Dermoid cyst. Advanced mrcs style information
Reading File
Finding Sources
Finding Sources
Searching the Web
dermoid cyst MRCS surgery pathology embryology complications management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching Images
dermoid cyst external angular orbital sequestration
Loading Image
Loading Image
I now have all the material needed. Here is the comprehensive MRCS-level reference on dermoid cysts:
Dermoid Cyst — Advanced MRCS Reference
Definition & Pathological Classification
A dermoid cyst is a cystic choristoma (histologically normal tissue in an abnormal location) lined by keratinising stratified squamous epithelium containing dermal appendages — hair follicles, sebaceous glands, and sweat glands — within the cyst wall. This distinguishes it from an epidermoid cyst, which lacks adnexal structures.
The contents are pultaceous (cheesy/paste-like) — a mixture of keratin, desquamated epithelium, sebum, and hair — which explains why the swelling does not transilluminate (cf. a pure fluid-filled cyst) and why fluctuation is present but translucency absent.
Classification of Dermoid Cysts
MRCS candidates must know the full classification:
| Type | Origin | Mechanism |
|---|---|---|
| Sequestration (congenital) dermoid | Entrapment of ectoderm along embryonic fusion lines | Ectoderm trapped at fusion zones during development |
| Implantation (acquired) dermoid | Surface ectoderm driven into deeper tissues by trauma | Puncture wound (needle, thorn); seen in fingers/hands |
| Tubulo-dermoid | Ectodermal entrapment around a developmental tube | E.g. post-anal dermoid |
| Teratomatous dermoid | Arises from all three germ layers | Ovarian dermoid (mature cystic teratoma) |
The most surgically relevant for MRCS is the sequestration dermoid.
Embryology (Sequestration Dermoid)
Sequestration dermoids arise at lines of embryonic fusion where two ectodermal processes meet. At these zones, ectoderm can become sequestered subcutaneously, forming a cyst lined by skin-type epithelium.
Classic sites map directly onto embryonic fusion points:
| Site | Fusion involved |
|---|---|
| External angular dermoid (outer angle of orbit) | Fronto-nasal process + maxillary process |
| Internal angular dermoid (inner canthus) | Same processes, medially |
| Post-auricular dermoid | Behind the pinna |
| Sub-lingual dermoid | Floor of mouth, midline |
| Nasal / midline scalp / frontal | Midline fusion |
| Sacrococcygeal | Post-anal midline |
| Spinal (lumbosacral) | Neural groove closure — associated with spina bifida |
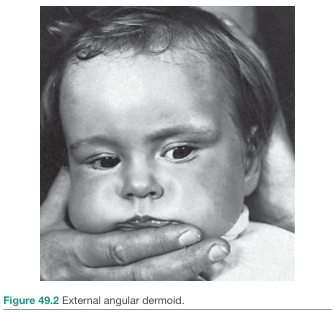
External angular dermoid — the most common site, at the outer angle of the orbit where fronto-nasal and maxillary processes fuse. (Bailey & Love's Short Practice of Surgery, 28th ed., p. 746)
Clinical Features
Examination findings (classic MRCS viva)
- Round, smooth, cystic swelling
- Fluctuation present but no transillumination (due to pultaceous contents)
- Free from overlying skin (not attached, unlike sebaceous cyst)
- Free from deeper structures (not tethered to muscle/bone except at bone margins — see below)
- Margin "yields to finger pressure" — does not slip away (cf. lipoma)
- Bony indentation may be palpable at the margin where the cyst abuts bone
- No impulse on coughing (except the rare partly intracranial type)
- Non-pulsatile, non-compressible
- Lesions present within the first year of life in most cases; 70% identified by age 5
Orbital dermoid: superficial vs deep (MRCS distinction)
| Feature | Superficial | Deep |
|---|---|---|
| Presentation | Infancy | Adolescence/adult |
| Site | Superotemporal > superonasal | Behind orbital septum |
| Clinical | Painless nodule 1–2 cm, mobile under skin, tethered to periosteum, posterior margins palpable | Proptosis, dystopia, indistinct posterior margins |
| Acute presentation | Rarely | Can rupture → inflamed orbit |
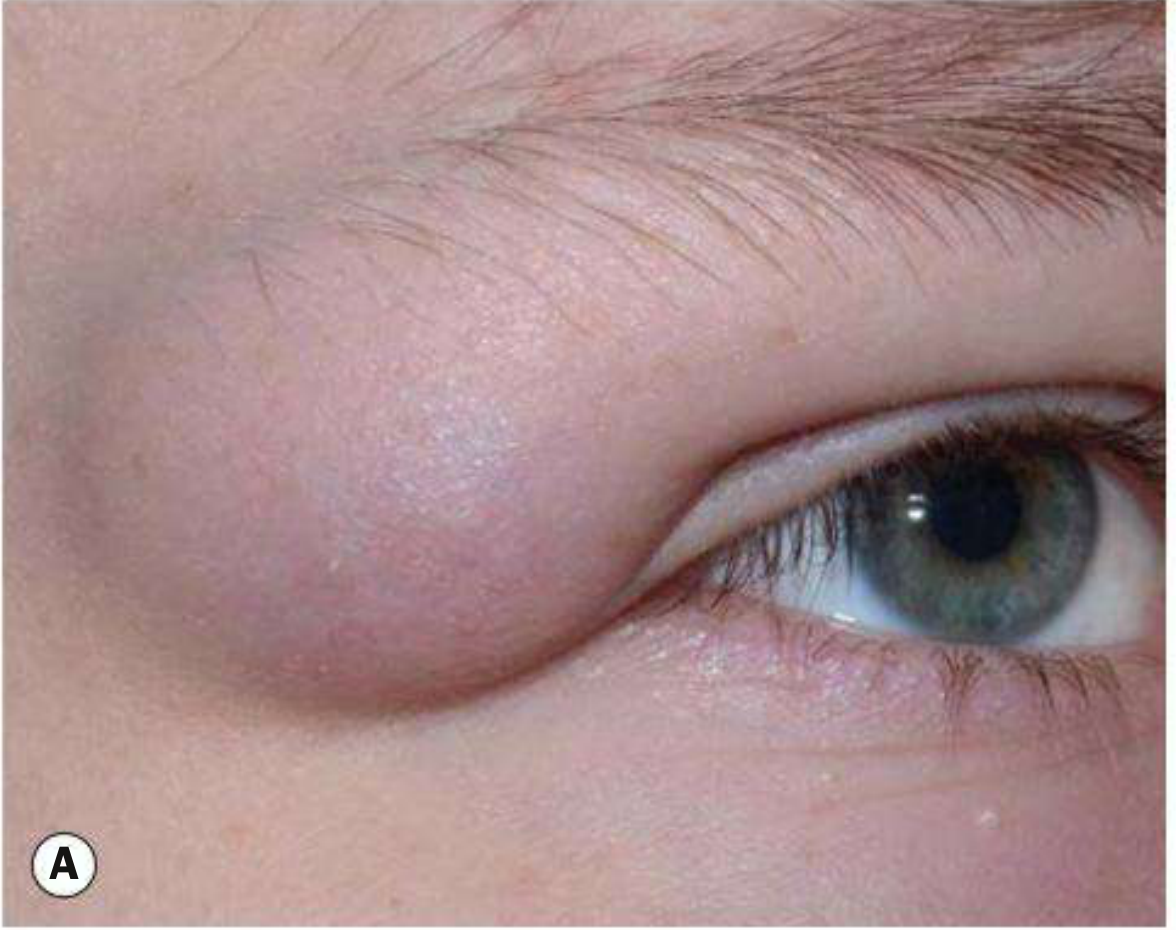
Superficial orbital dermoid (superotemporal, right eye) in a child. (Kanski's Clinical Ophthalmology, 10th ed., p. 148)
Scalp Dermoid — Important Subtypes
Dermoid cysts in the scalp can be classified by their relationship to the skull (MRCS classic):
- (a) Fully outside the skull bones
- (b) Outside skull but attached to the dura mater through a bony defect
- (c) Partly extracranial, partly intracranial — connected by a stalk (this type may elicit an impulse on coughing)
- (d) Fully intracranial (rarest) — between skull and dura
Key point: a scalp dermoid that gives an impulse on coughing implies intracranial extension — must image before excision.
Histology
- Cyst wall: keratinising stratified squamous epithelium
- Wall contains dermal appendages: hair follicles, sebaceous glands, sweat glands (absent in epidermoid cyst)
- Lining may show a wavy eosinophilic ("shark tooth") pattern resembling steatocystoma
- Contents: keratin + desquamated cells + hair + sebum
- Fibrous outer capsule — always encapsulated (benign)
Investigations
Pre-operative imaging is mandatory before excision of any midline dermoid or scalp lesion to exclude intracranial/intraspinal extension:
- CT scan — first line; shows:
- Well-circumscribed, heterogeneous cystic lesion (superficial)
- Fat-density content (hypodense on CT) — pathognomonic
- Bony scalloping/remodelling at orbital margin (chronic pressure)
- Thin sclerotic rim with occasional calcification
- MRI — mandatory if CT shows bony change; better delineates soft tissue/CNS connection
- T1: hyperintense (fat content)
- Fat-suppression sequence: signal drops out, confirming fat content
- No contrast enhancement (benign, avascular contents)
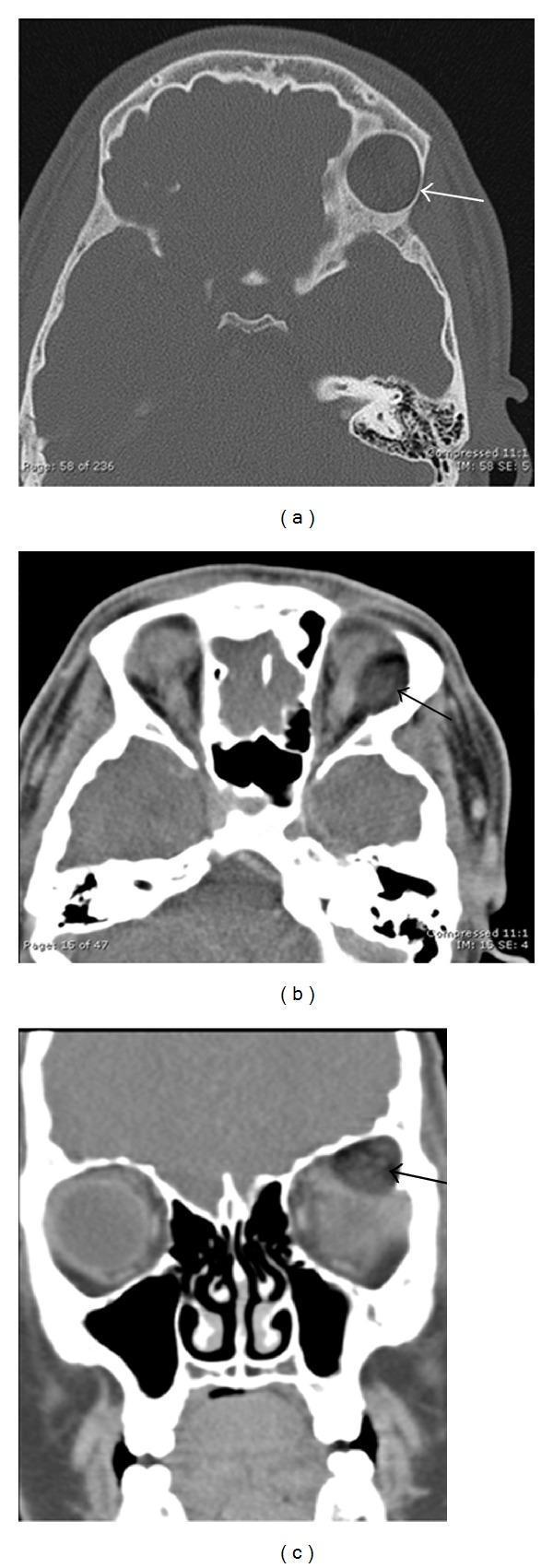
CT orbits: (a) bone window — well-circumscribed lesion at superolateral orbit with sclerotic rim and bone remodelling; (b,c) soft tissue windows — fat-density content (black arrows). Classic findings of orbital dermoid.
Needling (diagnostic puncture) can help distinguish dermoid (keratin-filled, thick contents) from thyroglossal duct cyst (mucus-filled). This is relevant for midline neck lesions.
Complications
| Complication | Mechanism | Clinical relevance |
|---|---|---|
| Infection | Secondary bacterial infection of the cyst | Presents as abscess; treat with antibiotics first, then elective excision |
| Rupture | Spontaneous or traumatic | Release of keratin/sebum → severe foreign body granulomatous inflammation |
| Intracranial/intraspinal extension | Communication via bony defect | Risk of chemical meningitis if ruptured at surgery or spontaneously |
| Spinal cord tethering | Dermoid sinus tracts in lumbosacral region | Associated with occult spinal dysraphism; late ambulatory difficulties |
| Malignant transformation | Rare | Squamous cell carcinoma in long-standing cysts |
Surgical tip (MRCS viva favourite): Never rupture a dermoid cyst during excision — keratin extruded into surrounding tissue causes intense granulomatous inflammation, making subsequent closure and healing difficult.
Differential Diagnosis
| Swelling | Key differences |
|---|---|
| Sebaceous (epidermoid) cyst | Attached to skin (punctum), no adnexal structures histologically, usually acquired |
| Lipoma | Slips away from fingers, soft, lobulated, transilluminates poorly but is compressible |
| Thyroglossal duct cyst | Elevates on tongue protrusion, moves with swallowing, midline neck, mucus-filled |
| Branchial cyst | Lateral neck, anterior to sternocleidomastoid, lined by squamous epithelium with lymphoid tissue |
| Encephalocele | Midline skull defect, pulsatile, compressible, impulse on coughing always present |
| Ranula | Floor of mouth, fluctuant, transilluminates |
Key differentiator from sebaceous cyst: dermoid is not attached to overlying skin and contains adnexal structures histologically.
Treatment
Principles
- Surgical excision is the treatment of choice — done electively
- If infected: antibiotics first, excision after resolution of acute infection
- For midline/scalp/spinal lesions: CT ± MRI to exclude intracranial/intraspinal extension before operation; if confirmed, refer to neurosurgeon
- Excise in toto — do not rupture the cyst wall
Orbital dermoid
- Superficial: excision in toto via well-planned incision; preserve periosteum; take care not to rupture
- Deep: also requires complete excision (they enlarge, may leak, and if incompletely excised recur with persistent low-grade inflammation and fibrosis)
Neck dermoid
- Simple cystectomy (no need for hyoid resection or strap muscle resection as with thyroglossal duct cyst)
- Confirmed by needle aspiration showing thick keratin material
Implantation dermoid (finger/hand)
- Simple excision under local/regional anaesthesia
Ovarian Dermoid (Mature Cystic Teratoma) — MRCS Gynaecology
This is the teratomatous dermoid and is the most common benign ovarian tumour in reproductive-age women.
- Arises from a germ cell (totipotent) that undergoes parthenogenetic development
- Karyotype: 46,XX (normal female)
- Differentiates principally along ectodermal lines: lined by squamous epithelium, contains hair, sebaceous glands, and teeth
- Can contain all three germ layers
- Gross pathology: cystic, filled with hair and sebaceous material; teeth may be present

Mature cystic teratoma (dermoid cyst) of the ovary. The ball of dark hair is classic. (Robbins & Kumar Basic Pathology)
Complications of ovarian dermoid:
- Torsion (most common surgical complication, 10–15% of cases)
- Rupture → chemical peritonitis
- Infection
- Malignant transformation (<1–2%) → squamous cell carcinoma
- Autoimmune haemolytic anaemia (rare paraneoplastic association)
Treatment: laparoscopic cystectomy (ovary-sparing); bilateral in ~10–15% of cases so inspect the contralateral ovary.
Intracranial Dermoid Cysts (Neurology/Neurosurgery)
- More common in children; tend to occur at the cerebellar vermis, parasellar/parapontine region, lumbosacral spinal canal
- Inner lining: squamous epithelium + hair follicles + skin appendages (distinguishes from epidermoid — epidermoid lacks appendages)
- Intact tumour: glistening white fibrous capsule ("pearly tumour")
- Contents if ruptured into meninges → chemical meningitis
- Sequestration cysts accompany dysraphism (spina bifida) and may communicate with skin via sinus tract
MRCS Viva High-Yield Points
- Dermoid = lined by skin-type epithelium WITH adnexal structures → distinguishes from epidermoid (no appendages) and teratoma (all 3 germ layers)
- Sequestration dermoid arises at embryonic fusion lines — know the sites (external angular is the most common)
- Fluctuant but NOT transilluminant — pultaceous contents
- Free from skin, unlike sebaceous cyst which is attached
- Bony indentation at margin when overlying bone
- Scalp dermoid with impulse on coughing = type (c) — intracranial extension — image first
- NEVER rupture during excision → granulomatous inflammation
- Midline dermoids require CT/MRI before surgery to exclude CNS communication
- Needle aspiration distinguishes dermoid (keratin) from thyroglossal cyst (mucus) in neck
- Ovarian dermoid = mature cystic teratoma — most common benign ovarian tumour in young women; main complication is torsion; malignant transformation <2%
- Rupture of intracranial/spinal dermoid → chemical meningitis
Sources:
- S Das: A Manual on Clinical Surgery, 13th ed.
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 746
- Andrews' Diseases of the Skin, Clinical Dermatology, p. 780
- Kanski's Clinical Ophthalmology, 10th ed., p. 148
- K.J. Lee's Essential Otolaryngology
- Robbins & Kumar Basic Pathology
- Bradley & Daroff's Neurology in Clinical Practice
- Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.