Coventional methods of tonsiilectomy
Reading File
Finding Sources
Searching the Web
conventional methods of tonsillectomy surgical techniques
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from both Pfenninger and Cummings. Let me compile the full answer.
Conventional Methods of Tonsillectomy
Tonsillectomy techniques are broadly classified into two anatomical categories based on the plane of dissection:
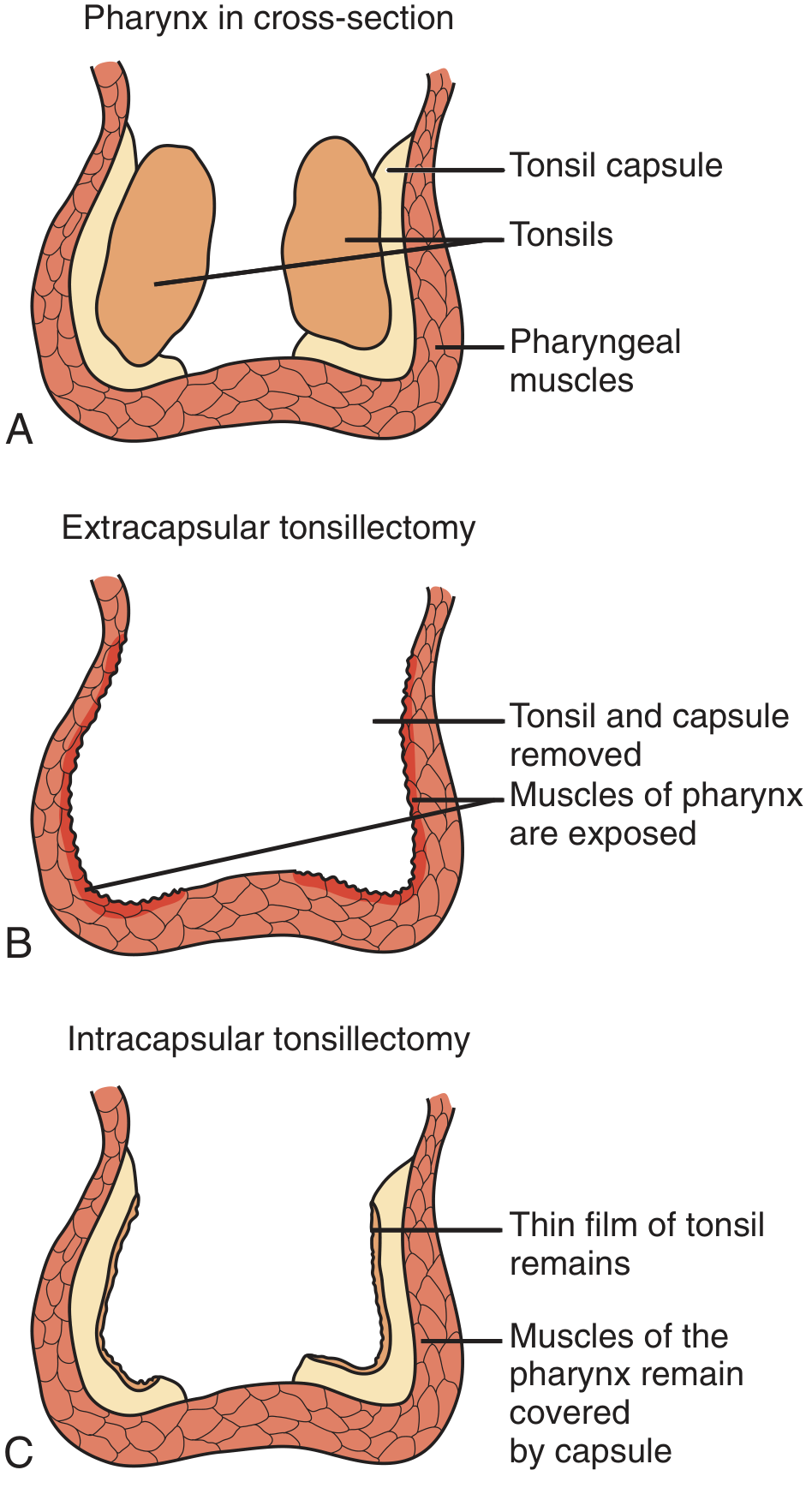
A: Normal anatomy — tonsil separated from pharyngeal muscle by a fibrous capsule. B: Extracapsular (subcapsular) tonsillectomy — tonsil + capsule removed, pharyngeal muscle left to re-epithelialize. C: Intracapsular tonsillectomy — capsule and a thin film of tonsil remain.
I. Classification by Dissection Plane
1. Extracapsular (Subcapsular) Tonsillectomy
The favored method in current practice. The entire tonsil and its capsule are dissected off the surrounding pharyngeal constrictor musculature. No residual capsule or tonsillar tissue is left, reducing the risk of delayed complications and recurrence.
2. Intracapsular Tonsillectomy (Tonsillotomy)
Removes only the body of the tonsil down to the level of the capsular membrane, which remains attached to the pharyngeal musculature. Tonsillar tissue is removed incrementally. Theoretically decreases postoperative pain and recovery time, but carries a risk of tonsil regeneration and recurrence.
II. Conventional Surgical Techniques
1. Cold Knife (Scalpel) and Snare Method — The Oldest Technique
This is the oldest and most widely recognized method of tonsil removal.
Principle: Cold (non-electrothermal) dissection using a scalpel and a wire snare, with separate hemostasis.
Step-by-step technique:
- Patient placed supine, head hyperextended over a shoulder roll.
- Airway secured via endotracheal intubation; self-retaining mouth gag (e.g., Boyle-Davis) placed to expose tonsils.
- Posterior throat pack inserted with a retrieval string.
- Tonsil grasped at its midpoint with a curved tonsillar tenaculum and pulled medially to apply traction.
- Dissection begins superiorly: a curved tonsil knife incises along the posterolateral aspect of the anterior pillar (palatoglossus muscle) down to the muscle plane.
- A tonsil dissector bluntly dissects the tonsil from its bed, working from superior to inferior.
- The inferior pole is amputated using a tonsil snare and wire applied over the inferior pedicle.
- Hemostasis achieved by electrocautery, vasoactive topical agents, packing, or absorbable suture ligatures (0 or 2-0 plain gut on tonsil needle).
Limitation: Bleeding requires separate hemostatic measures.
2. Guillotine Method
A historical technique (now largely obsolete) using a guillotine-style instrument to rapidly amputate the tonsil. It was fast but associated with significant hemorrhage and incomplete removal.
3. Monopolar Electrocautery (Diathermy) Dissection
The most popular technique over the past 2–3 decades.
Principle: Monopolar electrosurgical current used for both dissection and hemostasis simultaneously.
Advantages:
- Greater intraoperative hemostasis
- Faster operative time
- Widely available and familiar to surgeons
Disadvantages:
- Higher thermal spread to surrounding tissue
- Associated with increased postoperative pain and longer healing/re-epithelialization times compared to cold techniques
4. Bipolar Electrocautery
Uses bipolar current, which allows precise coagulation with less lateral thermal injury than monopolar. Can be performed with bipolar bayonet forceps (with microscope) or bipolar electrosurgical scissors.
5. Cold Dissection (Classical Blunt/Sharp Dissection)
Principle: The tonsil is grasped, the anterior tonsillar pillar incised, and the capsule is dissected off the pharyngeal constrictors using blunt and sharp dissection without electrothermal energy. Hemostasis obtained by suture ligature or subsequent electrocautery.
This is the pure "cold" extracapsular technique and is the historical standard against which newer methods are compared.
III. Newer/Energy-Based Techniques (for context)
| Technique | Mechanism | Key Advantage |
|---|---|---|
| Coblation (plasma excision) | Radiofrequency energy through saline creates active protons to dissolve tissue bonds | Lower tissue temperatures (~40–70°C); reduced thermal injury |
| Harmonic Scalpel | Ultrasonic vibration breaks hydrogen bonds | Minimal thermal spread, rapid dissection |
| Microdebrider (PITA) | Powered intracapsular removal | Preserves capsule as biologic dressing; less pain and hemorrhage |
IV. Hemostasis Methods Used Alongside Dissection
- Suture ligation — traditional; 0 or 2-0 plain catgut on a tonsil needle
- Electrocautery (monopolar/bipolar)
- Vasoactive topical agents (epinephrine-soaked packs)
- Posterior pharyngeal packing
Summary Table
| Method | Energy | Plane | Hemostasis |
|---|---|---|---|
| Cold knife + snare | None (cold) | Extracapsular | Separate (suture/cautery) |
| Monopolar electrocautery | Monopolar RF | Extracapsular | Simultaneous |
| Bipolar electrocautery | Bipolar RF | Extracapsular | Simultaneous |
| Cold blunt/sharp dissection | None | Extracapsular | Suture ligature |
| Intracapsular (tonsillotomy) | Any ablative modality | Intracapsular | Incorporated |
Sources:
- Pfenninger and Fowler's Procedures for Primary Care, 3e — Chapter 83 (Types of Tonsillectomy, Cold Knife and Snare Method)
- Cummings Otolaryngology Head and Neck Surgery — Surgical Techniques section (Tonsillectomy and Adenoidectomy)
Indications of tonsillectomy
Finding Sources
Searching the Web
indications for tonsillectomy AAO-HNS clinical practice guidelines 2019
Reading File
Reading File
Reading File
Finding Sources
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.