Necrotizing pancreatitis
Reading File
Finding Sources
Searching PubMed
"necrotizing pancreatitis"[MeSH Terms] AND management
Searching the Web
necrotizing pancreatitis management guidelines 2024 2025
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"necrotizing pancreatitis"[MeSH Terms] AND "step-up approach"
Reading File
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND "necrosectomy"
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from 6 textbooks plus an excellent treatment algorithm image. I have enough to write a thorough, well-structured answer.
Necrotizing Pancreatitis
Definition and Classification (Revised Atlanta 2012)
Necrotizing pancreatitis is a severe form of acute pancreatitis characterized by inflammation with necrosis of the pancreatic parenchyma, peripancreatic tissue, or both. It complicates approximately 20% of all acute pancreatitis cases.
Under the 2012 Revised Atlanta Classification, two distinct necrotic collections are recognized:
| Collection | Timing | CT Features | Content |
|---|---|---|---|
| Acute Necrotic Collection (ANC) | <4 weeks | No defined wall, heterogeneous | Fluid + necrosis, intra- and/or extrapancreatic |
| Walled-Off Necrosis (WON) | >4 weeks | Well-defined inflammatory wall, encapsulated | Fluid + necrosis, heterogeneous with possible loculations |
Both collections begin as sterile but may become superinfected - up to 70% of necrotic collections eventually become infected. Infection doubles the mortality rate: from ~10% for sterile necrotizing pancreatitis to ~20% for infected necrosis.
Current Surgical Therapy 14e (Table 2); ROSEN's Emergency Medicine; Fischer's Mastery of Surgery - 8th e
CT Appearances of the Four Peripancreatic Collections
The image below from Fischer's Mastery of Surgery shows the four distinct CT patterns:
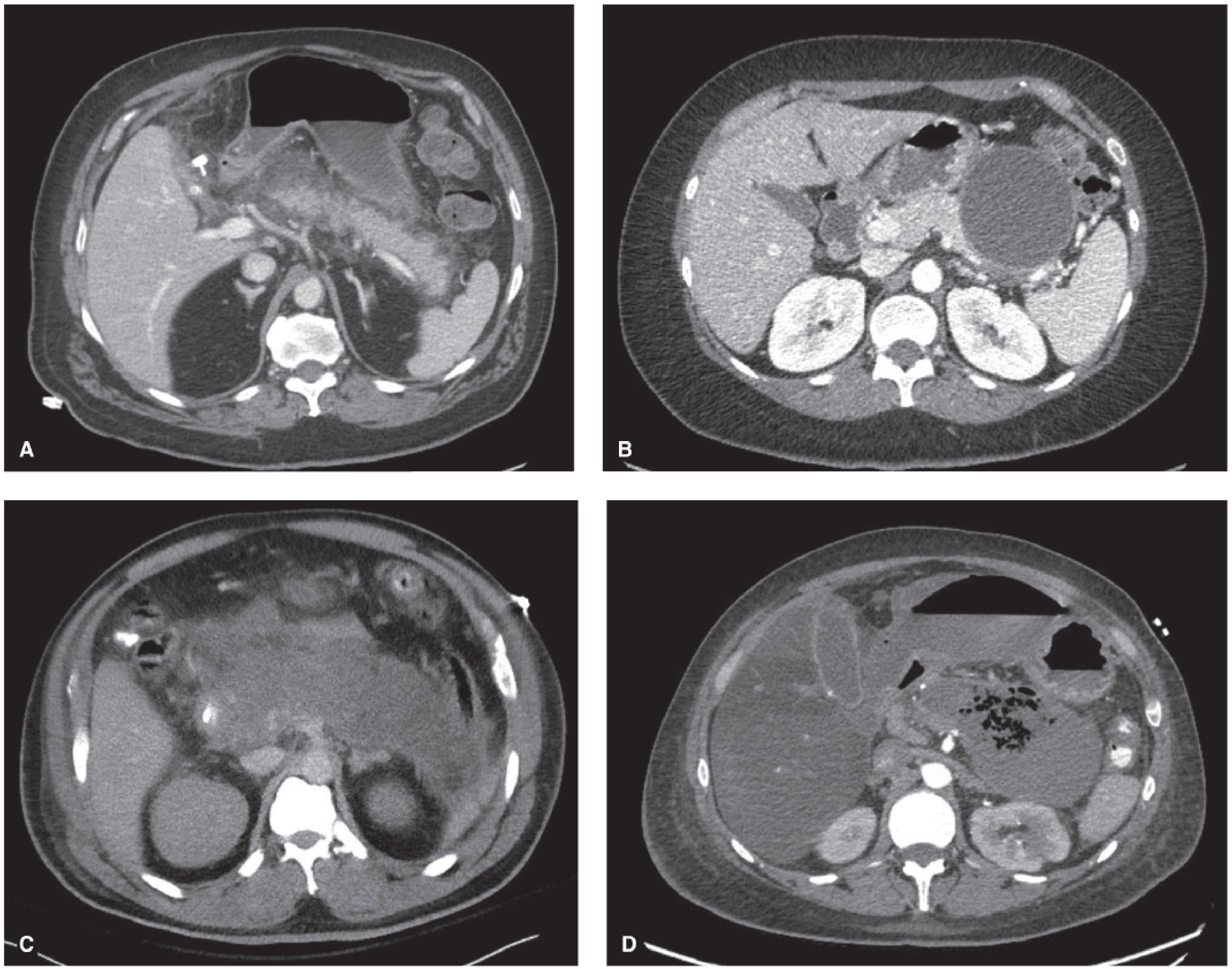
Panel C (ANC): heterogeneous collection without a defined wall, filling the lesser sac. Panel D (WON): heterogeneous collection with a well-defined encapsulating wall, containing gas (emphysematous change) indicating superinfection.
Pathophysiology
The inciting event is premature intracellular activation of digestive enzymes (trypsin) within pancreatic acinar cells. This triggers:
- Local injury: Autodigestion of pancreatic parenchyma and peripancreatic fat, releasing lipase that causes fat necrosis and calcium saponification (contributing to hypocalcemia in ~25% of patients).
- Systemic inflammatory response syndrome (SIRS): Release of TNF-α, IL-1, IL-6. Capillary leakage drives intravascular volume depletion.
- Hemoconcentration: Elevated hematocrit >44% and rising BUN are early markers of severity and predictors of necrosis.
- Organ failure: Respiratory failure (ARDS, PaO₂ <60 mmHg), renal failure (creatinine >2.0 mg/dL), and cardiovascular collapse can occur in the first 48 hours (early phase), driven by SIRS rather than infection.
- Late phase (>2 weeks): Dominated by septic complications from infected necrosis; bacteria reach the necrotic tissue primarily via bacterial translocation from the gut.
Yamada's Textbook of Gastroenterology, 7th e; Harrison's Principles of Internal Medicine 22E
Clinical Presentation and Diagnosis
Symptoms: Severe epigastric pain radiating to the back, nausea, vomiting, fever, tachycardia.
Diagnosis requires 2 of 3 criteria (Harrison's):
- Typical epigastric pain radiating to the back
- Serum lipase or amylase ≥3× upper limit of normal
- Confirmatory imaging on CT/MRI
Lab findings in severe/necrotizing disease:
- WBC 15,000-20,000/μL
- Hematocrit >44% (hemoconcentration)
- BUN >25 mg/dL on admission (strong mortality predictor; BUN AUC 0.918 in PROST trial)
- Hyperglycemia (decreased insulin + increased glucagon + glucocorticoid release)
- Hypocalcemia (~25%)
- Hyperbilirubinemia (~10%)
- ALT >3× ULN strongly suggests gallstone etiology
Imaging:
- Ultrasound: First-line; evaluates gallstones and CBD dilation but poor for necrosis
- Contrast-enhanced CT (CECT): Gold standard for necrotizing pancreatitis. Non-enhancing pancreatic parenchyma on CECT confirms necrosis. Optimal timing is 72-96 hours after onset (to allow demarcation). Gas within the collection = emphysematous/infected necrosis.
- MRI: Better differentiates solid necrotic debris from fluid (important for drainage planning)
Harrison's Principles of Internal Medicine 22E; Schwartz's Principles of Surgery 11th e
Severity Scoring
BISAP Score (within 24 hours - 1 point each):
- BUN >25 mg/dL
- Impaired mental status (GCS <15)
- SIRS present
- Age >60 years
- Pleural effusion on imaging
≥3 points = substantially increased risk for in-hospital mortality.
SOFA Score monitors ongoing organ failure (respiratory, coagulation, liver, cardiovascular, CNS, renal). A score ≥2 in any two systems = multiple organ failure.
Schwartz's Principles of Surgery 11th e; Harrison's 22E
Management
1. Resuscitation and ICU Care
- Aggressive IV fluid resuscitation: Balanced crystalloid (Lactated Ringer's preferred over normal saline). Target: falling hematocrit and BUN over first 12-24 hours, urine output >0.5 mL/kg/hr.
- ICU admission: Patients with persistent SIRS at 24 hours, elevated BISAP ≥3, organ failure, or inadequate response to initial resuscitation.
- Analgesia, bowel rest initially, then early enteral nutrition (nasojejunal feeding preferred - reduces infectious complications, maintains gut barrier integrity).
2. Nutrition
Early enteral nutrition (within 24-48 hours) via nasojejunal tube is preferred over parenteral nutrition. However, the PYTHON trial showed early forced enteral tube feeding did not reduce infection rates compared to on-demand feeding (25% vs 26%).
3. Antibiotics
- Prophylactic antibiotics are NOT recommended - multiple well-designed RCTs show they do not reduce infectious complications, need for surgery, or death. Overuse drives fungal infections and resistant organisms.
- Therapeutic antibiotics ARE indicated for confirmed or strongly suspected infected necrosis. Agents that penetrate pancreatic necrosis include carbapenems, fluoroquinolones, and metronidazole.
- CT-guided fine-needle aspiration (FNA) with Gram stain and culture is used to confirm infection when clinical status is unclear (sensitivity/specificity mid-90% range). Not recommended routinely due to false-negative risk and theoretical risk of introducing infection.
4. Biliary Etiology
- Cholangitis + biliary obstruction: ERCP within 24-48 hours.
- Gallstone pancreatitis without cholangitis: Early ERCP has no benefit (stone usually passes spontaneously). Cholecystectomy during the same admission in mild disease; delayed in severe disease after recovery.
5. Management of Infected/Symptomatic Necrosis - The "Step-Up" Approach
The current paradigm is a minimally invasive step-up approach, deferring intervention as long as possible to allow demarcation (preferably ≥4 weeks). Early surgery carries extremely high perioperative mortality.
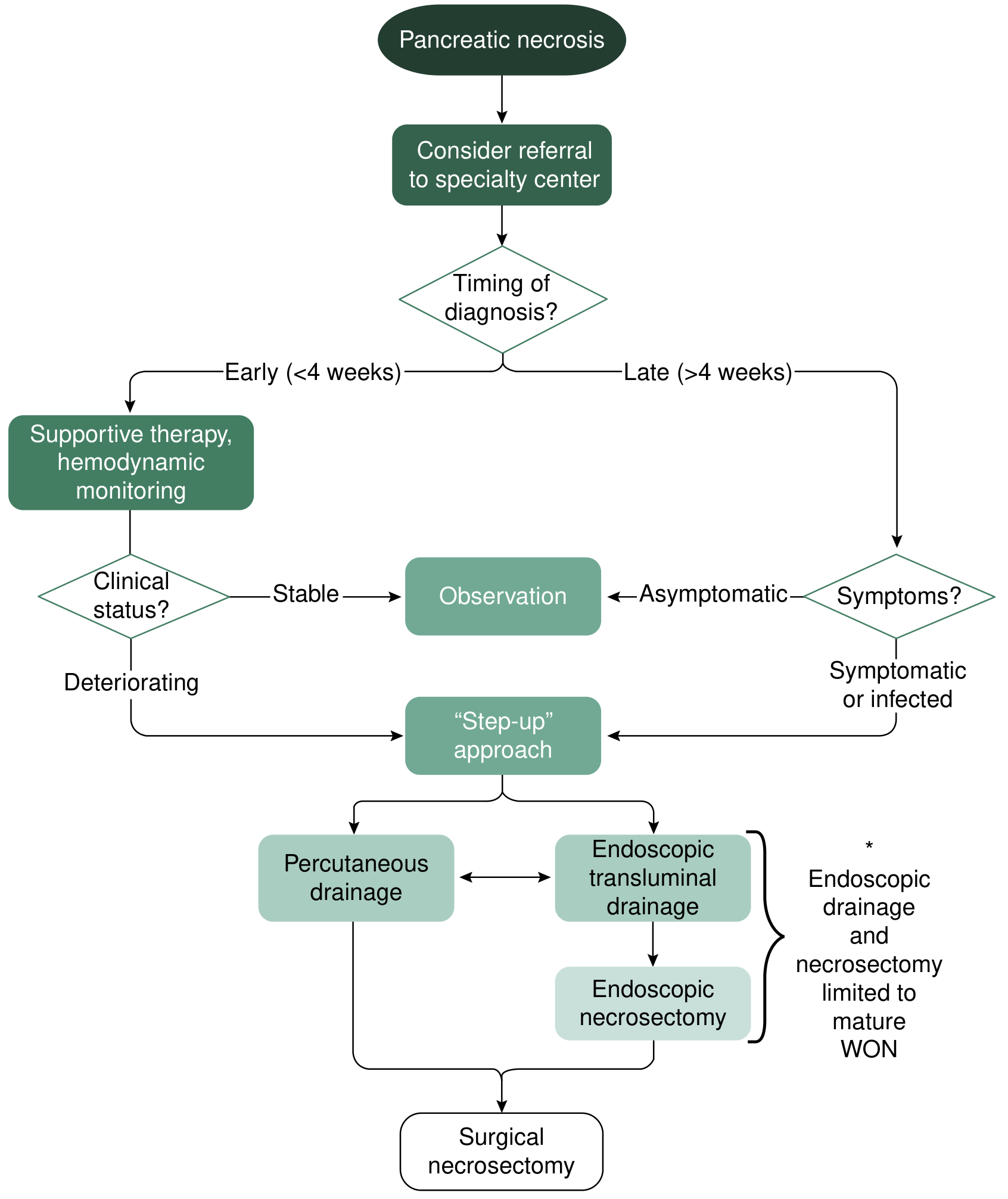
Step 1 - Percutaneous drainage (PD):
- First-line for infected necrosis or ANC with clinical deterioration
- Image-guided by interventional radiology (IR)
- Retroperitoneal access preferred to allow potential VARD
- Serial catheter upsizing + intracatheter irrigation with saline/H₂O₂
- Best for collections extending to retroperitoneum or paracolic gutters
- Up to 50% of patients managed with PD alone, avoiding necrosectomy
- Risk: pancreaticocutaneous fistula if communicating with pancreatic duct
Step 2 - Endoscopic drainage and necrosectomy:
- Best for mature WON within 2 cm of stomach or duodenum
- Requires ≥4 weeks from onset for wall maturation
- EUS-guided cystgastrostomy → balloon dilation → pigtail stents or lumen-apposing metal stents (LAMS)
- Direct endoscopic necrosectomy (DEN): endoscope inserted into collection, mechanical debridement
- PENGUIN trial (Dutch Acute Pancreatitis Study Group): endoscopic necrosectomy vs. surgical necrosectomy - significantly fewer major complications/death, fewer pancreatic fistulas, less new organ failure
- Up to two-thirds of patients avoid operative debridement with endoscopic necrosectomy
Step 3 - Video-Assisted Retroperitoneal Debridement (VARD):
- If percutaneous drainage fails but complete surgical necrosectomy not needed
- The PANTER trial: step-up approach (PD → VARD) vs. primary open surgical necrosectomy - step-up had significantly fewer complications and less new-onset organ failure
Step 4 - Surgical necrosectomy (open or laparoscopic):
- Reserved for failure of all minimally invasive approaches
- Indications per Maingot's Abdominal Operations:
- Diagnostic uncertainty / concurrent intra-abdominal catastrophe
- Infected necrosis documented by FNA or extraluminal gas on CT
- Severe sterile necrosis with persistent organ failure (ideally ≥2 weeks from onset)
- Symptomatic organized pancreatic necrosis ("persistent unwellness")
- Delayed surgery (>4 weeks) significantly better than early surgery - allows demarcation, reduces bleeding risk and collateral organ damage
Current Surgical Therapy 14e; Maingot's Abdominal Operations; Yamada's Textbook of Gastroenterology 7th e; Schwartz's Principles of Surgery 11th e
Complications
| Complication | Details |
|---|---|
| Infected necrosis | Most common cause of death; near-100% mortality without intervention |
| Pancreatic fistula | Communication with pancreatic duct - complicates drainage |
| Pseudoaneurysm | Splenic artery most common; presents as GI bleed or hemosuccus pancreaticus |
| Colonic necrosis | Transverse colon most vulnerable; presents as peritonitis |
| Abdominal compartment syndrome | Massive fluid resuscitation → raised intra-abdominal pressure |
| ARDS | PaO₂ <60 mmHg; ~5-10% of cases |
| Exocrine/endocrine insufficiency | Post-necrotizing pancreatitis diabetes and steatorrhea |
| Chronic pancreatitis | Postnecrotic fibrosis and ductal stricturing |
Prognosis
- Sterile necrotizing pancreatitis: ~10% mortality
- Infected necrotizing pancreatitis: ~20% mortality (effectively 100% without intervention)
- Patients who survive severe necrotizing pancreatitis are at risk for post-necrotizing chronic pancreatitis, as noted in Harrison's (TIGAR-O classification: "Postnecrotic - severe acute pancreatitis")
2025 IAP/APA Guidelines Update: The International Association of Pancreatology 2025 guidelines (PMID 40651900) represent the most current evidence-based recommendations, covering 96 questions across 18 domains including fluid therapy, nutritional support, conservative and interventional treatment of infected necrotizing pancreatitis, discharge criteria, and prevention of recurrence.
This is a shared conversation. Sign in to Orris to start your own chat.