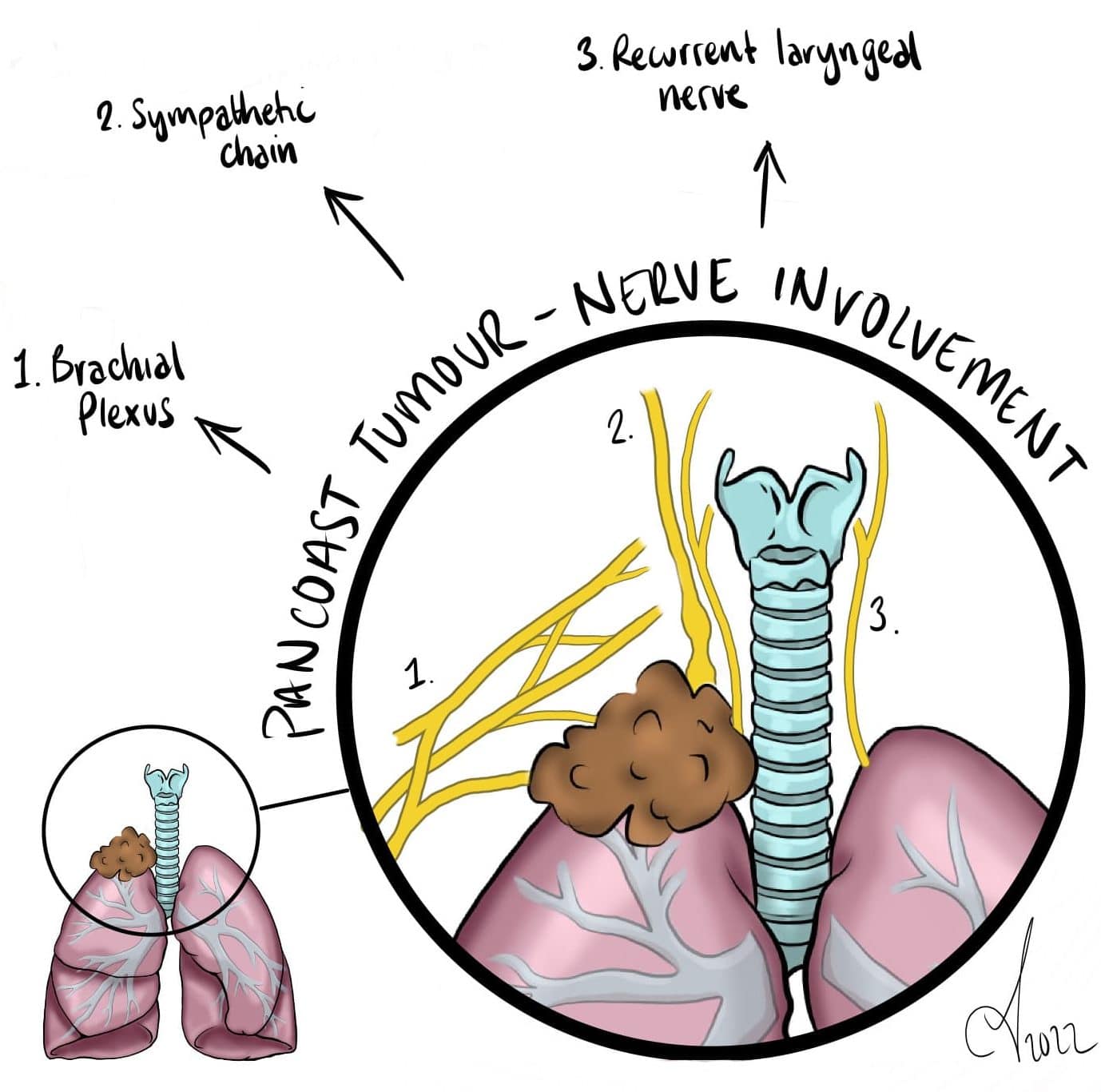
C. Pancoast Tumor (Superior Sulcus Tumor)
Accounts for 3-5% of all lung cancers. Arises at the apex of the lung, invades chest wall structures at or above the first rib.
Classic Pancoast-Tobias syndrome:
- Severe shoulder and upper limb pain (along ulnar distribution, C8/T1/T2 roots)
- Horner's syndrome — ptosis, miosis, anhidrosis (sympathetic chain invasion)
- Hand muscle wasting (brachial plexus invasion)
9. PARANEOPLASTIC SYNDROMES
Clinically significant in 1-10% of lung cancer patients. Critical high-yield topic.
| Syndrome | Mediator | Tumor Type |
|---|---|---|
| SIADH → hyponatremia | ADH | SCLC |
| Cushing's syndrome (ectopic) | ACTH | SCLC |
| Hypercalcemia | PTH-rP | Squamous cell |
| Lambert-Eaton syndrome | Anti-VGCC (anti-P/Q-type calcium channel) | SCLC |
| Limbic encephalitis | Anti-Hu antibodies | SCLC |
| Hypertrophic pulmonary osteoarthropathy (HPOA) | Periosteal new bone formation | Adenocarcinoma / large cell |
| Gynecomastia | Gonadotropins | Large cell |
| Carcinoid syndrome | Serotonin, bradykinin | Carcinoid |
| Hypocalcemia | Calcitonin | SCLC |
10. DIAGNOSIS
A. Imaging
Chest X-ray:
- Peripheral mass / central hilar mass
- Post-obstructive atelectasis/consolidation
- Pleural effusion
- Mediastinal widening
CT scan of chest + abdomen:
- Gold standard for primary assessment
- Evaluates mediastinal lymph nodes (>10mm = suspicious), adrenal mets, liver mets
- CT sensitivity for mediastinal nodes: 57%, specificity 82%
FDG-PET scan:
- Superior to CT for mediastinal nodal staging
- Sensitivity 84%, specificity 89% for mediastinal disease
- Detects occult distant metastases
- Standard of care along with CT for NSCLC staging
MRI brain:
- Mandatory in all patients being evaluated for curative intent surgery
- Brain is common site of metastasis (especially adenocarcinoma, SCLC)
B. Tissue Sampling (Histologic Confirmation)
| Method | Best for |
|---|---|
| Flexible bronchoscopy + biopsy | Central tumors (sensitivity 88%) |
| CT-guided FNA / core biopsy | Peripheral lesions |
| Endobronchial Ultrasound (EBUS) | Mediastinal nodes |
| Sputum cytology | Rarely used; specificity 99%, low sensitivity |
| VATS (Video-Assisted Thoracoscopic Surgery) | Indeterminate peripheral nodule |
| Mediastinoscopy | Pathologic mediastinal node sampling |
C. Molecular Testing (Mandatory for NSCLC adenocarcinoma)
- EGFR, KRAS, ALK, ROS1, BRAF, NTRK, RET — for targeted therapy selection
- PD-L1 IHC — for checkpoint inhibitor eligibility
- Liquid biopsy (circulating tumor DNA) increasingly used
11. TNM STAGING (8th Edition — AJCC/UICC/IASLC)
Based on 94,708 NSCLC cases from multiple international centers (1990-2010).
TNM 9th Edition Reference (2025 update):
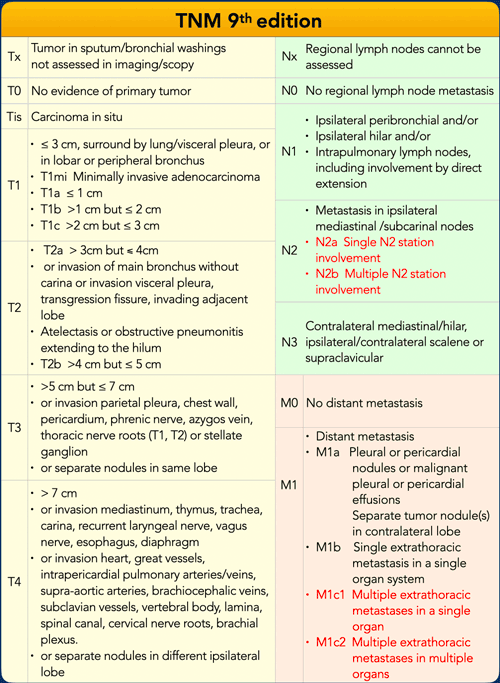
IASLC 8th Edition TNM Staging Summary Poster:

Key T Descriptors (8th/9th Edition):
| T | Definition |
|---|---|
| Tis | Carcinoma in situ (pure lepidic adenocarcinoma ≤3 cm) |
| T1a | ≤1 cm |
| T1b | >1-2 cm |
| T1c | >2-3 cm |
| T2 | >3-4 cm OR main bronchus without carina OR visceral pleura OR atelectasis to hilum |
| T3 | >5-7 cm OR chest wall/pericardium/phrenic nerve invasion OR satellite nodule same lobe |
| T4 | >7 cm OR mediastinum/heart/great vessels/trachea/carina invasion OR separate nodule different ipsilateral lobe |
Key N Descriptors:
| N | Definition |
|---|---|
| N0 | No regional lymph node metastasis |
| N1 | Ipsilateral peribronchial / hilar nodes |
| N2 | Ipsilateral mediastinal/subcarinal nodes |
| N3 | Contralateral mediastinal/hilar; scalene/supraclavicular |
Key M Descriptors:
| M | Definition |
|---|---|
| M0 | No distant metastasis |
| M1a | Pleural/pericardial nodules or malignant effusion; contralateral lung nodule |
| M1b | Single extrathoracic metastasis (oligometastasis) |
| M1c1 | Multiple extrathoracic in one organ |
| M1c2 | Multiple extrathoracic in multiple organs |
Stage Groupings:
| Stage | TNM | 5-year survival |
|---|---|---|
| IA | T1 N0 M0 | ~75-85% |
| IB | T2a N0 M0 | ~60-70% |
| IIA | T2b N0 M0 | ~50-60% |
| IIB | T1-2 N1 M0 / T3 N0 M0 | ~35-45% |
| IIIA | T1-3 N2 M0 / T3-4 N1 M0 | ~10-25% |
| IIIB | T1-4 N3 M0 / T4 N2 M0 | ~5-10% |
| IV | Any T, Any N, M1 | <5% at 5 years |
12. METASTATIC SITES
NSCLC common mets: Brain, bone, liver, adrenal glands, contralateral lung, supraclavicular nodes
SCLC common mets: Bone marrow, liver, brain, bone — almost always present at diagnosis
Evaluation: CT chest + abdomen, MRI brain, FDG-PET whole body, +/- bone scan
13. TREATMENT
A. NSCLC
| Stage | Treatment |
|---|---|
| Stage I-II (resectable) | Surgical resection (lobectomy preferred; wedge/segmentectomy for poor reserve) ± adjuvant chemotherapy |
| Stage IIIA | Multimodality: neoadjuvant chemoradiation → surgery OR definitive concurrent chemoradiation |
| Stage IIIB | Concurrent chemoradiation (not resectable) |
| Stage IV | Systemic therapy guided by molecular profile: targeted therapy (EGFR/ALK/ROS1 inhibitors), immunotherapy (pembrolizumab if PD-L1 ≥50%), platinum-based chemotherapy |
Surgery types:
- Lobectomy (standard/preferred)
- Pneumonectomy (for central tumors)
- VATS (Video-Assisted Thoracoscopic Surgery) — minimally invasive
B. SCLC
| Stage | Treatment | Outcome |
|---|---|---|
| Limited stage | Etoposide + cisplatin + concurrent thoracic RT → prophylactic cranial irradiation (PCI) | Response 85-90%; median survival 18-24 months |
| Extensive stage | Etoposide + cisplatin/carboplatin ± atezolizumab (immunotherapy) | Response 75-85%; median survival 7-11 months |
| Surgery | Only for very early T1-2 N0 (rare); followed by adjuvant chemo | 5-year survival 30-50% for T1N0 |
Prognosis: Median survival with treatment ~1 year; only 5% alive at 10 years.
14. IMMUNOTHERAPY
- High mutation burden from tobacco carcinogens → tumor neoantigens → immunogenic
- PD-L1 on tumor cells blocks PD-1 on CD8+ T cells → immune evasion
- Checkpoint inhibitors (pembrolizumab, nivolumab, atezolizumab) block this interaction
- NSCLC: Responsive — especially if PD-L1 ≥50% (pembrolizumab first-line monotherapy)
- SCLC: Relatively unresponsive — mechanisms being studied
15. PROGNOSIS SUMMARY
| Histotype | Resectable? | 5-yr survival |
|---|---|---|
| Adenocarcinoma (early) | Yes | ~50% (localized) |
| Squamous cell (early) | Yes | ~40-50% (localized) |
| Large cell | Rarely early | Poor |
| SCLC | Rarely (<10%) | 5% at 10 years |
| All stages combined | — | ~20% |
16. HIGH-YIELD MNEMONICS FOR FINALS
"SCLC MNEMONIC" — remember the paraneoplastic syndromes:
- SIADH
- Cushing's (ectopic ACTH)
- Lambert-Eaton
- Central location
"SCC — CENTRAL + CAVITATES + CALCIUM (PTH-rP)"
"ADC — PERIPHERAL + PERIPHERAL LOCATION + EGFR/ALK mutations + women/non-smokers"
Pancoast = Apex tumor → brachial plexus (C8/T1/T2) + sympathetic chain (Horner) + recurrent laryngeal nerve (hoarseness)
References:
- Robbins & Kumar Basic Pathology, pp. 483-497
- Mulholland & Greenfield's Surgery, Scientific Principles and Practice 7e, pp. 4267-4282
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
- Harrison's Principles of Internal Medicine 22E
- TNM 8th/9th Edition — IASLC / AJCC / UICC
This is a shared conversation. Sign in to Orris to start your own chat.