Explain me ecg changes of major heart diseases in emergency
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive data from Tintinalli's Emergency Medicine, Harrison's, Goldman-Cecil, and Rosen's Emergency Medicine. Let me compile the full answer:
ECG Changes in Major Cardiac Emergencies
Sources: Tintinalli's Emergency Medicine, Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine, Rosen's Emergency Medicine, Braunwald's Heart Disease
Pathophysiology of ST Changes (The Foundation)
Ischemia exerts complex time-dependent effects on myocardial cells. Severe acute ischemia lowers the resting membrane potential, creating a voltage gradient between normal and ischemic zones — "currents of injury" — visible as ST deviation. The direction of the ST vector determines whether you see elevation or depression:

A = Subendocardial ischemia → ST depression in overlying leads. B = Transmural (epicardial) ischemia → ST elevation in overlying leads.
1. STEMI — ST-Elevation Myocardial Infarction
Diagnostic Criteria (per Tintinalli's)
New ST elevation at the J-point:
- ≥1 mm in all leads except V₂–V₃
- ≥2 mm in V₂–V₃ (men ≥40 y), ≥2.5 mm (men <40 y), ≥1.5 mm (women)
Localisation by Territory
| Territory | Leads with ST Elevation | Infarct-Related Artery |
|---|---|---|
| Anteroseptal | V₁, V₂ (±V₃) | Proximal LAD |
| Anterior | V₁–V₄ | LAD |
| Anterolateral | V₁–V₆, I, aVL | Proximal LAD / LCx |
| Lateral | I, aVL | LCx or diagonal |
| Inferior | II, III, aVF | RCA (most common) or LCx |
| Inferolateral | II, III, aVF + V₅, V₆ | RCA or dominant LCx |
| True posterior | Tall R in V₁–V₂, R/S ≥1, ST depression V₁–V₃ | LCx / RCA |
| Right ventricular (RV) | II, III, aVF + ST elevation in V₃R–V₆R | Proximal RCA |
Inferior STEMI ECG (RCA occlusion):
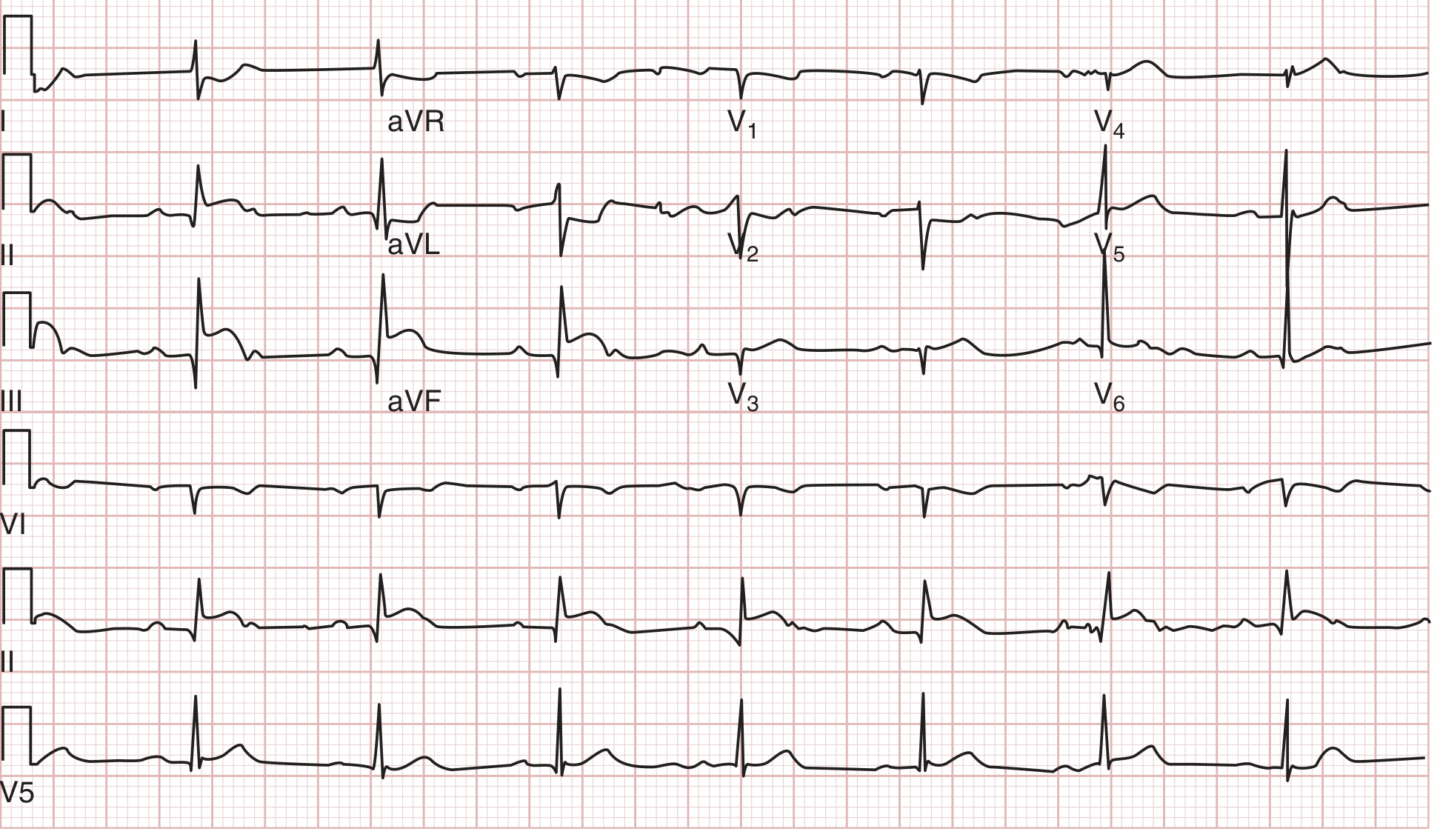
ST elevation in III > II, ST depression in I and aVL — 100% RCA occlusion confirmed at catheterisation.
Anterior STEMI ECG (LAD occlusion):
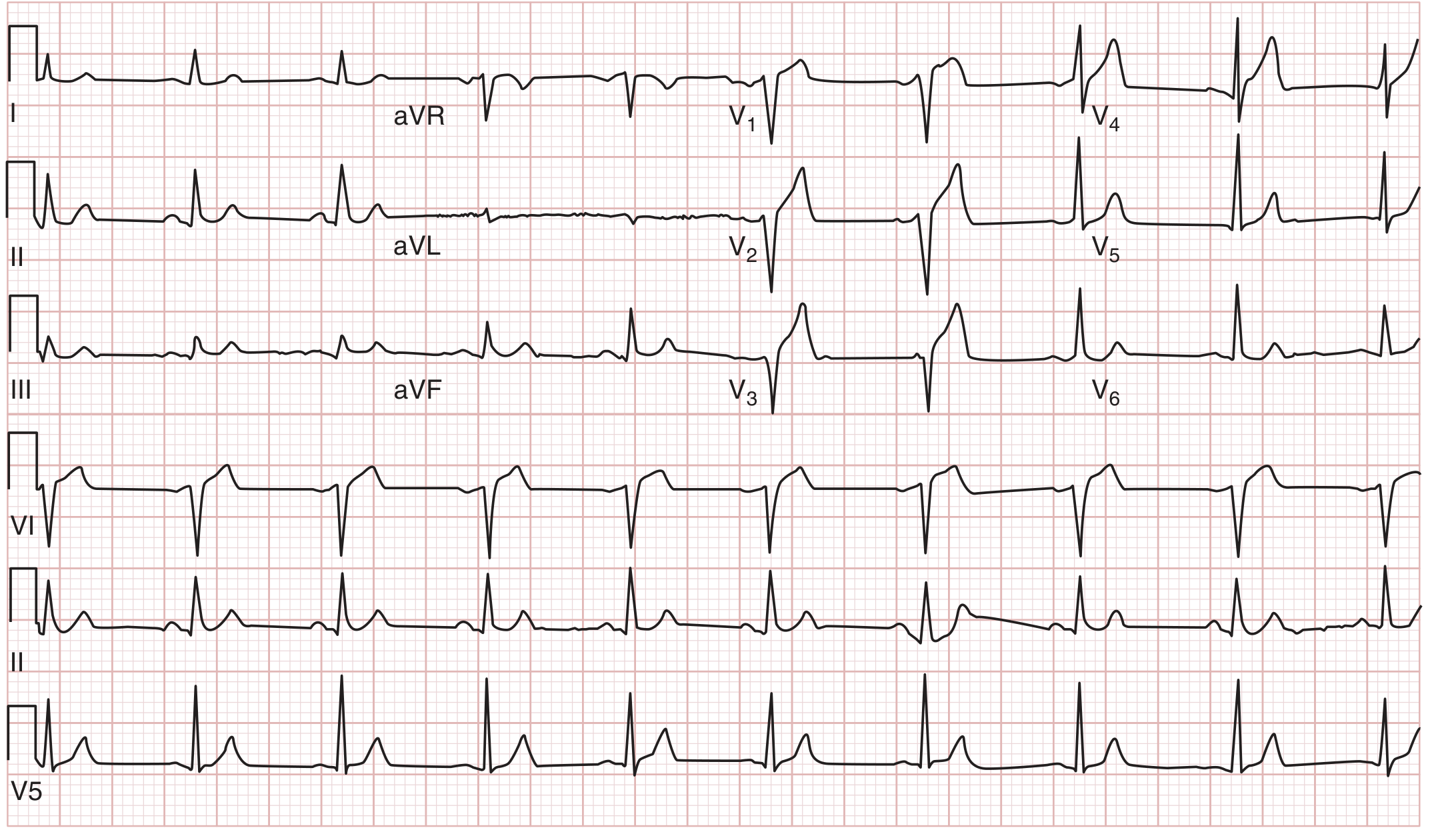
ST elevation in I, V₁–V₃ with absence of depression in II/III/aVF — distal LAD.
Evolutionary ECG Sequence
| Time | ECG Finding |
|---|---|
| Minutes (hyperacute) | Tall, broad, peaked hyperacute T waves |
| Hours | ST elevation — convex ("tombstone") or concave |
| Hours–days | T-wave inversion begins in same leads |
| Hours–days | Pathological Q waves develop (>40 ms wide, >25% of R height) |
| Days–weeks | ST normalises; T waves may remain inverted |
| Months–years | Q waves persist (marker of old infarct) |
Key Points
- Reciprocal ST depression in leads opposite the infarct zone indicates larger injury, more severe CAD, worse prognosis
- New LBBB with chest pain was historically a STEMI equivalent, but <10% actually have AMI — use Sgarbossa criteria
- RV infarction: always obtain right-sided leads (V₄R) in inferior STEMI; ST elevation ≥1 mm in V₄R is highly suggestive
2. NSTEMI / Unstable Angina
ECG Findings
- ST depression ≥0.5 mm in ≥2 contiguous leads (subendocardial ischemia pattern)
- T-wave inversions — symmetric, deep
- ST elevation in aVR with diffuse ST depression elsewhere → suggests left main or proximal LAD occlusion (or severe 3-vessel disease)
- Normal ECG in 1–6% of confirmed NSTEMI — does not exclude the diagnosis
Wellens' Syndrome (Critical LAD Stenosis)
A warning pattern indicating critical proximal LAD stenosis — often pain-free at time of ECG:
- Type A (25%): Biphasic T waves in V₂–V₃
- Type B (75%): Deeply symmetric T-wave inversions in V₂–V₃ (may extend to V₄–V₆)
- T-wave changes normalise when pain returns, reappear when pain subsides — dynamic pattern
3. Acute Pericarditis
Stages of ECG Change
| Stage | Timing | ECG |
|---|---|---|
| Stage I | Acute (days) | Diffuse concave ("saddle-shaped") ST elevation in nearly all leads (I, II, III, aVF, V₂–V₆); PR depression (most specific); ST elevation in aVR with PR elevation |
| Stage II | 1–2 weeks | ST and PR normalise |
| Stage III | Weeks | Diffuse T-wave inversions |
| Stage IV | Months | ECG returns to normal |
Distinguishing from STEMI
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST distribution | Diffuse (all leads) | Regional (territory) |
| ST shape | Concave (saddle) | Convex (tombstone) |
| Reciprocal changes | Absent (except aVR) | Present |
| PR depression | Yes | No |
| Q waves | No | Yes (evolving) |
| ST:T ratio in V₆ | >0.25 → pericarditis | <0.25 |
4. Cardiac Tamponade
ECG Findings
- Sinus tachycardia — almost universal
- Low voltage (QRS amplitude <5 mm in limb leads, <10 mm precordial) — from pericardial fluid insulating electrical activity
- Electrical alternans — beat-to-beat alternation in QRS amplitude/morphology as the heart swings within fluid; pathognomonic when present
"The cardiac position will alternate, with the heart returning to its original position with every other beat, thus electrical alternans may be seen." — Rosen's Emergency Medicine
- Electrical alternans is highly specific but seen in only ~20% of tamponade; its absence does not exclude tamponade
5. Pulmonary Embolism (PE)
The ECG in PE is often non-specific or normal in minor PE. In massive PE with right heart strain:
Classic Pattern — S₁Q₃T₃
- S wave in lead I (right axis deviation)
- Q wave in lead III
- T-wave inversion in lead III
Other RV Strain Patterns
- Sinus tachycardia — most common finding
- New RBBB (complete or incomplete) — indicates severe RV strain/hypertension
- T-wave inversions in V₁–V₄ — RV strain
- Right axis deviation
- P pulmonale (peaked P in II >2.5 mm) — right atrial enlargement
- Atrial fibrillation/flutter
- ST elevation in V₁ ± aVR
"A new right bundle branch block suggests right ventricular strain and severe pulmonary hypertension." — Goldman-Cecil Medicine
The S₁Q₃T₃ is specific but present in only ~20% of PE cases; sinus tachycardia + anterior T-wave inversions is more commonly seen with large PE.
6. Hyperkalemia
ECG changes progress in a predictable sequence with rising K⁺:
| K⁺ Level | ECG Change |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked (tent-shaped) T waves, narrow base, shortened QT |
| 6.5–7.5 mEq/L | Loss of P waves, PR prolongation, widening QRS |
| 7.0–8.0 mEq/L | Wide QRS, ST changes (depression), bundle branch blocks |
| >8.0–9.0 mEq/L | Sine wave pattern (QRS merges with T wave) → imminent cardiac arrest, VF |
The sine wave is a medical emergency requiring immediate IV calcium.
7. Wolff-Parkinson-White (WPW)
ECG Triad During Sinus Rhythm
- Short PR interval (<120 ms) — rapid conduction via accessory pathway bypasses AV node delay
- Delta wave — slurred upstroke of initial QRS (pre-excitation of ventricle)
- Widened QRS complex — fusion of normal and accessory pathway depolarisation
- Secondary ST-T changes — discordant to QRS direction
Tachyarrhythmias in WPW (Emergency)
| Type | ECG | Rate | Danger |
|---|---|---|---|
| Orthodromic AVRT (65%) | Narrow QRS, regular, no delta wave | 160–220 bpm | Moderate |
| Antidromic AVRT (5–10%) | Wide QRS, regular, can mimic VT | 160–220 bpm | High |
| AF with pre-excitation (25%) | Wide, bizarre, irregular QRS, delta waves, rate often >200 bpm | >200 bpm | Immediately life-threatening |
Critical Warning: In WPW + AF, avoid AV-nodal blocking agents (adenosine, verapamil, digoxin, beta-blockers) — they block the normal pathway, forcing all conduction down the accessory pathway, potentially triggering VF.
8. Ventricular Tachycardia (VT) vs. SVT with Aberrancy
VT Features on ECG (Favour VT)
- AV dissociation (P waves independent of QRS) — most specific sign
- QRS width >160 ms
- Concordance in precordial leads (all positive or all negative)
- Fusion beats and capture beats
- Extreme axis (Northwest axis, −90° to ±180°)
- Brugada criteria / Josephson's sign (notching near S-wave nadir)
SVT with Aberrancy
- QRS usually <160 ms
- Typical RBBB or LBBB morphology
- Responds to vagal manoeuvres or adenosine
9. Aortic Dissection
ECG is usually non-specific, but important to obtain urgently to exclude MI (since thrombolytics given for MI are fatal in dissection):
- Most common: normal ECG or non-specific ST-T changes
- ST elevation in inferior leads — if dissection involves the RCA ostium (Type A with coronary involvement)
- LVH pattern — from underlying hypertension (common predisposing factor)
- Pericardial effusion changes (low voltage, electrical alternans) — from haemopericardium in Type A
10. Brugada Syndrome
A channelopathy causing sudden cardiac death in structurally normal hearts:
- Type 1 (diagnostic): Coved ST elevation ≥2 mm in V₁–V₂ with T-wave inversion — "coved pattern"
- Type 2: Saddle-back ST elevation ≥2 mm in V₁–V₂ (high takeoff) — not diagnostic alone
- Pattern can be concealed and unmasked by fever, sodium channel blockers, class IC antiarrhythmics
11. Long QT Syndrome / Torsades de Pointes
- QTc >440 ms (men), >460 ms (women) — prolonged
- QTc >500 ms — high risk for Torsades de Pointes (TdP)
- Torsades: Polymorphic VT with rotating axis ("twisting of the points") around baseline — characteristically self-terminates but can degenerate to VF
- Triggers: hypomagnesaemia, hypokalaemia, QT-prolonging drugs (class IA/III antiarrhythmics, antipsychotics, antiemetics)
- Treatment: IV magnesium 2g, correct electrolytes, consider overdrive pacing
Quick Reference Summary Table
| Emergency | Key ECG Finding | Do Not Miss |
|---|---|---|
| Anterior STEMI | ST elevation V₁–V₄ | Check for aVR elevation (LM/proximal LAD) |
| Inferior STEMI | ST elevation II, III, aVF | Get right-sided leads → RV infarction |
| Posterior MI | Tall R + ST depression V₁–V₃ | Mirror image: posterior leads show elevation |
| NSTEMI/UA | ST depression, T inversion | Normal ECG does not exclude |
| Wellens' syndrome | Biphasic/deep T in V₂–V₃ (pain free) | Do NOT stress test — proximal LAD critical stenosis |
| Pericarditis | Diffuse concave ST elevation + PR depression | Differentiate from STEMI |
| Tamponade | Low voltage + electrical alternans | Treat clinically + echo, not ECG alone |
| PE (massive) | Sinus tachy, S₁Q₃T₃, new RBBB, T inversion V₁–V₄ | Normal ECG does not exclude PE |
| Hyperkalemia | Peaked T → loss of P → wide QRS → sine wave | Sine wave = give IV calcium STAT |
| WPW + AF | Wide irregular QRS >200 bpm | NO AV blockers — can cause VF |
| VT | Wide QRS + AV dissociation | Treat as VT until proven otherwise |
| Brugada | Coved ST in V₁–V₂ | Fever can unmask; high SCD risk |
| Long QT / TdP | QTc >500 ms, polymorphic VT | IV Mg 2g + correct K⁺/Mg²⁺ |
Sources: Tintinalli's Emergency Medicine (9e), Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine, Rosen's Emergency Medicine, Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.