Endometriosis
Reading File
Finding Sources
Searching PubMed
"endometriosis"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content and all key images. Let me compile the full answer.
Endometriosis
Definition
Endometriosis is a common chronic inflammatory condition defined by the presence of endometrial glands and stroma in extrauterine locations. It affects an estimated 5-10% of women of reproductive age and is found in nearly half of women with infertility.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Robbins & Kumar Basic Pathology
Types
Three distinct subtypes are recognized:
| Type | Description |
|---|---|
| Superficial peritoneal endometriosis | Small implants on serosal/peritoneal surfaces |
| Ovarian endometriosis (endometriomas) | Cystic lesions filled with old blood ("chocolate cysts"); reported in 17-44% of cases |
| Deep infiltrating endometriosis | Tissue >5 mm beneath the peritoneum; involves uterosacral ligaments, vagina, bowel, bladder, ureters |
Risk of malignant transformation is mainly confined to the deep infiltrating type.
Pathogenesis
The exact mechanism remains elusive. Four leading theories are proposed:
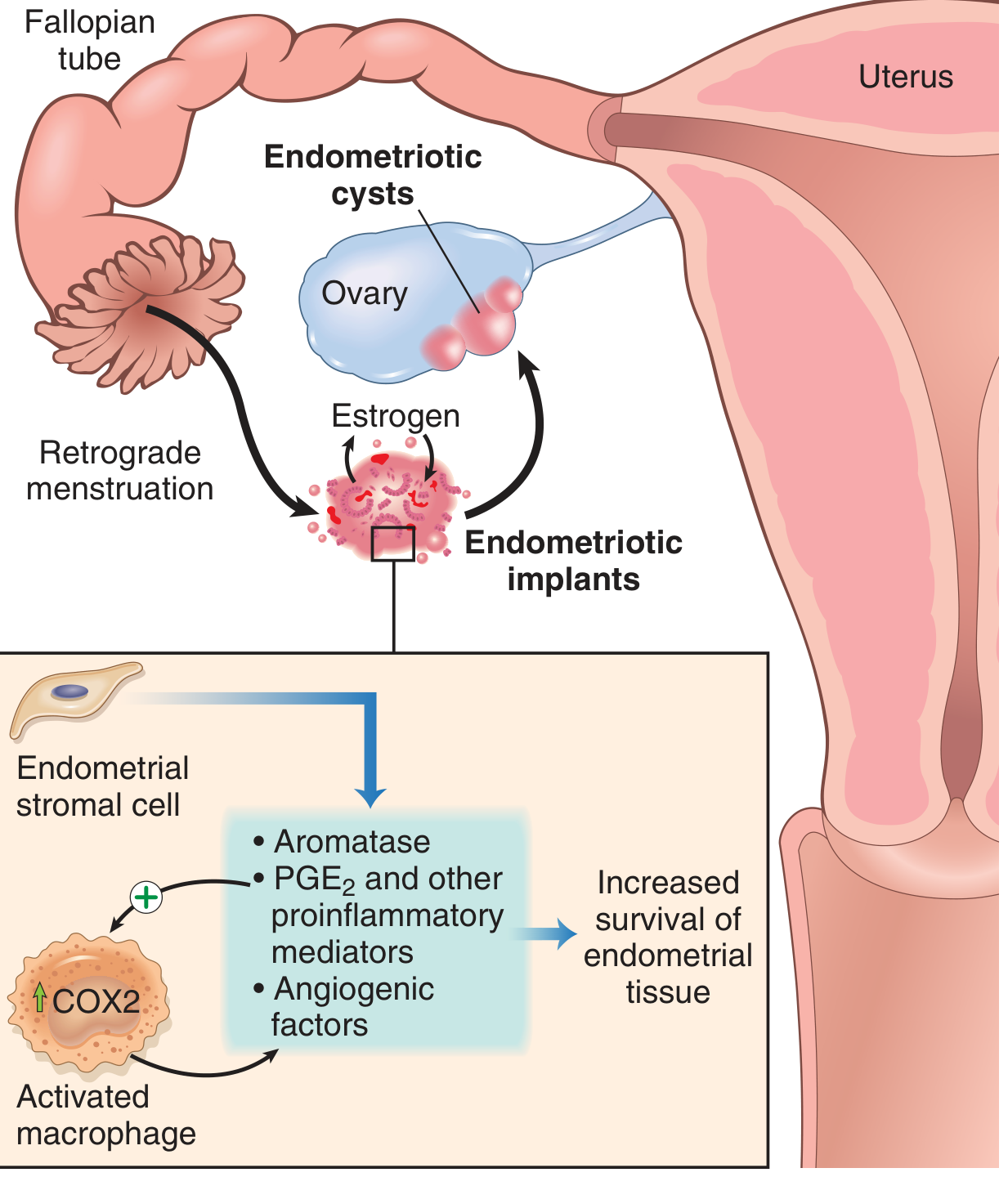
Pathogenesis of endometriosis - Robbins & Kumar Basic Pathology, Fig. 17.9
- Regurgitation theory (most widely accepted): retrograde flow of menstrual endometrium through the fallopian tube implants at ectopic pelvic sites.
- Benign metastasis theory: endometrial tissue spreads to distant sites (bone, lung, brain) via blood vessels and lymphatics.
- Metaplastic theory: coelomic epithelium (mesothelium) undergoes metaplasia into endometrial tissue - explains extraperitoneal sites.
- Extrauterine stem/progenitor cell theory: bone marrow-derived stem cells differentiate into endometrial tissue.
Why implants persist
Endometriotic stromal cells produce high levels of aromatase, leading to increased local estrogen synthesis from androgens - creating a self-sustaining estrogen-rich microenvironment. Implants also express elevated PGE2, VEGF, and MMPs, partly released by recruited macrophages (via COX-2), promoting survival, angiogenesis, and invasion.
Sites of Involvement
Common pelvic sites:
- Ovaries (most common)
- Pouch of Douglas
- Uterosacral ligaments
- Fallopian tubes
- Peritoneum / pelvic sidewall
Extrapelvic sites (less common):
- GI tract: sigmoid colon and small bowel loops in 12-37% of cases; cecum also affected
- Bladder, ureters
- Lungs (causing catamenial hemoptysis or recurrent pneumothoraces at time of menstruation)
- Periumbilical tissues, laparotomy scars
- Rarely: bone, brain
Gross and Microscopic Appearance
Typical ("powder burn") lesions:
- Black, dark brown, or bluish puckered nodules on ovaries, serosal surfaces, and peritoneum
- Represent old hemorrhage surrounded by fibrosis
Atypical / "subtle" lesions:
- Red implants (petechial, vesicular, polypoid, red flame-like)
- Serous or clear vesicles
- White plaques/scarring
- Yellow-brown peritoneal discoloration
Endometriomas ("chocolate cysts"):

Ovarian endometrioma - Robbins & Kumar Basic Pathology, Fig. 17.10
- Cystic masses 3-5 cm in diameter, filled with thick dark brown fluid ("tar-like")
- Densely adherent to peritoneum of the ovarian fossa, fallopian tube, and posterolateral uterus
- Distinguishable from simple hemorrhagic ovarian cysts by their adherence pattern
Microscopically: functioning endometrial glands + stroma undergoing cyclic bleeding, with hemosiderin deposition and fibrous adhesions. Diagnosis requires both glands and stroma at ectopic sites.
Clinical Features
Cardinal symptoms (the "4 Ds"):
- Dysmenorrhea - pain related to menstruation (most common symptom)
- Dyspareunia - deep pain during intercourse
- Dyschezia - pain on defecation (with bowel involvement)
- Dysuria - pain on urination (with bladder involvement)
Other symptoms:
- Chronic pelvic pain (cyclical and non-cyclical)
- Infertility - presenting complaint in 30-40% of patients
- Fatigue
- Rectal bleeding (haematochezia), hematuria
- A significant proportion remain asymptomatic
Important caveat: There is little correlation between the extent/severity of disease on classification systems and the type or severity of symptoms experienced.
Diagnosis
Gold standard: Laparoscopy with histological confirmation
Non-invasive imaging:
- Transvaginal/transrectal ultrasound: reliable only for severe forms (endometriomas, deep pelvic endometriosis)
- MRI: can detect hemosiderin deposits in abdominal organs; demonstrates low-signal fibrotic plaques; increasingly used for deep disease
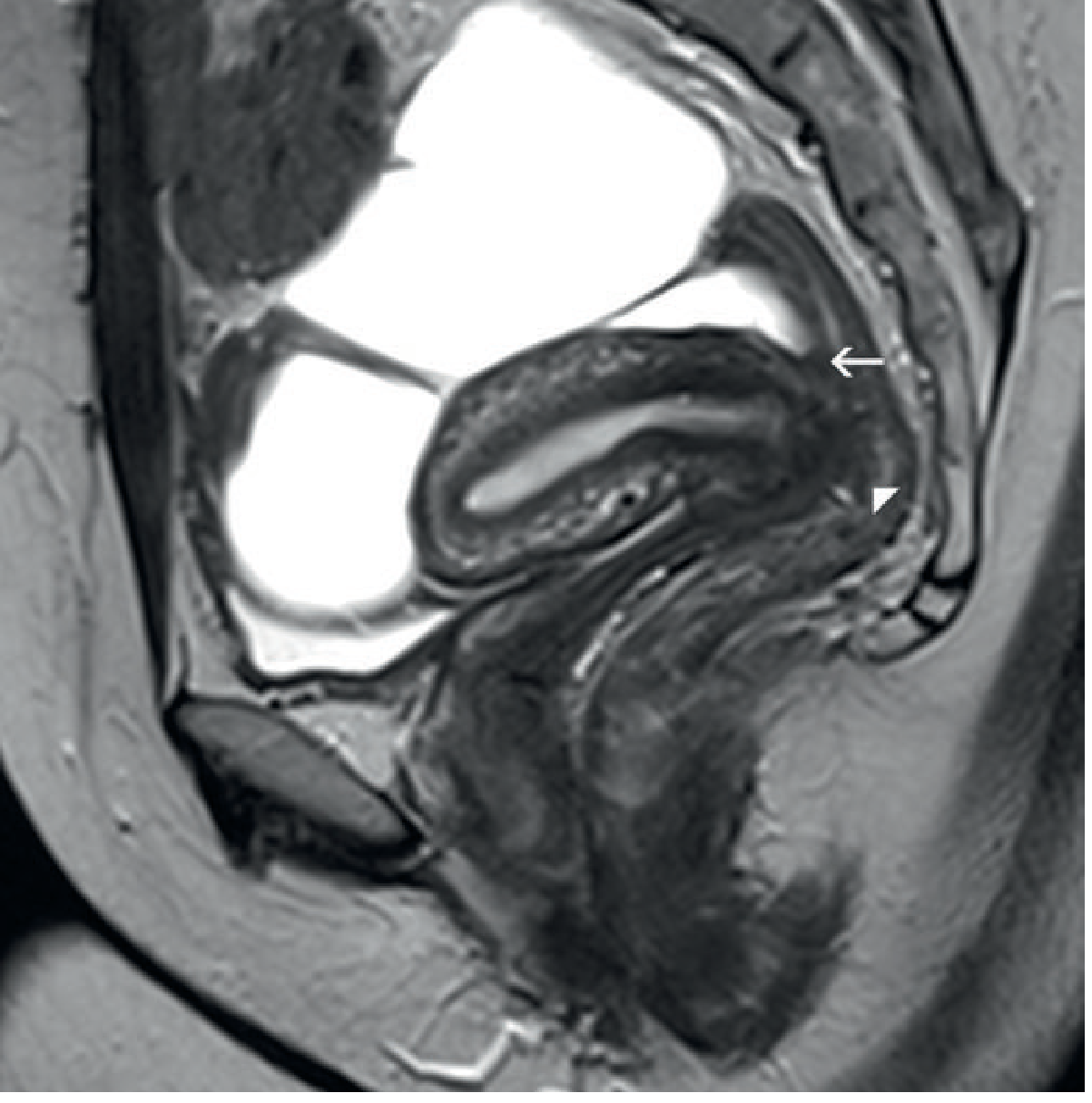
MRI pelvis - deep rectovaginal endometriosis obliterating the pouch of Douglas - Grainger & Allison's Diagnostic Radiology
- Sigmoidoscopy: useful for assessing level of bowel involvement; distance of rectal lesion from anal verge affects surgical planning (lesions 5-8 cm from the anal verge carry higher risk of anastomotic leak)
- Serum CA-125 is neither sensitive nor specific enough for routine diagnosis
Management
Medical (hormonal suppression - estrogen-dependent disease)
| Drug Class | Examples | Mechanism |
|---|---|---|
| Combined OCP | Ethinylestradiol/levonorgestrel | Suppresses ovulation, induces pseudopregnancy |
| Progestogens | Norethisterone, Medroxyprogesterone, Levonorgestrel IUS | Decidualization and atrophy of implants |
| GnRH agonists | Leuprorelin, Goserelin | Medical castration; hypoestrogenic state |
| GnRH antagonists | Elagolix | Rapid FSH/LH suppression |
| Danazol | Synthetic androgen/antigonadotropin | Androgenic/anabolic state, suppresses LH surge |
| COX-2 inhibitors | Celecoxib | Reduce PGE2, anti-inflammatory |
| Aromatase inhibitors | Letrozole, Anastrozole | Block local estrogen production in implants |
All medical treatments are suppressive, not curative - symptoms typically return after stopping treatment.
Surgical
Indications: failed medical therapy, desire for fertility, severe or deep disease, diagnostic uncertainty
- Conservative surgery (laparoscopy): excision or ablation of endometriotic lesions, lysis of adhesions, cystectomy for endometriomas - preferred approach for fertility preservation
- Bowel surgery: segmental resection, rectal shaving, disc excision for deep bowel endometriosis; low rectal lesions (5-8 cm from anal verge) carry higher risk of anastomotic leak and transient neurogenic bladder dysfunction
- Definitive surgery: hysterectomy ± bilateral salpingo-oophorectomy for women who have completed their families with severe refractory disease
Complications
- Infertility (mechanism: adhesions distorting tubo-ovarian anatomy, impaired folliculogenesis, altered peritoneal environment)
- Extensive fibrous adhesions obliterating the pouch of Douglas
- Bowel obstruction / ureteral obstruction
- Malignant transformation - rare; mainly from deep infiltrating endometriosis (clear cell and endometrioid carcinomas)
- Recurrent pneumothorax / catamenial hemoptysis (thoracic endometriosis)
Recent Evidence (2024-2026)
Three recent systematic reviews are worth noting:
- Fibrosis in endometriosis (PMID 39067455): A 2024 systematic review in Human Reproduction Update identifies fibrosis as a key driver of deep infiltrating endometriosis and pain - a potential therapeutic target beyond hormonal suppression.
- Diagnosis delay (PMID 39373298): A 2025 systematic review in BJOG confirms persistent diagnostic delays of 6-8+ years globally, with significant regional variation - underscoring the importance of clinical suspicion.
- Exercise and physical activity (PMID 39946383): A 2025 meta-analysis finds physical activity reduces pain and improves quality of life in women with endometriosis, supporting its role as an adjunct to medical/surgical care.
Sources: Bailey and Love's Short Practice of Surgery (28th Ed.) | Robbins & Kumar Basic Pathology | Grainger & Allison's Diagnostic Radiology
In detail acute congestive glaucoma for opthalmology Final mbbs?students
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive, detailed content from Kanski's Clinical Ophthalmology, Rosen's Emergency Medicine, and Goldman-Cecil Medicine. Let me now compile the complete Final MBBS-level answer.
Acute Congestive Glaucoma (Acute Primary Angle-Closure Glaucoma)
Ocular Emergency - requires immediate treatment to prevent permanent blindness
Definition
Acute congestive glaucoma (now formally called Acute Primary Angle Closure - APAC) is a sudden, dramatic rise in intraocular pressure (IOP) caused by occlusion of the trabecular meshwork by the peripheral iris (iridotrabecular contact - ITC), which obstructs aqueous outflow. It was historically called "acute glaucoma" and remains the classic ophthalmic emergency tested in Final MBBS.
- Kanski's Clinical Ophthalmology, 10th Ed.
Aqueous Humor Physiology (Essential Background)
Aqueous humor is produced by the ciliary processes, passes from the posterior chamber → anterior chamber through the pupillary aperture, then drains through the trabecular meshwork → Canal of Schlemm → episcleral veins.
Normal IOP = 10-20 mmHg. Any obstruction to outflow raises IOP dramatically.
Anatomy of the Angle - Shaffer Grading System
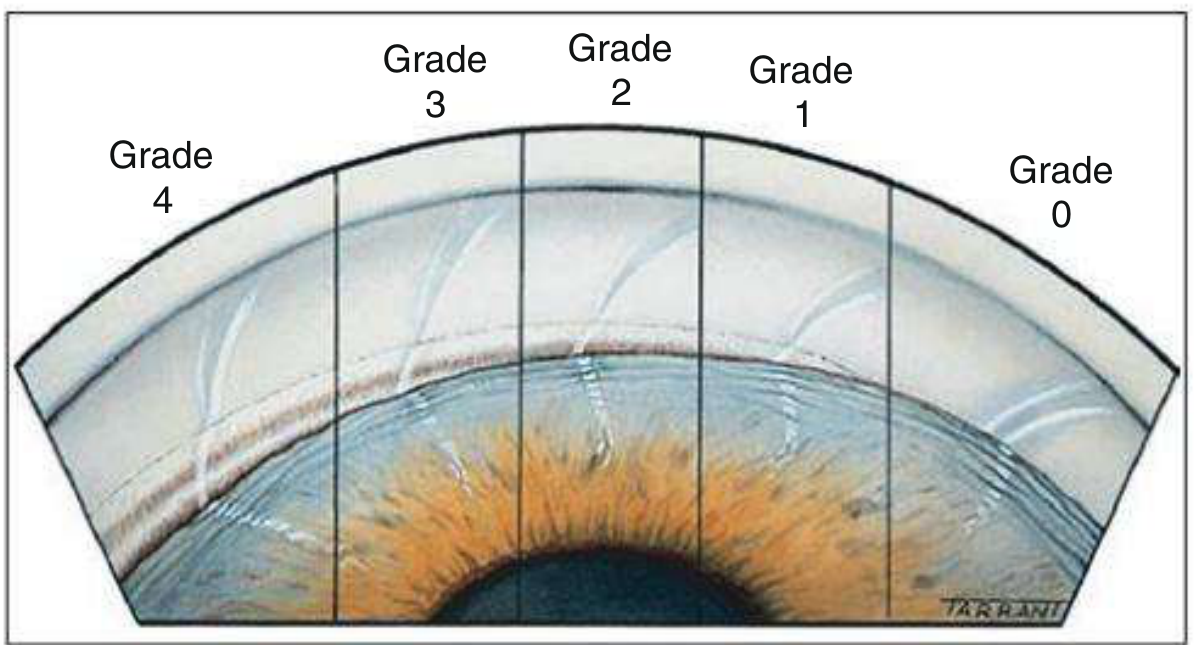
Shaffer angle grading - Kanski's Clinical Ophthalmology, Fig. 11.31
| Grade | Angle (degrees) | Visible Structures | Clinical Significance |
|---|---|---|---|
| 4 | 35-45° | Ciliary body visible | Widest; typical in myopia |
| 3 | 25-35° | Scleral spur visible | Open - incapable of closure |
| 2 | 20° | Trabeculum only, no scleral spur | Should undergo gonioscopy |
| 1 | 10° | Schwalbe line ± top of trabeculum | Very narrow - dangerously occludable |
| 0 | 0° | Iridocorneal contact | Closed |
Van Herick method (slit lamp): compares peripheral AC depth to corneal thickness - a space <1/4 corneal thickness = gonioscopy urgently needed.
Pathophysiology - Mechanism of Angle Closure
The relative pupillary block is the primary mechanism in most cases:
Anatomically predisposed eye (hypermetropic, short axial length, shallow AC)
↓
Posterior iris surface contacts anterior lens surface
↓
Aqueous CANNOT flow freely from posterior → anterior chamber
↓
Pressure builds in posterior chamber
↓
Peripheral iris bows FORWARD (iris bombé)
↓
Peripheral iris occludes trabecular meshwork
↓
Aqueous CANNOT drain → IOP rises rapidly to 50-80 mmHg
↓
Ischemia of cornea, iris, lens, optic nerve
Why pupillary mid-dilation is the danger zone:
- Miosis → iris taut → pulls away from lens → flow unblocked
- Mydriasis → iris folds peripherally → angle may open
- Mid-dilation (4-6 mm) → maximum lens-iris contact area → maximum block
Predisposing Factors (Risk Factors)
| Factor | Detail |
|---|---|
| Refractive error | Hypermetropia (short axial length, shallow AC) - most common |
| Age | Elderly - lens increases in volume with age, displacing iris anteriorly |
| Sex | Females more commonly affected |
| Race | Particularly prevalent in Far Eastern and Indian Asians |
| Family history | Genetic factors important but poorly defined |
| Axial length | Short eyes (nanophthalmos <20 mm) - very high risk |
| Cataracts | Large lens → phacomorphic element |
Precipitating Factors
An attack is triggered by anything that produces pupillary mid-dilation or forward iris displacement:
- Dim lighting (cinema, watching TV in the dark) - physiological mydriasis
- Pharmacological mydriasis - atropine drops, cyclopentolate (e.g. during fundus examination - a key MBBS exam point)
- Systemic drugs: anticholinergics (antihistamines, antispasmodics), sympathomimetics, cold/flu remedies, motion sickness patches, inhalers
- Topiramate and other sulfonamide derivatives - cause ciliary body effusion pushing the lens-iris diaphragm forward
- Semi-prone reading position
- Acute emotional stress
- Rarely: pilocarpine (miosis-induced forward iris shift in certain eyes)
Clinical Features
Symptoms
| Symptom | Mechanism |
|---|---|
| Severe unilateral eye pain | Very high IOP → stretching of ocular coats |
| Periocular/brow pain | Referred pain via trigeminal nerve |
| Headache | IOP-mediated |
| Blurred vision | Corneal epithelial edema |
| Coloured halos around lights | Corneal epithelial edema diffracting light ("rainbow around lights") |
| Nausea and vomiting | Vagal reflex; may simulate acute abdomen |
| Redness | Circumcorneal injection |
Classic exam point: Nausea and vomiting can be so severe that the patient may present to a general physician with apparent abdominal pain, and the eye problem is missed. Always check the pupil.
Signs (APAC - the full examination findings)
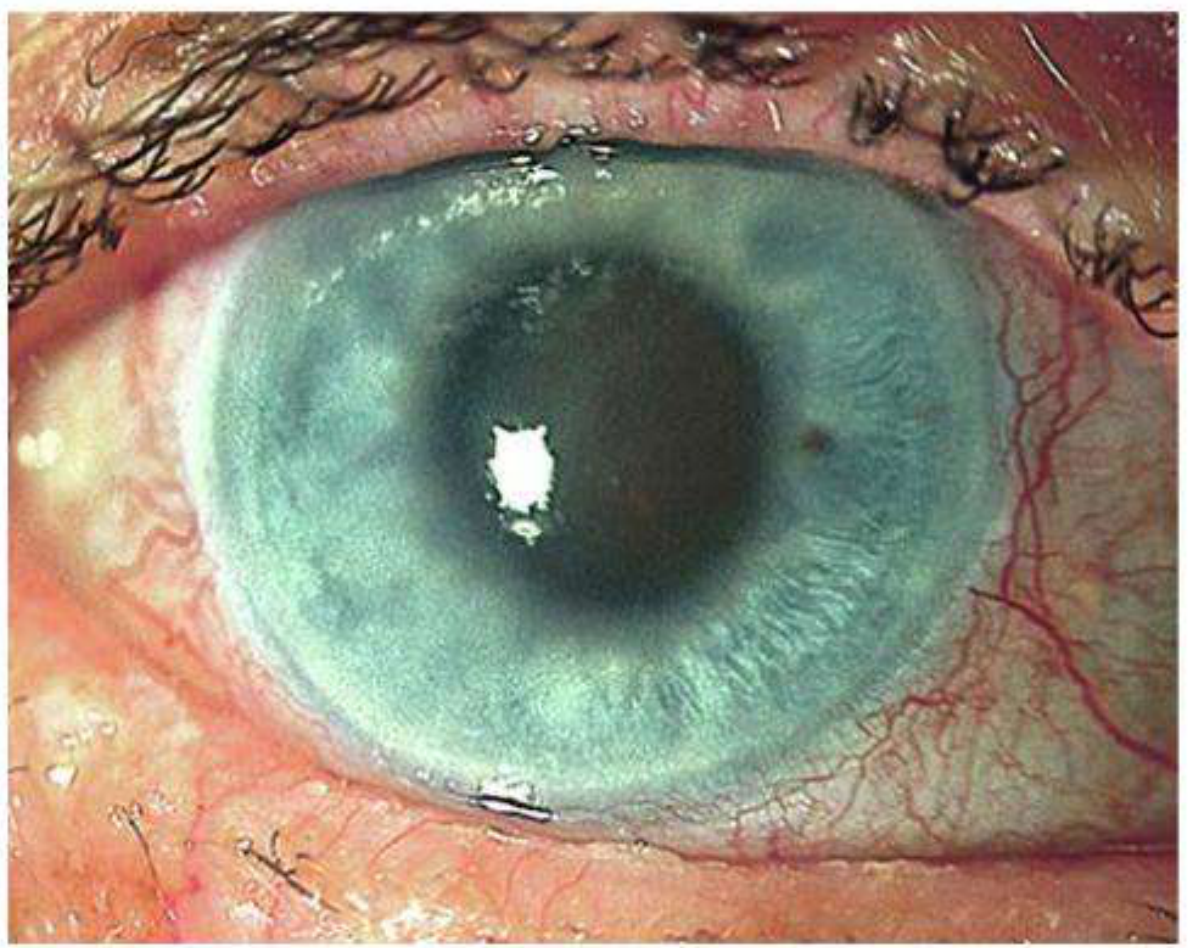
Acute congestive glaucoma - mid-dilated vertically oval, non-reactive pupil with corneal haze - Kanski's Clinical Ophthalmology, Fig. 11.36
| Sign | Detail |
|---|---|
| Visual acuity | 6/60 to hand movements (HM) |
| IOP | Very high: 50-80 mmHg (can approach diastolic BP) |
| Conjunctiva | Violaceous circumcorneal (ciliary/pericorneal) injection |
| Cornea | Hazy, cloudy due to epithelial edema |
| Anterior chamber | Shallow + aqueous flare (protein-rich exudate) |
| Pupil | Mid-dilated, vertically oval, fixed/non-reactive - CLASSIC SIGN |
| Fellow eye | Typically shows an occludable angle (same anatomical predisposition) |
| Penlight test | Shadow on nasal side of iris when light shone from temporal side = shallow AC |
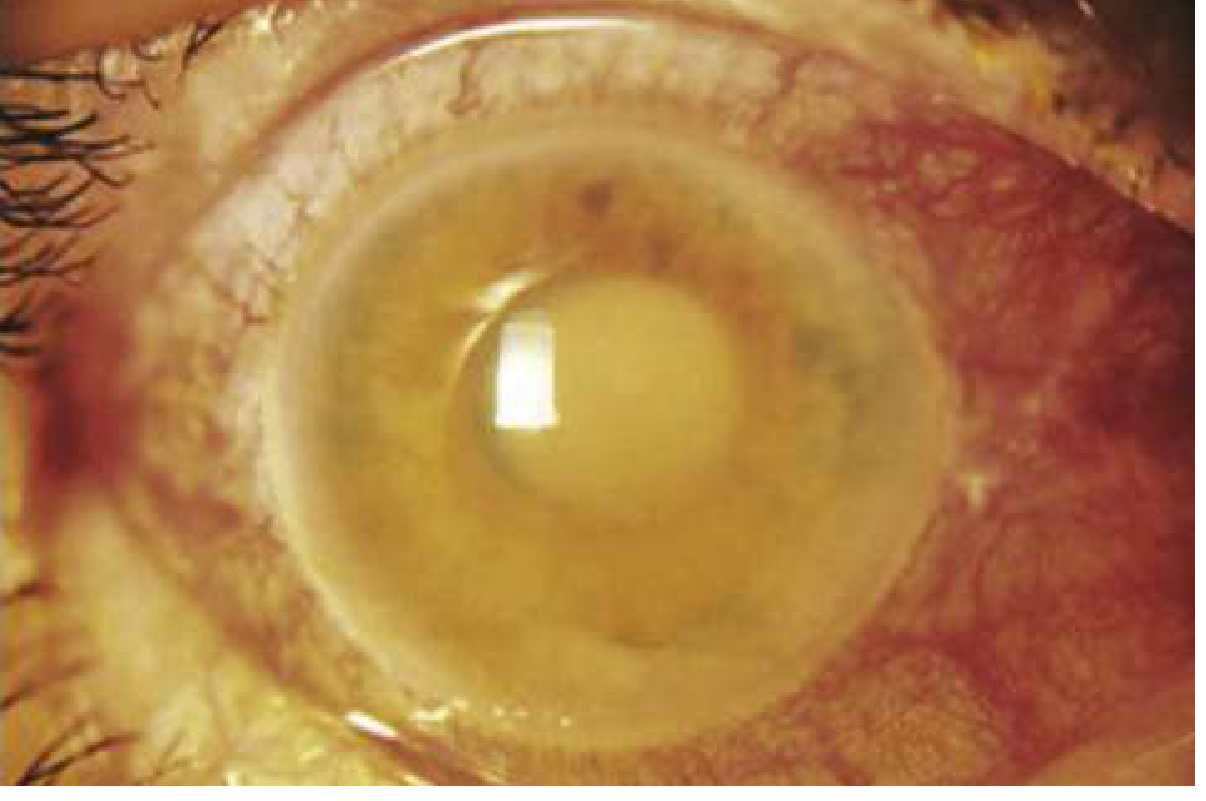
Acute angle-closure glaucoma - cloudy cornea, injected conjunctiva - Rosen's Emergency Medicine, Fig. 57.22
Sequelae After an Acute Attack (Post-Congestive Changes)
| Finding | Significance |
|---|---|
| Glaukomflecken | Small anterior subcapsular lens opacities - pathognomonic of previous acute attack; caused by ischemic necrosis of lens epithelium |
| Spiral-shaped iris atrophy | Sector iris atrophy from ischemia |
| Posterior synechiae | Adhesions between iris and lens |
| Corneal folds (Descemet membrane) | Residual corneal edema |
| Optic atrophy | Combined pallor and cupping from optic nerve ischemia |
| Peripheral anterior synechiae (PAS) | Permanent angle closure requiring surgery |
Investigations
- IOP measurement (tonometry - applanation/Tonopen): typically >30-80 mmHg
- Gonioscopy (gold standard for angle assessment): shows Grade 0-1 angle; confirms ITC; indentation gonioscopy distinguishes appositional from synechial closure
- Slit lamp examination: corneal edema, shallow AC, flare, pupil changes, glaukomflecken
- Penlight test: Oblique illumination - shallow AC casts a shadow on nasal iris
- Visual field testing: after acute phase
- Optic disc assessment: cupping, pallor
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Acute iritis/uveitis | Miosed pupil (vs. mid-dilated), keratic precipitates, IOP normal/low, photophobia |
| Acute conjunctivitis | Discharge, normal vision, normal IOP, no corneal edema |
| Corneal ulcer | Staining with fluorescein, history of trauma/contact lens |
| Migraine | No red eye, no corneal edema, normal IOP, visual aura |
| Paroxysmal hemicrania | Autonomic symptoms, normal IOP |
| Cataracts | Painless, no acute red eye, gradual onset |
| Acute abdomen | Missed if vomiting dominating - ALWAYS examine the eyes |
Management
Immediate (Emergency) Treatment - Lower IOP Fast
Step 1: Reduce aqueous production
| Drug | Dose | Route | Mechanism |
|---|---|---|---|
| Acetazolamide (carbonic anhydrase inhibitor) | 500 mg IV (if IOP >50 mmHg) OR 500 mg oral (if IOP <50 mmHg) | IV / PO | Reduces aqueous secretion by ciliary epithelium |
| Timolol 0.5% (beta-blocker) | 1-2 drops | Topical | Reduces aqueous production |
| Apraclonidine 0.5%-1% (alpha-2 agonist) | 1 drop | Topical | Reduces aqueous production, mild increased outflow |
Step 2: Increase aqueous outflow / miose the pupil
| Drug | Dose | Route | Mechanism |
|---|---|---|---|
| Pilocarpine 2% | 1 drop to affected eye; repeat after 30 min. 1% to fellow eye | Topical | Miosis → pulls peripheral iris away from angle → opens drainage |
| Prednisolone 1% | 1 drop | Topical | Reduces intraocular inflammation |
Critical exam point: Pilocarpine should NOT be repeated if IOP remains >40 mmHg - ischemia of the iris sphincter impairs its action, it may exert a forward iris vector and excessive dosing carries systemic toxicity risk.
Step 3: Systemic osmotic agents (resistant cases)
| Drug | Dose | Route |
|---|---|---|
| Mannitol 20% | 1-2 g/kg IV over 1 hour | IV |
| Glycerol 50% | 1 g/kg | Oral |
| Isosorbide | 1-1.5 g/kg | Oral |
Also:
- Analgesia and antiemetic
- Patient lying supine helps aqueous lens-iris separation
Drug Summary Box (from Rosen's Emergency Medicine):
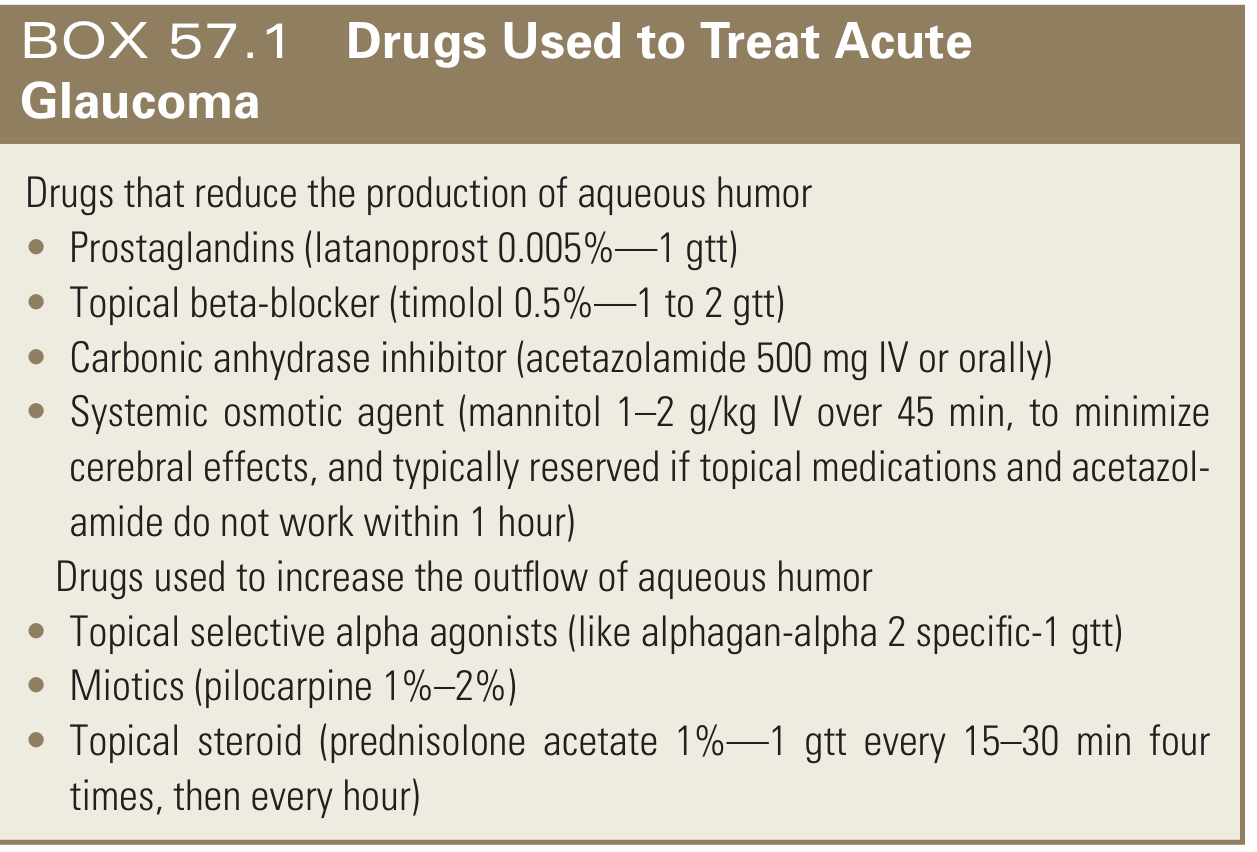
Drugs for acute glaucoma - Rosen's Emergency Medicine, Box 57.1
Definitive Treatment - Breaking the Anatomical Block
Laser Peripheral Iridotomy (LPI) - Treatment of Choice
- Creates a small full-thickness hole in the peripheral iris
- Equalizes pressure between posterior and anterior chambers
- Breaks the pupillary block mechanism
- Performed within 24-48 hours once the cornea has cleared (glycerol 50% drops can be used to clear corneal edema first)
- Bilateral - prophylactic LPI should be performed on the fellow eye as it has the same anatomical predisposition
Surgical Options (if laser fails or not available):
- Peripheral iridectomy (surgical - the historic gold standard before laser)
- Lens extraction (phacoemulsification + IOL) - deepens the AC, corrects hypermetropia, opens the angle; highly effective - EAGLE trial shows this may be preferred over LPI in eyes with early PACG
- Goniosynechialysis - to break peripheral anterior synechiae
- Trabeculectomy - if IOP remains elevated despite open angle
- Cyclodiode laser - cyclodestruction in refractory cases
- Paracentesis - effective emergency option but risk of lens damage; reserved for extreme cases
Subsequent / Follow-up Treatment
After IOP is controlled and cornea clears:
- Pilocarpine 2% four times daily to affected eye
- Pilocarpine 1% four times daily to fellow eye
- Topical steroids (prednisolone 1%) four times daily if acutely inflamed
- Continue timolol/apraclonidine as needed by IOP response
- Gonioscopy repeated to confirm angle is open
- Bilateral LPI performed electively once attack resolved
Contraindications to Remember
- Acetazolamide - contraindicated in sulfonamide allergy AND angle closure secondary to topiramate (sulfonamide derivative - giving acetazolamide worsens ciliary body effusion)
- Mannitol - contraindicated in cardiac failure, renal failure, pulmonary edema
- Pilocarpine not to be repeated when IOP >40 mmHg
MBBS Exam High-Yield Summary
| Feature | Key Fact |
|---|---|
| Most common cause | Hypermetropic middle-aged/elderly female |
| Mechanism | Relative pupillary block → iris bombé → angle closure |
| Classic precipitant | Pharmacological mydriasis (atropine, cyclopentolate, dark cinema) |
| IOP in attack | 50-80 mmHg |
| Pathognomonic sign | Mid-dilated vertically oval fixed pupil |
| Pathognomonic sequela | Glaukomflecken (anterior subcapsular lens opacities) |
| Gold standard investigation | Gonioscopy |
| First drug given | Acetazolamide 500 mg IV/oral |
| Miotic used | Pilocarpine 2% |
| Definitive treatment | Laser peripheral iridotomy |
| Fellow eye treatment | Prophylactic LPI (same anatomy, high risk) |
| Must not miss trap | Nausea/vomiting masking as acute abdomen - examine the eye |
| Race with highest prevalence | Far Eastern and Indian Asians |
Sources: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th Ed. | Rosen's Emergency Medicine, 10th Ed. | Goldman-Cecil Medicine, International Ed.
Create a quick-reference PDF flowchart for acute angle-closure management for the ED
Reading File
Running Command
mkdir -p /home/daytona/workspace/aacg-flowchart && ls /home/daytona/workspace/
!
Failed to create session: bad request: failed to resolve container IP after 3 attempts: no IP address found. Is the Sandbox started?
We encountered an error while processing your request. Please try again or reach out to us for help.
This is a shared conversation. Sign in to Orris to start your own chat.