Leptospirosis
Reading File
Finding Sources
Searching PubMed
leptospirosis
Searching the Web
leptospirosis 2025 clinical features diagnosis treatment guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I have all the information needed for a comprehensive answer. Let me now compile it.
Leptospirosis
The Pathogen
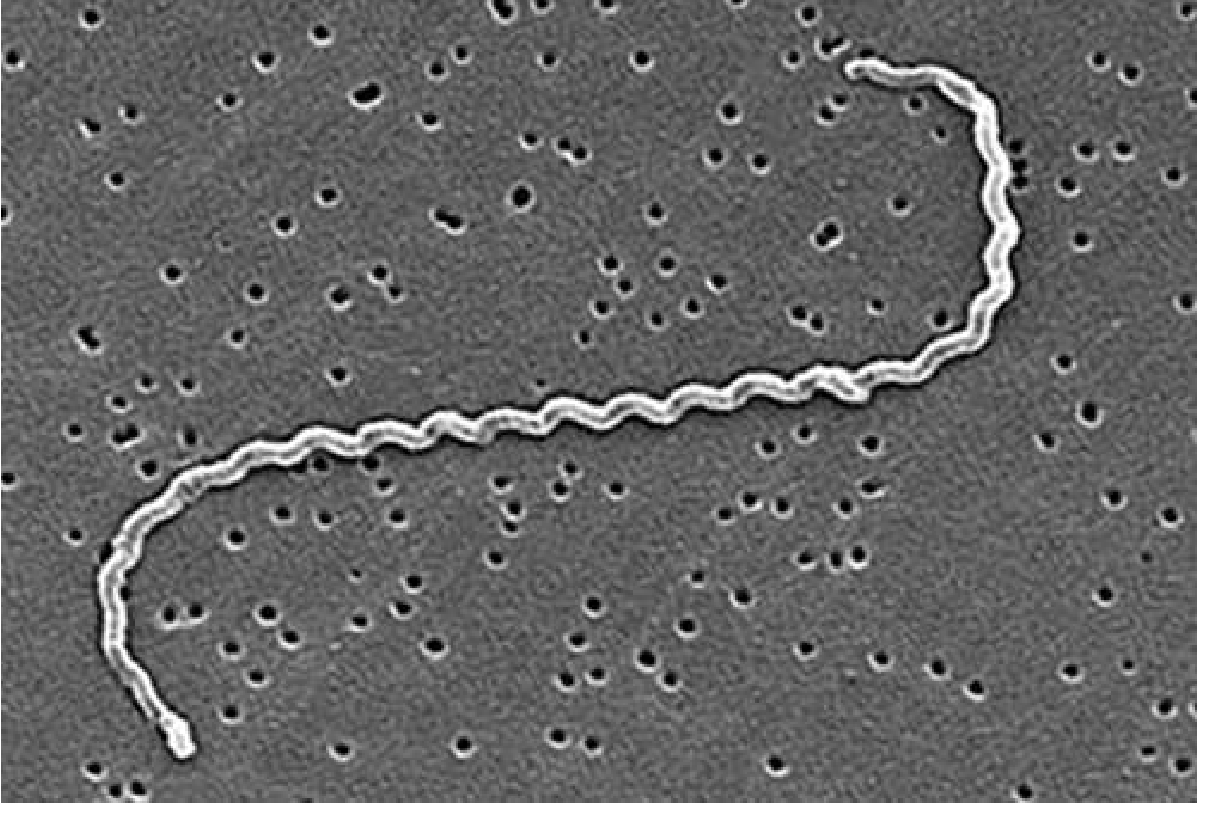
Leptospirosis is a zoonotic infection caused by pathogenic spirochetes of the genus Leptospira. The organisms are 0.1 µm in diameter and 6-20 µm long, with a characteristic hooked trailing end that gives L. interrogans (the most common human pathogen) its name - from Latin interrogans ("question mark" shape). There are over 25 serogroups and 250 serovars, differing by geography and host specificity. The most virulent serovar in humans is Icterohaemorrhagiae, typically carried by rats. - Goldman-Cecil Medicine, p. 3243
Epidemiology
Leptospirosis is the most widespread zoonosis globally, causing approximately 1 million clinical infections and 60,000 deaths annually - numbers that are likely underestimates due to misdiagnosis as dengue, malaria, or influenza. Endemic in tropical developing countries (India, Malaysia, Brazil), it is predominantly a disease of poverty linked to poor urban flood control and rodent access to human living spaces.
Transmission routes:
- Contact with water or soil contaminated by infected animal (especially rodent) urine - the most common route
- Direct contact with infected animals (farmers, veterinarians, slaughterhouse workers at occupational risk)
- Entry via abraded skin, conjunctiva, or oral mucous membranes
- Human-to-human transmission is rare
The urban brown rat (Rattus norvegicus) is the primary reservoir, acquiring L. interrogans serovar Icterohaemorrhagiae early in life and persistently shedding it in urine. Cases spike dramatically after heavy rainfall and flooding. Adventure travelers (e.g., white water kayaking, jungle trekking) are also at risk. - Goldman-Cecil Medicine, p. 3243; Sherris & Ryan Medical Microbiology, p. 1424
Pathobiology
Leptospires penetrate skin abrasions or mucous membranes and disseminate hematogenously to all organs including the kidneys, liver, lungs, and CNS. Key immune evasion mechanisms include:
- Binding complement regulators on their surface proteins, rendering them resistant to complement-mediated killing
- Binding lipopolysaccharide and peptidoglycan to shield these from innate immune detection
- Disrupting endothelial cell junctions, facilitating tissue barrier penetration
The disease is classically biphasic:
| Phase | Timing | Pathology |
|---|---|---|
| Leptospiremic phase | Days 1-7 | Bacteremia; organisms in blood, urine, CSF |
| Immune phase | Week 2 onwards | Agglutinating antibodies rise; organisms cleared from blood; immune-mediated organ damage |
Renal injury is caused by proximal tubular colonization, leading to decreased expression of sodium/water transporter proteins, potassium wasting, and inability to concentrate urine. Histology shows acute interstitial nephritis with mononuclear cell infiltration. Hepatic damage occurs from leptospires in hepatic sinusoids causing bile leakage and jaundice. Pulmonary hemorrhage results from disruption of the alveolar-capillary barrier combined with thrombocytopenia and coagulation disorders. - Goldman-Cecil Medicine, p. 3243
Clinical Manifestations
The incubation period is 6-29 days (median 15 days).
Most infections (~90%) are mild and self-limited or even asymptomatic. About 10% develop severe (Weil) disease.

Mild Leptospirosis (Anicteric)
- Abrupt-onset fever, chills, rigors (75-100%)
- Severe bitemporal/frontal throbbing headache with retro-orbital pain and photophobia
- Myalgia - characteristically involves calves and lower back
- Conjunctival suffusion - pathognomonic red injection of the conjunctiva WITHOUT discharge or exudate
- Nausea, vomiting, diarrhea, abdominal pain (~35-45%)
- Non-productive cough (~50%)
- Maculopapular erythematous rash, often pretibial
Severe Leptospirosis - Weil Disease (Icteric)
The classic Weil's triad: jaundice + acute renal failure + bleeding

- Jaundice (hyperbilirubinemia occurs in 85% of severe cases)
- Acute kidney injury (AKI) - present in 44-67% of patients; characteristically non-oliguric with hypokalemia
- Hemorrhage - usually mild petechiae/ecchymoses; severe gastrointestinal or pulmonary hemorrhage in some (Weil-Larrey syndrome = severe pulmonary hemorrhage syndrome, ARDS, high mortality)
- Aseptic meningitis - organisms in CSF during leptospiremic phase even without symptoms
- Cardiac arrhythmias (myocarditis)
- Uveitis (can occur weeks after acute illness)
- Multiorgan failure
Mortality in Weil disease can reach 10%. - Goldman-Cecil Medicine, p. 3244; Sherris & Ryan, p. 1425
Renal Pathology
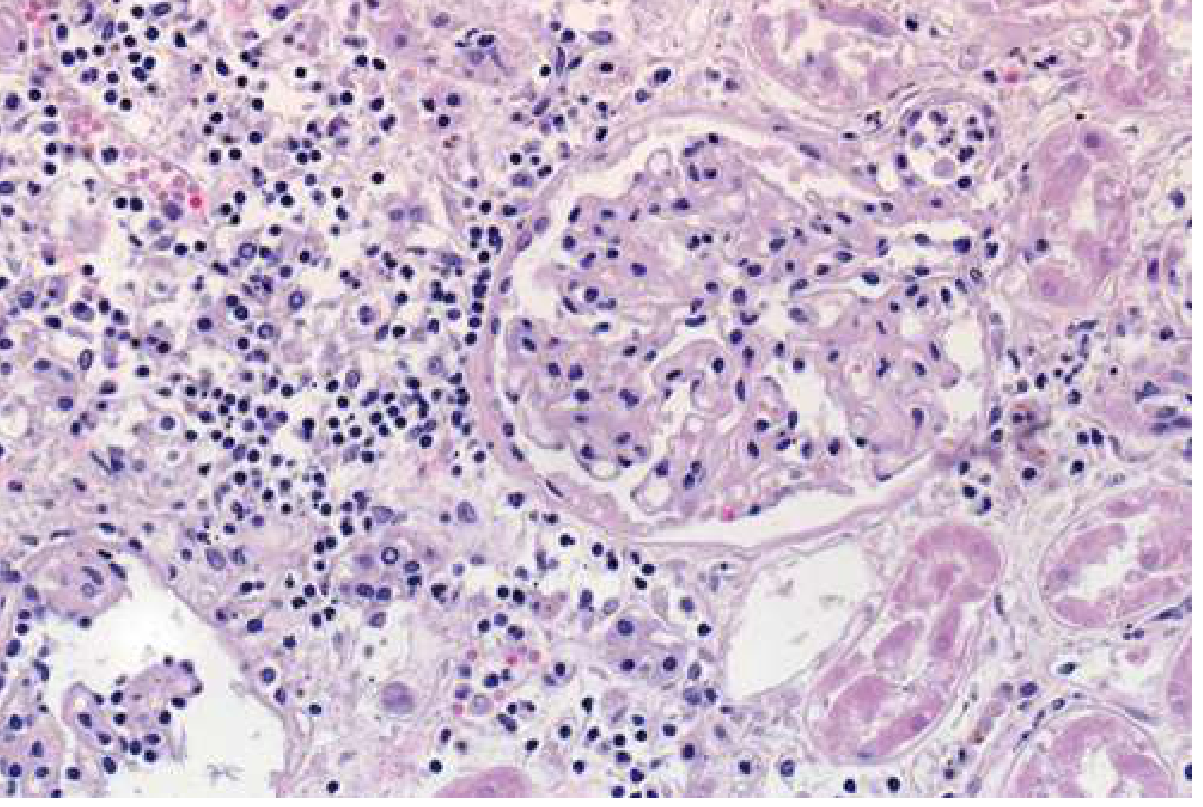
The hallmark renal lesion is acute tubulointerstitial nephritis with:
- Dense mononuclear infiltrate (lymphocytes/macrophages), diffuse or perivascular
- Acute tubular necrosis (direct leptospiral toxicity + ischemia)
- Leptospires visible throughout tubular basement membranes on silver staining
- Glomeruli typically spared (minimal glomerular changes)
The AKI is typically non-oliguric - a distinguishing feature. Profound hypokalemia occurs due to tubular potassium wasting. Hemodialysis or hemofiltration is superior to peritoneal dialysis in leptospirosis-associated AKI. - Brenner & Rector's The Kidney, p. 3266; A 2025 systematic review (PMID 40111731) confirms kidney involvement is the most clinically significant complication.
Diagnosis
Case Definitions (WHO)
| Category | Criteria |
|---|---|
| Suspect | Fever ≥38.5°C + headache + myalgia + prostration/conjunctival suffusion + history of exposure |
| Probable (clinical) | Suspect + any 2 of: calf tenderness, cough ± hemoptysis, SOB, rash, jaundice, hemorrhage, meningism, oliguria/proteinuria, arrhythmia |
| Probable (lab) | Suspect + positive rapid IgM + any 3 of: proteinuria/pyuria/hematuria; neutrophilia >80%; platelets <100,000/µL; elevated bilirubin >2mg/dL |
| Confirmed | Suspect/Probable + culture, PCR, seroconversion, or MAT titer ≥400 |
Diagnostic Tests
| Test | Timing | Notes |
|---|---|---|
| PCR (blood/urine/CSF) | First week (leptospiremic phase) | Highest sensitivity for early diagnosis; preferred |
| MAT (microscopic agglutination test) | Requires 2 samples 2 weeks apart | Gold standard for confirmation; 4-fold titer rise diagnostic; reference labs only |
| Rapid IgM ELISA | From day 5-7 | Lower sensitivity first week; practical point-of-care test |
| Blood culture | First 7-10 days | Very slow growth (weeks); rarely practical |
| Urine culture | After day 10 | Organisms shed in urine in immune phase |
| Darkfield microscopy | Not recommended | Very low yield; confusion with debris |
- Goldman-Cecil Medicine, p. 3244; Sherris & Ryan, p. 1425
Treatment
Mild-Moderate Disease
- Doxycycline 100 mg PO twice daily x 7 days (drug of choice)
- Azithromycin (alternative)
- Amoxicillin (alternative)
Doxycycline shortens illness by ~2 days and prevents urinary organism shedding.
Severe Disease (Weil)
- Penicillin G IV 1,500,000 units every 6 hours x 7 days (traditional standard)
- Ceftriaxone IV 1 g once daily x 7 days (equivalent efficacy to penicillin; often preferred)
- Cefotaxime IV 1 g every 6 hours x 7 days (alternative)
Supportive Care
- Aggressive IV fluid resuscitation for non-oliguric renal failure + potassium supplementation
- Hemodialysis (preferred) or peritoneal dialysis for oliguric renal failure
- Management of pulmonary hemorrhage (mechanical ventilation in severe ARDS)
- Correction of coagulopathy
Note: Antimicrobials are less effective when started during the immune phase (week 2+), as organ damage at that stage has an immunopathological component.
- Brenner & Rector's The Kidney, p. 3266; Goldman-Cecil Medicine, p. 3244
Prevention
| Strategy | Details |
|---|---|
| Chemoprophylaxis | Doxycycline 200 mg once weekly for high-risk short-term exposures (jungle trekking, kayaking in endemic areas) |
| Personal protection | Waterproof boots and gloves; cover skin abrasions |
| Environmental | Rodent control; drainage of contaminated water sources |
| Veterinary vaccination | Available for cattle, dogs, pigs - reduces human risk |
| Human vaccine | Available in some countries (Cuba, China, France) for specific serovars; not universally available |
Key Points at a Glance
- Leptospirosis is caused by Leptospira interrogans, a spirochete spread via rodent/animal urine-contaminated water
- ~1 million cases/60,000 deaths annually; grossly underdiagnosed
- Classic biphasic illness: leptospiremic phase (fever, myalgia, conjunctival suffusion) → immune phase (organ damage)
- Weil disease = jaundice + AKI (non-oliguric, hypokalemic) + hemorrhage - ~10% of cases
- Conjunctival suffusion without discharge is pathognomonic
- Diagnosis: early PCR is best; MAT is the gold standard (paired sera); rapid IgM for field use
- Treatment: doxycycline (mild) or IV ceftriaxone/penicillin (severe) x 7 days
- A 2025 systematic review on kidney involvement (PMID 40111731) confirms AKI is the dominant life-threatening complication
Sources: Goldman-Cecil Medicine (27th ed.), Brenner & Rector's The Kidney, Sherris & Ryan's Medical Microbiology (8th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.