Acromegaly
Reading File
Finding Sources
Searching PubMed
acromegaly treatment management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive information to write a thorough, well-structured answer. Let me compile it:
Acromegaly
Definition
Acromegaly is a syndrome of chronic GH (growth hormone) excess occurring after epiphyseal plate closure. When GH excess occurs before epiphyseal fusion (in children/adolescents), the result is gigantism rather than acromegaly. The name comes from the Greek for "large extremities."
Etiology
98% of cases originate from a pituitary adenoma (somatotroph adenoma). The breakdown by tumor type is:
| Cause | Prevalence |
|---|---|
| Densely/sparsely granulated GH cell adenoma | ~60% |
| Mixed GH + PRL cell adenoma | ~25% |
| Mammosomatotrope cell adenoma | ~10% |
| Plurihormonal adenoma (also secreting ACTH, TSH, or α-subunit) | rare |
| Ectopic pituitary tissue (nasopharynx, sphenoid sinus) | rare |
| Extrapituitary GH-secreting tumor (pancreatic islet cell, lymphoma) | <1% |
| Ectopic GHRH secretion (bronchial carcinoid, small-cell lung cancer, pancreatic islet cell tumor, medullary thyroid carcinoma, pheochromocytoma) | <1% |
Genetic associations: MEN1 (menin gene mutation - pituitary adenoma in 50% of MEN1 patients, 10% secrete GH), McCune-Albright syndrome (activating Gsα mutation causing ligand-independent cAMP elevation and GH hypersecretion), and Carney complex.
- Harrison's Principles of Internal Medicine 22E, p. 3051
- Goldman-Cecil Medicine, p. 1471
Pathophysiology
GH acts directly on peripheral tissues and also stimulates hepatic IGF-1 (somatomedin C) production. IGF-1 mediates most of GH's tissue-growth effects. In normal physiology, IGF-1 feeds back to inhibit GH release. In acromegaly, a GH-secreting adenoma escapes this feedback, leading to:
- Continuous soft tissue and bony overgrowth
- Metabolic effects (insulin resistance, lipolysis)
- Organomegaly (viscera, heart, thyroid, salivary glands)
Clinical Features
Symptoms are often subtle and progressive, with an average diagnostic delay of 10+ years from onset. By the time of diagnosis, 75% of pituitary adenomas are macroadenomas (>10 mm).
Skeletal/Craniofacial
- Coarsening of facial features (frontal bossing, prognathism, macroglossia, splayed teeth, malocclusion)
- Enlargement of hands and feet (patients notice increasing ring, shoe, and hat size)
- Acromegalic arthropathy - initially cartilage hypertrophy widens joints (especially MCP joints visible on hand X-ray), then premature osteoarthritis develops as cartilage weakens; spinal involvement can cause cord compression
- Generalized osteoporosis (from hypogonadism and direct GH effects)
Skin
- Thickened, oily skin with exaggerated skin folds (nasolabial grooves, forehead wrinkling)
- Hyperhidrosis (excessive sweating at rest - very common and persistent even after treatment)
- Skin tags (acrochordon) - often associated with premalignant colonic polyps and colon cancer
- Hypertrichosis, hyperpigmentation
- Cutis verticis gyrata (~30% of patients)
- Thick lips and tongue
Mass Effects (Pituitary Tumor)
- Headaches (up to 60% at presentation)
- Bitemporal hemianopsia (~10%) from optic chiasm compression
- Cranial nerve palsies (in invasive tumors)
Systemic/Metabolic Complications
- Cardiovascular: Cardiomegaly (myocardial hypertrophy), hypertension, increased risk of ischemic heart disease and heart failure - the leading cause of death in untreated acromegaly
- Respiratory: Sleep apnea (obstructive, due to macroglossia and pharyngeal soft tissue enlargement; also central)
- Metabolic: Glucose intolerance/diabetes mellitus (GH is counter-regulatory, causing insulin resistance)
- Neurological: Carpal tunnel syndrome (median nerve entrapment), peripheral neuropathy
- Renal: GH and IGF-1 enhance phosphate reabsorption in proximal tubules (via increased Npt2a expression), leading to hyperphosphatemia; also associated with hypercalciuria and nephrolithiasis
- ENT: Voice deepening (resonant, rough voice), prognathism causing dental problems, enlarged sinuses
Co-secretion
- Mixed GH+PRL tumors produce features of hyperprolactinemia (hypogonadism, galactorrhea, infertility) on top of acromegaly
- Acidophilic stem cell adenomas often have hyperprolactinemia features predominating
Diagnosis
Step 1 - Screening: Serum IGF-1
- Age- and gender-matched serum IGF-1 is the single best screening test
- Elevated in virtually all cases; correlates well with 24-hour GH secretion
- Random GH is unreliable due to pulsatile secretion (normal peaks can exceed 50 ng/mL)
Step 2 - Confirmation: Oral Glucose Tolerance Test (OGTT)
- 75 g oral glucose load; measure GH at 0, 30, 60, 90, 120 minutes
- Normal: GH suppressed to <0.3 μg/L (nadir)
- Acromegaly: GH fails to suppress below 0.3 μg/L (or paradoxical rise)
- Combination of failure to suppress GH + elevated IGF-1 = diagnostic of acromegaly
- Normal IGF-1 + GH suppression to <0.3 μg/L excludes acromegaly
Step 3 - Imaging: Pituitary MRI
- MRI with contrast to identify and characterize the adenoma (size, extension, cavernous sinus invasion)
- Used to plan surgery and assess completeness of resection
Additional workup
-
Assess for co-secretion (prolactin, ACTH, TSH, α-subunit)
-
Screen for associated conditions: colonoscopy (colon polyps/cancer), echocardiogram (cardiomyopathy), sleep study (sleep apnea)
-
If no pituitary adenoma found on MRI: measure plasma GHRH to look for ectopic source; CT chest/abdomen to look for carcinoid tumor
-
Henry's Clinical Diagnosis and Management by Laboratory Methods
-
Harrison's Principles of Internal Medicine 22E, p. 3051
Treatment
The goal of treatment is biochemical remission: normalization of age-matched IGF-1 and GH <1 μg/L (random) or <0.4 μg/L (after OGTT).
1. Surgery (First-line for most patients)
Transsphenoidal microsurgical adenomectomy is the preferred primary treatment:
- Curative in ~85% of microadenomas (GH normalized postoperatively)
- Only ~50% of macroadenomas are cured by surgery alone (due to cavernous sinus invasion or large size)
- Rapid relief of mass effects (headache, visual field defects improve within days)
2. Somatostatin Receptor Ligands (SRLs) - Primary Medical Therapy
Octreotide LAR (long-acting, monthly IM injection) and lanreotide (monthly deep SC injection) are the main SRLs. Oral octreotide capsules are a newer formulation.
- Normalize IGF-1 in ~50-70% of patients
- Reduce tumor size in many patients
- Can be used as primary therapy when surgery is not feasible (e.g., medically unfit patient, patient preference) or as adjuvant therapy after incomplete surgery
Side effects of SRLs:
- Transient nausea, abdominal discomfort, diarrhea, fat malabsorption (resolves within 2 weeks)
- Gallstones/biliary sludge (up to 30% with long-term use, usually asymptomatic)
- Mild glucose intolerance (transient insulin suppression)
- Asymptomatic bradycardia, mild hypothyroxinemia
Pasireotide (2nd-generation SRL with broader receptor affinity): similar efficacy but significantly higher risk of glucose intolerance and new-onset diabetes mellitus.
3. GH Receptor Antagonist: Pegvisomant
- Blocks peripheral GH binding to its receptor → suppresses IGF-1 production
- Daily subcutaneous injection (10-30 mg/day)
- Normalizes IGF-1 in ~70% of patients even in SRL-resistant cases
- Note: GH levels remain elevated (does not act on the adenoma) - monitor tumor size with MRI
- Side effects: reversible liver enzyme elevation, lipodystrophy, injection site pain
Combination therapy: Monthly SRL + weekly/biweekly pegvisomant is effective for treatment-resistant patients.
4. Dopamine Agonists
- Cabergoline at very high doses (up to 0.5 mg/day) achieves modest GH suppression
- Combined octreotide + cabergoline may have additive biochemical control
- Used as adjuvant in patients with co-secreting GH+PRL tumors or mild residual disease
5. Radiation Therapy
- External beam radiotherapy or stereotactic radiosurgery (Gamma Knife, CyberKnife)
- Reserved for patients with residual/recurrent disease not controlled by surgery or medical therapy
- Advantage: does not require patient compliance with ongoing treatment
- Disadvantage: slow effect - 50% of patients need ≥8 years to achieve GH <5 μg/L; 90% achieve this after 18 years
- Major concern: hypopituitarism develops in most patients (gonadotropin, ACTH, TSH deficiency) within 10 years of radiotherapy
Management Algorithm
The following flowchart from Harrison's (2025) summarizes the treatment approach:
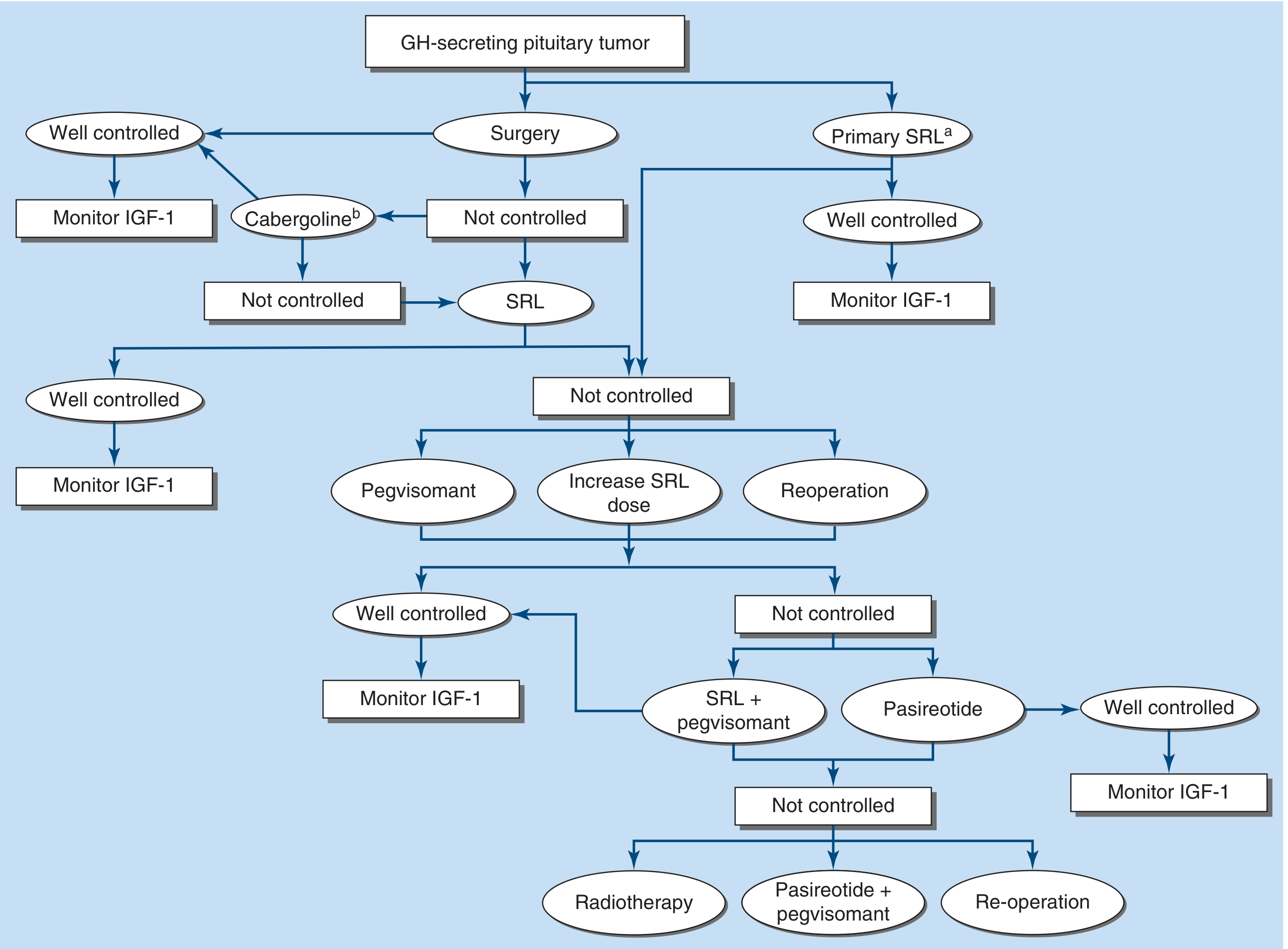
Figure 392-3, Harrison's Principles of Internal Medicine 22E - Management of acromegaly. SRL = somatostatin receptor ligand.
Prognosis
Untreated acromegaly reduces life expectancy by ~10 years, primarily due to cardiovascular and cerebrovascular complications. Successful biochemical control normalizes mortality to that of the general population. Persistent hyperhidrosis is common even after otherwise successful treatment. Bony and structural changes (prognathism, enlarged hands/feet) do not reverse with treatment; only soft tissue changes improve.
Differential Diagnosis
- Pseudoacromegaly: Acquired in severe insulin-resistant diabetes (fibroblast defect) or with long-term minoxidil use - no GH/IGF-1 abnormality
- Acromegaloid facial appearance syndrome: Inherited condition with only facial changes, normal GH
- Pachydermoperiostosis, Paget disease, myxedema - can mimic facial/acral changes
- Leonine facies of leprosy (Hansen disease)
Recent Evidence
A 2025 network meta-analysis on medical treatment in acromegaly (PMID 41140134, Eur J Endocrinol) and a 2025 CNS systematic review on perioperative medical management of functioning pituitary adenomas (PMID 40815128, Neurosurgery) are the most recent high-quality evidence reviews. These reinforce SRLs as the cornerstone of medical therapy and support perioperative SRL use in select patients.
Sources: Harrison's Principles of Internal Medicine 22E | Goldman-Cecil Medicine | Andrews' Diseases of the Skin | Grainger & Allison's Diagnostic Radiology | Comprehensive Clinical Nephrology, 7th Ed. | Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.