I have my MD medicine exams coming up.
Asking for Preferences
No problem! I'm ready to help you ace your MD medicine exams. Here's what I can do for you:
Ask me anything across all medicine topics:
- Cardiology - heart failure, arrhythmias, ACS, valvular disease
- Respiratory - COPD, asthma, pneumonia, TB, lung cancer
- Nephrology - AKI, CKD, glomerulonephritis, electrolyte disorders
- Gastroenterology - liver disease, IBD, GI bleeding, pancreatitis
- Endocrinology - diabetes, thyroid, adrenal, pituitary disorders
- Neurology - stroke, epilepsy, meningitis, movement disorders
- Infectious Disease - antibiotics, tropical medicine, sepsis
- Hematology/Oncology - anemias, leukemias, coagulation disorders
- Rheumatology - SLE, RA, vasculitis, crystal arthropathies
- Pharmacology - drug mechanisms, side effects, interactions
How I can help:
- Explain concepts and pathophysiology clearly
- High-yield MCQ-style questions with explanations
- Mnemonics and memory aids
- Differentials and clinical reasoning
- Quick revision summaries
- Recent evidence and guidelines
I have access to authoritative medical textbooks and current literature. Just ask me your first question or name the topic you want to start with!
Teach me ecg from basics to advanced for exam as well as daily clinical practice.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is your complete ECG masterclass, built from Harrison's Principles of Internal Medicine (22nd ed., 2025) and Fuster & Hurst's The Heart (15th ed.).
ECG Mastery: Basics to Advanced
MODULE 1 - Why ECG? The Big Picture
The ECG records electrical activity of the heart from the body surface using 12 leads. It is the single most used diagnostic test in medicine - cheap, instant, non-invasive, and packed with information. Every clinical doctor must be able to read one confidently.
What the ECG tells you:
- Rhythm and rate
- Conduction system integrity
- Chamber size (hypertrophy)
- Ischemia and infarction (location, age, extent)
- Metabolic/electrolyte status
- Drug effects
- Pericardial disease
MODULE 2 - The Cardiac Conduction System
Before reading any ECG you must understand what generates the signals.
SA Node (right atrium)
↓ (atrial depolarization = P wave)
AV Node (PR delay = AV node slowing)
↓
Bundle of His
↓
Right Bundle Branch + Left Bundle Branch
↙ ↘
Left Anterior Left Posterior
Fascicle Fascicle
↓
Purkinje Fibers → Ventricular myocardium (= QRS)
Key points:
- SA node fires at 60-100/min (dominant pacemaker)
- AV node fires at 40-60/min if SA fails (junctional escape)
- Purkinje / ventricle fires at 20-40/min (ventricular escape)
- Ventricular repolarization = ST segment + T wave
MODULE 3 - ECG Paper and Calibration
Always check calibration before reading any ECG.
| Parameter | Value |
|---|---|
| Paper speed | 25 mm/s (standard) |
| 1 small square (1 mm) | 0.04 s (40 ms) |
| 1 large square (5 mm) | 0.20 s (200 ms) |
| Standard voltage | 1 mV = 10 mm (2 large squares tall) |
| Half-standard | 1 mV = 5 mm (written on trace) |
MODULE 4 - ECG Waveforms and Intervals

(Harrison's Principles of Internal Medicine 22E, Fig. 247-2)
The Waves
| Wave | Represents | Normal |
|---|---|---|
| P wave | Atrial depolarization | <120 ms wide, <2.5 mm tall; upright in II, inverted in aVR |
| QRS complex | Ventricular depolarization | <100-110 ms (2.5 small squares) |
| Q wave | Septal depolarization (normal) or infarction (pathological) | Normal: <0.04 s, <25% of R height |
| ST segment | Plateau of action potential (phase 2) | Isoelectric (flat) |
| T wave | Ventricular repolarization | Upright in I, II, V3-V6; inverted in aVR normal |
| U wave | After-depolarization / Purkinje repolarization | Same direction as T, low amplitude |
The Intervals
| Interval | Normal Range | Meaning |
|---|---|---|
| PR | 120-200 ms (3-5 small squares) | AV conduction time |
| QRS | <100-110 ms | Ventricular conduction |
| QT | <450 ms men, <460 ms women (rate-corrected) | Total ventricular repolarization |
| RR | Depends on rate | Used to calculate heart rate |
Heart Rate Calculation:
- Regular rhythm: HR = 300 ÷ (number of large squares between R-R)
- Or: HR = 1500 ÷ (number of small squares between R-R)
- Irregular: count QRS complexes in 10-second strip × 6
Memorize the 300 rule:
1 large square = 300 bpm | 2 = 150 | 3 = 100 | 4 = 75 | 5 = 60 | 6 = 50
MODULE 5 - The 12 Leads (Understanding the "Camera Angles")
Each lead is like a camera viewing the heart from a different direction. A positive (upright) deflection means electrical activity is moving toward that lead's positive pole.
Limb Leads (Frontal Plane)
| Lead | Looks at | Positive Pole Direction |
|---|---|---|
| I | Lateral | 0° (left) |
| II | Inferior | +60° |
| III | Inferior | +120° |
| aVR | Cavity (right shoulder) | -150° |
| aVL | Lateral (left shoulder) | -30° |
| aVF | Inferior (feet) | +90° |
Memory trick for limb lead placement: RA, LA, RL, LL (Red Arm, Yellow Arm, Green Leg, Black Leg - "Ride Your Green Bike")
Precordial Leads (Horizontal Plane)
| Lead | Position | Looks at |
|---|---|---|
| V1 | 4th ICS, right sternal border | Septal / RV |
| V2 | 4th ICS, left sternal border | Septal |
| V3 | Between V2 and V4 | Anterior |
| V4 | 5th ICS, midclavicular line | Anterior |
| V5 | Anterior axillary line | Lateral |
| V6 | Midaxillary line | Lateral |
Grouping Leads by Territory
| Territory | Leads | Coronary Artery |
|---|---|---|
| Inferior | II, III, aVF | RCA (right coronary) |
| Anteroseptal | V1, V2, V3, V4 | LAD (left anterior descending) |
| Lateral | I, aVL, V5, V6 | LCx (left circumflex) |
| Posterior | Reciprocal changes in V1, V2 | RCA / LCx |
| Right ventricle | V3R, V4R (right leads) | RCA proximal |
MODULE 6 - The Normal ECG (What to Expect)
Normal Sinus Rhythm Checklist
- Rate: 60-100 bpm
- P wave before every QRS; QRS after every P
- PR interval: 120-200 ms
- P wave: upright in I, II; inverted in aVR
- QRS: <110 ms, normal axis (-30° to +90°)
- R-wave progression in V1-V6 (R grows from V1 to V5)
P Wave Morphology
- Right atrial enlargement (P pulmonale): P wave >2.5 mm tall in II (peaked)
- Left atrial enlargement (P mitrale): P wave >120 ms wide, notched in II; terminal negative deflection in V1 >1 mm² (>1 small square wide AND deep)
QRS Axis
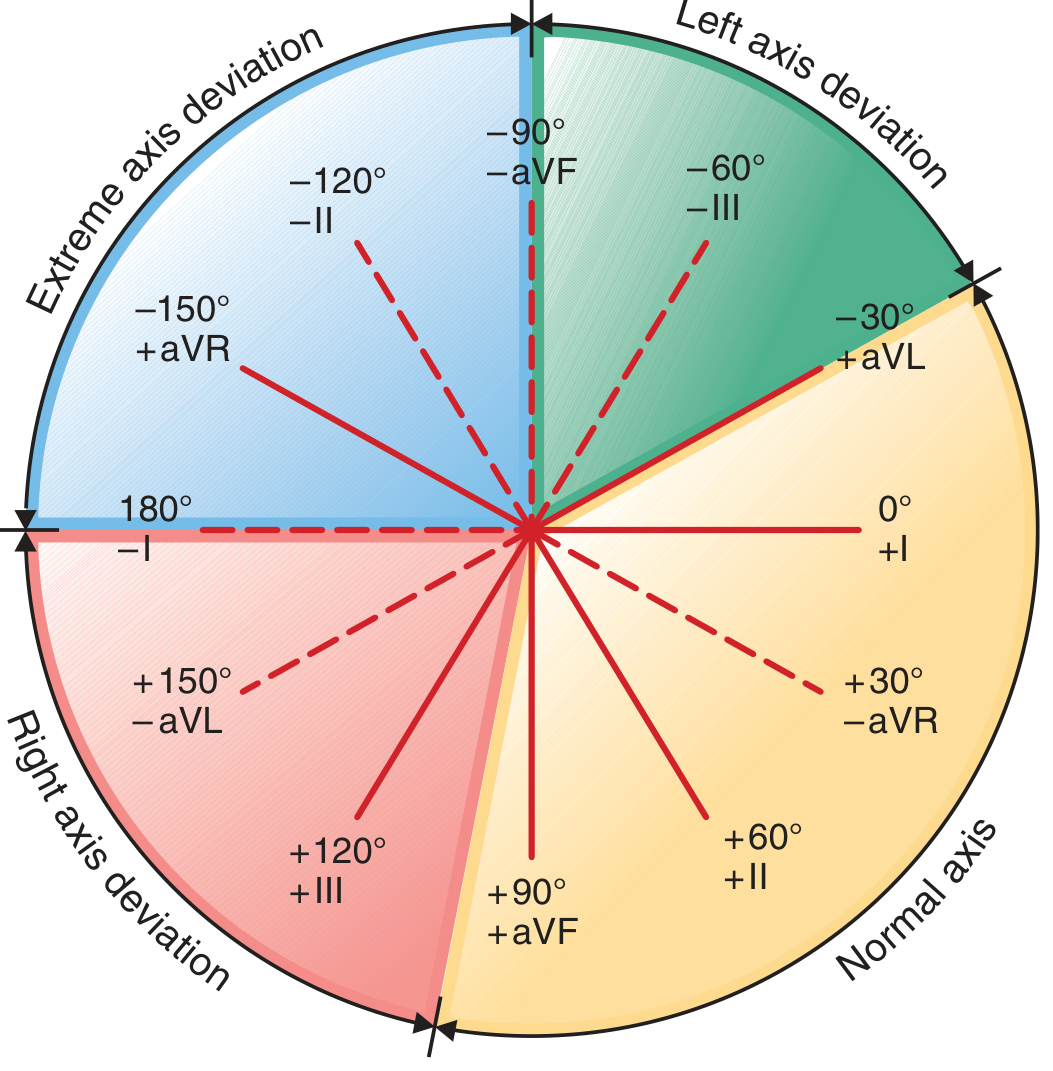
(Harrison's Principles of Internal Medicine 22E, Fig. 247-4)
| Axis | Degrees | Leads |
|---|---|---|
| Normal | -30° to +90° | QRS upright in I and aVF |
| Left axis deviation (LAD) | -30° to -90° | QRS upright in I, negative in aVF |
| Right axis deviation (RAD) | +90° to +180° | QRS negative in I, positive in aVF |
| Extreme ("Northwest") axis | -90° to +/-180° | QRS negative in both I and aVF |
Quick axis trick: Look at I and aVF.
- Both upright → Normal
- I up, aVF down → Left axis
- I down, aVF up → Right axis
- Both down → Extreme axis
Causes of LAD: LBBB, left anterior fascicular block, inferior MI, LVH, WPW (right-sided accessory pathway)
Causes of RAD: RVH, RBBB, left posterior fascicular block, PE, lateral MI, WPW (left-sided accessory pathway), normal variant in tall thin adults
MODULE 7 - Chamber Enlargement / Hypertrophy
Left Ventricular Hypertrophy (LVH)
Most used criteria (Sokolow-Lyon):
- S in V1 + R in V5 or V6 ≥ 35 mm
- R in aVL ≥ 11 mm (Cornell criteria)
- Associated with: LV strain pattern (ST depression + T wave inversion in lateral leads I, aVL, V5, V6)
Causes: Hypertension (most common), aortic stenosis, HCM, coarctation
Right Ventricular Hypertrophy (RVH)
- R ≥ S in V1 (dominant R in V1)
- RAD (axis >+90°)
- rSR' in V1 is NOT RVH - that is RBBB
- ST depression + T wave inversion in V1-V3 (RV strain)
Causes: Pulmonary hypertension, mitral stenosis, cor pulmonale, Tetralogy of Fallot
MODULE 8 - Bundle Branch Blocks
Right Bundle Branch Block (RBBB)
Criteria:
- QRS ≥ 120 ms
- RSR' ("M-shaped" or "rabbit ears") in V1
- Wide, slurred S wave in I, V5, V6
- T wave inverted in V1 (secondary change - normal with RBBB)
Memory: "William Marrow" - RBBB: W in V1 (rSR'), M in V6... wait, it's actually simpler:
RBBB = bunny ears in V1 (rSR' = ears of a rabbit)
Causes: Normal variant, RV pressure overload, PE, anterior MI, post-cardiac surgery
Left Bundle Branch Block (LBBB)
Criteria:
- QRS ≥ 120 ms
- Broad, notched R (no Q, no S) in I, aVL, V5, V6
- rS or QS (deep S) in V1, V2
- T wave opposite to main QRS deflection (secondary change)
CRITICAL clinical point: New LBBB with chest pain = treat as STEMI equivalent (Sgarbossa criteria needed)
Memory: "WiLLiaM MaRRow"
- LBBB: W in V1, M in V6
- RBBB: M in V1, W in V6
Causes: IHD, HTN, cardiomyopathy, aortic valve disease
Fascicular Blocks (Hemiblocks)
| Block | Axis | QRS duration | Pattern |
|---|---|---|---|
| Left Anterior Fascicular Block (LAFB) | LAD > -45° | Normal or slightly prolonged | Small Q in I, aVL; small R in II, III, aVF |
| Left Posterior Fascicular Block (LPFB) | RAD > +120° | Normal | Small R in I, aVL; small Q in II, III, aVF; must exclude other RAD causes |
Bifascicular block: RBBB + LAFB (most common) = wide QRS with RBBB pattern + LAD
Trifascicular block: Bifascicular + prolonged PR = one step away from complete heart block
MODULE 9 - AV Blocks
First Degree AV Block
- PR interval > 200 ms (>1 large square)
- Every P conducts to QRS (just slowly)
- Usually benign; can be normal in athletes
Second Degree AV Block
Mobitz Type I (Wenckebach):
- Progressive PR lengthening until a P wave is blocked (QRS dropped)
- "Longer, longer, longer, DROP - then you have a Wenckebach"
- PR after the dropped beat is shortest
- Usually at AV node level; generally benign
- Can be normal in athletes (vagal tone)
Mobitz Type II:
- Fixed PR interval; sudden non-conducted P wave (QRS drops without warning)
- Below AV node (His-Purkinje level) - more serious
- Often associated with wide QRS
- High risk of progressing to complete heart block → needs pacemaker
Third Degree (Complete) AV Block
- Complete dissociation: P waves and QRS complexes march independently
- P rate > QRS rate
- QRS escape rhythm: narrow (junctional, 40-60/min) or wide (ventricular, 20-40/min)
- Wide-complex escape = more severe (infranodal block)
- Emergency: Atropine (for narrow-complex), transcutaneous pacing, then permanent pacemaker
Memory for 2nd degree blocks:
Wenckebach = Increasing PR before drop (I = Increasing) Mobitz II = Suddenly drops (II = abrupt, Sudden)
MODULE 10 - Ischemia and Infarction
This is the most clinically critical section.
Spectrum of Ischemic ECG Changes
Hyperacute T waves (earliest change, minutes):
- Tall, broad, peaked T waves over ischemic zone
- First sign of complete coronary occlusion
ST Elevation (STEMI - transmural ischemia):
- ST elevation in ≥2 contiguous leads
- Threshold: ≥1 mm (most leads), ≥2 mm (V1-V3 men), ≥1.5 mm (V1-V3 women)
- Represents full-thickness (transmural) injury
- Mechanism: epicardial injury current shifts ST vector outward
ST Depression (subendocardial ischemia/NSTEMI):
- Horizontal or downsloping ST depression ≥0.5-1 mm
- Mechanism: ischemia confined to subendocardium; ST vector shifts inward
T wave inversion (ischemia or evolving MI):
- Symmetric, deep T wave inversions
- Wellens' syndrome: deep T inversions in V2-V3 = critical proximal LAD stenosis (do NOT stress test - risk of VF)
Pathological Q waves (established infarction, hours-days):
- Width ≥ 40 ms (1 small square)
- Depth ≥ 25% of R wave height in same lead
- Represent electrically dead (necrotic) myocardium
- Q waves in II, III, aVF = inferior MI; V1-V4 = anterior MI; I, aVL = lateral MI
Localization of STEMI
| Location | ST Elevation In | Reciprocal ST Depression In | Culprit Artery |
|---|---|---|---|
| Inferior | II, III, aVF | I, aVL | RCA (80%), LCx (20%) |
| Anterior | V1-V4 | II, III, aVF (sometimes) | LAD |
| Anteroseptal | V1-V3 | - | LAD proximal |
| Apical/Extensive | V1-V6 | - | LAD proximal (widow maker) |
| Lateral | I, aVL, V5-V6 | V1-V2 | LCx |
| Posterior | Tall R + ST depression V1-V2 | ST elevation in V7-V9 | RCA or LCx |
| Right Ventricular | V1 + V4R elevation | - | Proximal RCA |
Posterior MI pearl: Tall broad R in V1 + ST depression in V1-V2 - the mirror image of anterior ST elevation. Always do V7-V9 leads if inferior MI to check for posterior extension.
RV MI pearl: Inferior STEMI + RV MI = hypotension + clear lungs - DO NOT give nitrates (will drop BP catastrophically). Give IV fluids instead.
Evolution of STEMI Over Time
Minutes: Hyperacute T waves (peaked, tall)
Hours: ST elevation (convex/"tombstone" shape)
6-24h: ST elevation + Q waves appear + T inversion begins
Days: ST returns to baseline + T waves inverted + Q waves persist
Weeks-mos: ST and T normalize; Q waves often persist permanently
MODULE 11 - Arrhythmias
Approach to Any Arrhythmia (systematic)
- Rate: Fast / slow / normal?
- Regular or irregular?
- QRS wide or narrow?
- P waves present? What is the relationship to QRS?
Narrow Complex Tachycardias (QRS < 120 ms)
| Arrhythmia | Rate | Rhythm | P waves | Key feature |
|---|---|---|---|---|
| Sinus tachycardia | 100-160 | Regular | Present, normal | Gradual onset/offset |
| Atrial flutter | 250-350 atrial; 150 ventricular (2:1) | Regular | Sawtooth in II, III, aVF | 150 bpm = think flutter |
| Atrial fibrillation | 100-160 ventricular | Irregularly irregular | No discrete P waves (fibrillatory baseline) | Most common sustained arrhythmia |
| AVNRT | 140-280 | Regular | P buried in QRS or just after | Pseudo-R' in V1, pseudo-S in II |
| AVRT (WPW) | 150-250 | Regular | Retrograde P after QRS | Delta wave in sinus rhythm |
| Atrial tachycardia | 150-250 | Regular | Abnormal P before QRS | Different P morphology |
| Multifocal atrial tachycardia | Variable >100 | Irregular | ≥3 different P wave morphologies | COPD patients |
Wide Complex Tachycardias (QRS ≥ 120 ms) - THE HIGH-STAKES AREA
Causes:
- VT (ventricular tachycardia) - most dangerous, assume this first
- SVT with aberrant conduction (LBBB/RBBB)
- SVT with pre-excitation (WPW with AF = most dangerous SVT)
- Pacemaker-mediated tachycardia
Rules:
If in doubt, treat wide complex tachycardia as VT until proven otherwise Never give adenosine or verapamil to pre-excited AF (WPW+AF) - can precipitate VF
Features favoring VT over SVT with aberrancy (Brugada criteria):
- AV dissociation (P waves marching independently) = definitive VT
- Capture beats (narrow QRS among wide) = definitive VT
- Fusion beats = definitive VT
- QRS duration > 160 ms
- Concordance (all precordial leads all-positive or all-negative)
- NW (extreme) axis deviation
Bradyarrhythmias
| Arrhythmia | ECG Feature | Management |
|---|---|---|
| Sinus bradycardia | Regular rhythm <60, P before each QRS | Treat if symptomatic: atropine, pacing |
| Sick Sinus Syndrome | SA dysfunction: Brady-tachy, sinus pauses, sinus arrest | PPM if symptomatic |
| Junctional escape | Narrow QRS, rate 40-60, P absent/inverted/retrograde | Treat underlying cause |
| Ventricular escape | Wide QRS, rate 20-40 | Emergency pacing |
Ventricular Arrhythmias
Premature Ventricular Complexes (PVCs):
- Wide (>120 ms), bizarre QRS
- No preceding P wave
- Compensatory pause
- Bigeminy (every other beat), trigeminy (every third)
Ventricular Tachycardia (VT):
- ≥3 consecutive wide QRS complexes at ≥100 bpm
- Sustained (>30 s) vs non-sustained (<30 s)
- Monomorphic (uniform QRS) vs polymorphic (varying QRS)
Torsades de Pointes:
- Polymorphic VT with twisting QRS axis around baseline
- Occurs with long QT (congenital or acquired)
- Triggers: hypokalemia, hypomagnesemia, drugs (class IA/III antiarrhythmics, antipsychotics, antibiotics like azithromycin)
- Treatment: IV magnesium sulfate; correct electrolytes; stop offending drug
Ventricular Fibrillation (VF):
- Chaotic, irregular deflections, no organized QRS
- No cardiac output = cardiac arrest
- Immediate defibrillation + CPR
MODULE 12 - Pre-excitation (WPW Syndrome)
ECG features (in sinus rhythm):
- Short PR interval (<120 ms) - bypass of AV node
- Delta wave - slurred upstroke of QRS
- Wide QRS (>110 ms) - fusion of normal and accessory pathway conduction
- ST-T changes secondary to abnormal depolarization
Accessory pathway location by delta wave polarity:
- Positive delta in V1-V3, negative in aVL = left-sided pathway (most common)
- Negative delta in II, III, aVF = posterior/inferior pathway
Danger: AF with pre-excitation. Very rapid ventricular response via accessory pathway (can conduct at >250 bpm) → VF. ECG shows irregular wide complex tachycardia with varying QRS. NEVER use digoxin, verapamil, diltiazem, adenosine (enhance accessory conduction or drop AVN without blocking AP). Use: DC cardioversion (if unstable) or procainamide / ibutilide.
MODULE 13 - Metabolic and Drug Effects
Hyperkalemia (sequential changes as K+ rises)
| K+ level (approx) | ECG change |
|---|---|
| 5.5-6.5 mEq/L | Peaked ("tented"), narrow T waves |
| 6.5-7.5 mEq/L | Prolonged PR, flattened P waves |
| 7.5-8.0 mEq/L | Wide QRS |
| >8.0 mEq/L | Sine-wave pattern → asystole |
Treatment: Calcium gluconate (membrane stabilization, immediate), insulin+dextrose, sodium bicarbonate, furosemide, kayexalate, dialysis.
Hypokalemia
- Flattened T waves
- Prominent U waves (U > T wave height = significant)
- Apparent QT prolongation (actually QU prolongation)
- Risk of Torsades
Hypercalcemia
- Shortened QT interval
- Short ST segment or absent ST
Hypocalcemia
- Prolonged QT (prolonged ST segment)
- T wave remains normal
Digoxin
- "Reverse tick" or "Salvador Dali mustache" ST depression (scooping)
- Shortened QT
- T wave flattening or inversion
- Digoxin toxicity: PAT with block, ventricular bigeminy, PVCs, AV blocks
Hypothermia
- Bradycardia
- Osborn (J) wave: positive deflection at J point (most visible in V5, V6)
- Prolonged PR, QRS, QT
- Shivering artifact
MODULE 14 - Pericarditis vs. STEMI
| Feature | Acute Pericarditis | STEMI |
|---|---|---|
| ST elevation | Diffuse (all/most leads) | Regional (contiguous leads) |
| ST morphology | Concave (saddle-shaped) | Convex (domed/tombstone) |
| PR depression | Present (classic) | Absent |
| Reciprocal ST depression | Absent (except aVR) | Present in opposite leads |
| Q waves | No | Develop over hours-days |
| Chest pain position | Pleuritic, worse lying, better leaning forward | Central, radiation to arm/jaw |
MODULE 15 - Pulmonary Embolism ECG
ECG is rarely diagnostic but supports clinical suspicion. Classic (but uncommon) finding:
S1Q3T3 pattern:
- Deep S wave in Lead I
- Q wave in Lead III
- T wave inversion in Lead III
Other PE ECG findings:
- Sinus tachycardia (most common sign)
- New RBBB (acute right heart strain)
- RAD
- T wave inversions V1-V4 (RV strain pattern)
- Atrial arrhythmias (AF, flutter)
- P pulmonale
MODULE 16 - The Brugada Pattern
Type 1 (Diagnostic):
- Coved (convex) ST elevation ≥2 mm in V1-V2
- Down-sloping ST segment followed by T wave inversion
- Spontaneous or drug-induced
Types 2 and 3: Saddleback or less elevation - not diagnostic alone
Clinical importance: Risk of sudden cardiac death from VF. Autosomal dominant SCN5A mutation (sodium channel). Fever, alcohol, certain drugs can unmask it.
MODULE 17 - The 14-Step Systematic ECG Approach (Exam and Clinical)
Use this for EVERY ECG. Never skip steps.
| Step | What to Assess | What to Look For |
|---|---|---|
| 1 | Calibration & technical | 1 mV = 10 mm, 25 mm/s, correct lead placement |
| 2 | Rhythm | Sinus? Regular? P before every QRS? |
| 3 | Heart rate | 300 rule for regular; count in 10 s for irregular |
| 4 | PR interval | 120-200 ms; short = WPW/junctional; long = AV block |
| 5 | QRS duration | <110 ms; wide = BBB, aberrancy, pacing, hyperK |
| 6 | QT/QTc interval | <450 ms men / <460 ms women |
| 7 | Mean QRS axis | I and aVF method; -30° to +90° normal |
| 8 | P waves | Morphology, size, axis - atrial hypertrophy? |
| 9 | QRS voltages | LVH? Low voltage (pericardial effusion, obesity, COPD)? |
| 10 | R-wave progression | V1 (small r) → V5 (tall R). Poor progression = anterior MI |
| 11 | Q waves | Pathological? Location? Old vs new? |
| 12 | ST segments | Elevation? Depression? Which leads? Shape? |
| 13 | T waves | Tall? Inverted? Symmetric? Asymmetric? |
| 14 | U waves | Prominent (hypokalemia, bradycardia)? |
Always compare with previous ECGs.
MODULE 18 - High-Yield Exam Mnemonics
| Mnemonic | What it's for |
|---|---|
| WILLIAM MARROW | BBB: W in V1 = LBBB; M in V1 = RBBB |
| 300-150-100-75-60-50 | Heart rate from R-R large squares |
| I See aVF (Both up = Normal axis) | Quick axis check |
| Longer, longer, longer, DROP | Wenckebach (Mobitz I) |
| DEAD | VT clues: Dissociation, Extreme axis, Absence of P-QRS relationship, Duration >160 ms |
| ABCDE for PE | Arrhythmia, BBB (RBBB), Cor pulmonale (P pulmonale), Deviation (RAD), S1Q3T3 |
| Tented T = hyperK; Flat T + prominent U = hypoK | Electrolytes |
| Concave ST = pericarditis; Convex ST = MI | Distinguishing causes of ST elevation |
| PR depression + ST elevation = pericarditis | Classic pericarditis ECG clue |
MODULE 19 - Quick Clinical Decision Rules
Chest pain + ECG → Action:
- ST elevation ≥1 mm in ≥2 contiguous leads → Activate cath lab (STEMI protocol) - door to balloon <90 min
- New LBBB + chest pain → Same as STEMI (Sgarbossa criteria)
- ST depression V1-V4 + inferior STEMI → Posterior MI; do V7-V9
- Inferior STEMI + hypotension + clear lungs → Rule out RV MI with V4R
Hemodynamically unstable tachycardia: Synchronized DC cardioversion regardless of type (except AF narrow complex without hemodynamic compromise)
VT vs SVT with aberrancy: When uncertain in unstable patient → cardiovert. When uncertain in stable patient → adenosine (if narrow) or amiodarone (safest for wide complex)
Prolonged QTc + syncope: Torsades de Pointes until proven otherwise. Give IV MgSO4. Stop QT-prolonging drugs. Correct K+ and Mg2+.
Suggested Study Order for Exams
- Paper calibration + waveform basics (Module 3, 4)
- Leads and normal ECG (Module 5, 6)
- Ischemia/STEMI localization (Module 10) - highest exam yield
- Bundle branch blocks (Module 8)
- AV blocks (Module 9)
- Arrhythmias systematic approach (Module 11)
- Metabolic effects (Module 13)
- Practice 14-step approach on real ECGs (Module 17)
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025), Chapter 247 - Electrocardiography; Fuster and Hurst's The Heart, 15th ed., Chapter on Cardiac Conduction System; Gray's Anatomy for Students.
Ask me about any module in more depth - arrhythmia identification, STEMI localization, specific drugs, or work through ECG cases together!
Give me all ecgs for stepwise learning with explanation
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I have all images verified and ready. Now composing the full visual ECG atlas:
ECG Visual Atlas: Stepwise Learning with Real ECGs
All ECGs sourced from Harrison's Principles of Internal Medicine (22nd ed.) and Rosen's Emergency Medicine.
LEVEL 1 - The Foundation
ECG 1: Normal Sinus Rhythm - Your Baseline
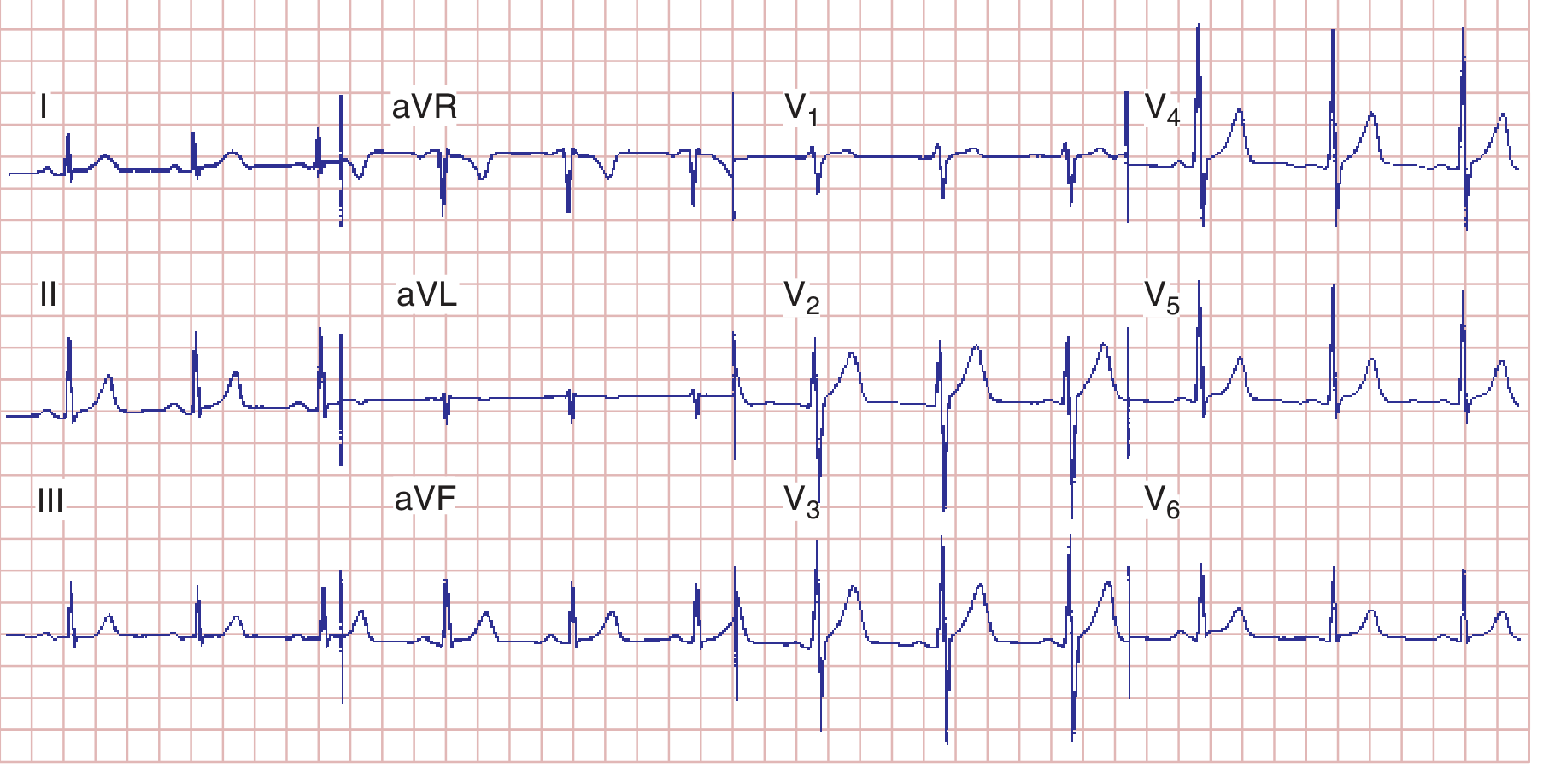
What you're seeing: This is the template every other ECG is compared against.
Step-by-step analysis:
| Feature | This ECG | Normal? |
|---|---|---|
| Rate | 75 bpm | ✅ 60-100 |
| Rhythm | Regular, P before every QRS | ✅ Sinus |
| PR interval | 160 ms (4 small squares) | ✅ 120-200 ms |
| QRS duration | 80 ms (2 small squares) | ✅ <110 ms |
| QT interval | 360 ms, QTc ~390 ms | ✅ <450 ms |
| Axis | ~+70° (upright in I and aVF) | ✅ Normal |
| R-wave progression | Small r in V1 → tall R in V5 | ✅ Normal |
Train your eye here first. Every abnormal ECG will deviate from this pattern in at least one way.
ECG 2: Ventricular Depolarization - How the QRS is Born
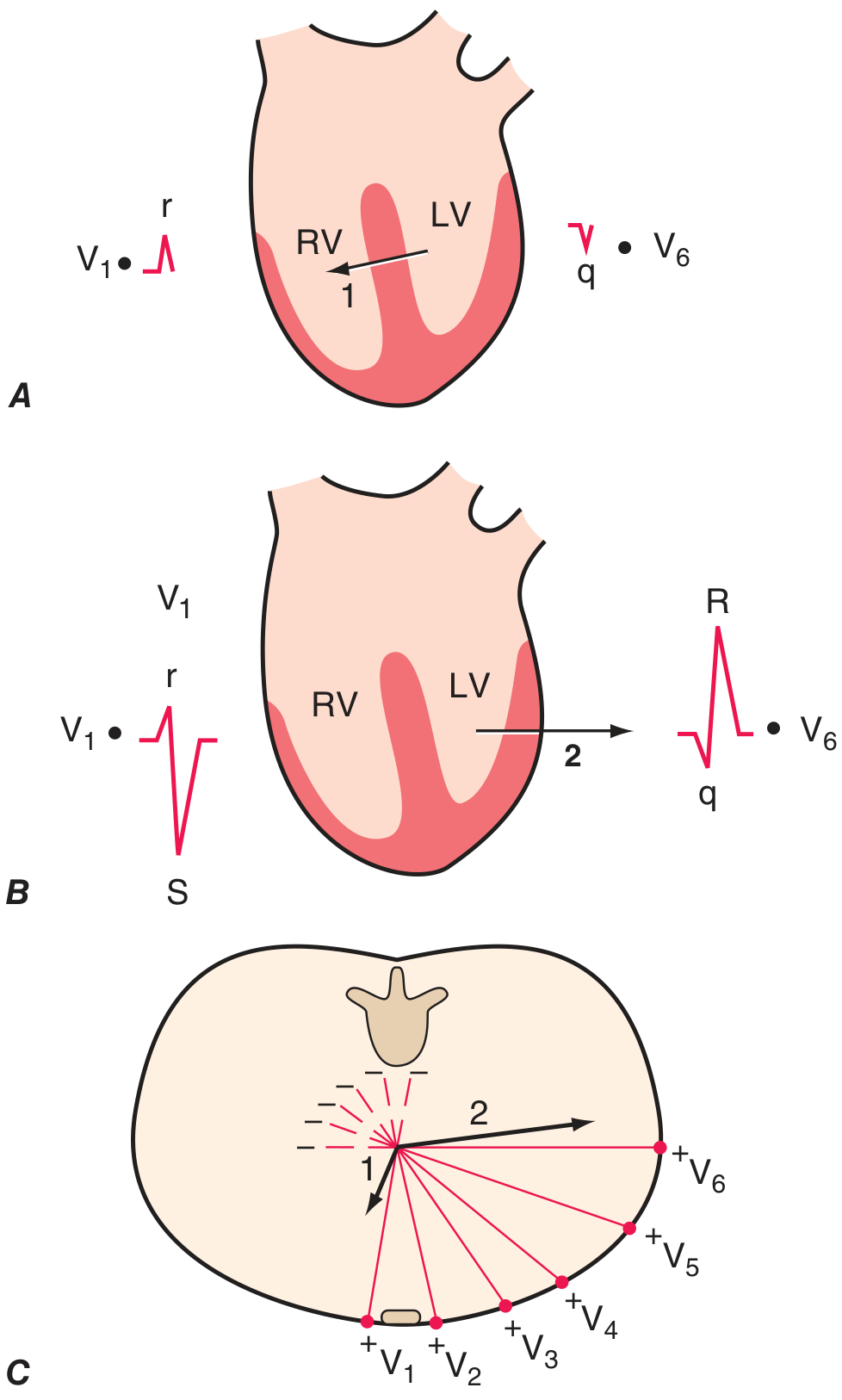
This diagram explains why V1 looks different from V6:
- Phase 1 (septum): Depolarizes left → right. V1 sees it coming → small upward r wave. V6 sees it going away → small downward q wave.
- Phase 2 (ventricles): LV dominates, vector swings left → right. V1 sees it going away → deep S wave. V6 sees it coming → tall R wave.
Result:
- V1 = rS (small r, big S)
- V6 = qR (tiny q, big R)
- V1 → V5 = R wave progressively gets bigger (R-wave progression)
Poor R-wave progression (R stays small across V1-V4) = anterior MI until proven otherwise.
LEVEL 2 - Atrial and Ventricular Enlargement
ECG 3: P Wave Morphology - Atrial Abnormalities
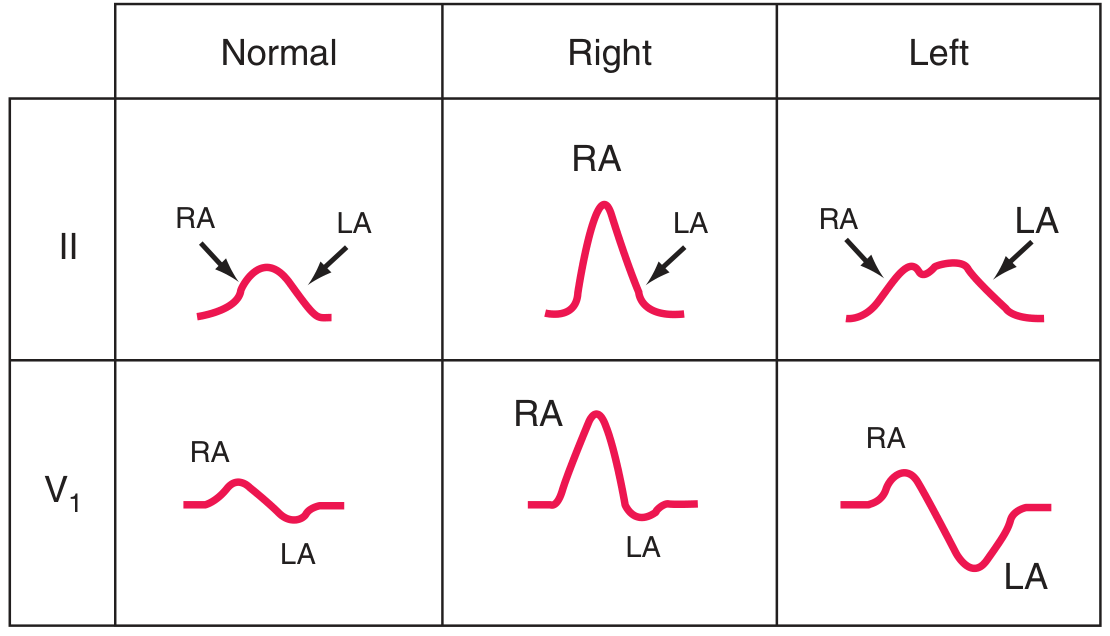
How to read this diagram:
| Lead II | Lead V1 | |
|---|---|---|
| Normal | Small, smooth P (RA then LA humps) | Small biphasic P |
| Right atrial enlargement | Tall (>2.5 mm), peaked P ("P pulmonale") | Large initial positive deflection |
| Left atrial enlargement | Broad (>120 ms), notched P ("P mitrale") | Large terminal negative component >1 mm² |
Clinical causes:
- RAE (P pulmonale): COPD, pulmonary hypertension, tricuspid stenosis, PE
- LAE (P mitrale): Mitral stenosis, mitral regurgitation, LVH, dilated cardiomyopathy
Exam pearl: In V1, the terminal (second) negative deflection = left atrial component. If it's >1 mm wide AND >1 mm deep = LAE.
ECG 4: LVH and RVH Patterns
The normal ECG above has normal voltages. For LVH/RVH, study the voltage criteria below:
LVH Criteria (Sokolow-Lyon):
- S in V1 + R in V5 or V6 ≥ 35 mm
- R in aVL ≥ 11 mm (women); ≥ 28 mm (men) - Cornell criteria
- LV strain pattern: ST depression + asymmetric T inversion in I, aVL, V5, V6
RVH Criteria:
- Dominant R wave in V1 (R ≥ S in V1)
- Right axis deviation (axis > +90°)
- RV strain pattern: T inversion in V1-V3
Memory: LVH = tall left; RVH = tall right (V1)
LEVEL 3 - Ischemia and Infarction (Highest Exam Yield)
ECG 5: The Mechanism of ST Deviation

This diagram is the conceptual key to all ischemia ECGs:
- Panel A (Subendocardial ischemia): Injury current vector points inward → leads overlying the LV see ST depression. This is NSTEMI/unstable angina territory.
- Panel B (Transmural/epicardial ischemia): Injury current vector points outward → leads overlying the zone see ST elevation. This is STEMI territory.
Think of it like a compass: The ST segment points toward the injured zone.
ECG 6: Anterior STEMI (LAD occlusion)
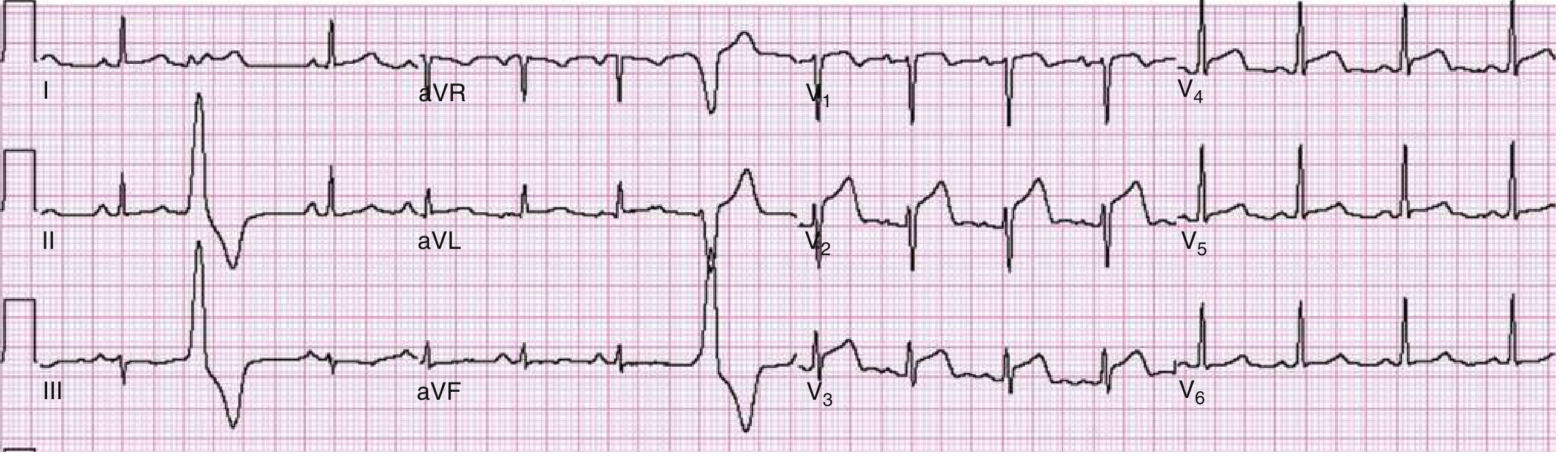
What you're seeing:
- ST elevation in V1-V4 (anteroseptal leads) - convex/oblique ST morphology
- Note the tall R waves progressing V1-V4, then cut short by the ST change
- This patient had a 90% LAD stenosis - went to cath lab immediately
Systematic read:
- Rate: ~70 bpm, sinus
- ST elevation: V1, V2, V3, V4 - ≥2 mm in V1-V3 = diagnostic STEMI
- Reciprocal changes: Look for ST depression in II, III, aVF (inferior leads)
- Q waves: May be developing - marker of established necrosis
- ACTION: Activate cath lab. Door-to-balloon time target: <90 min
ECG 7: Anterolateral STEMI (LAD + circumflex territory)
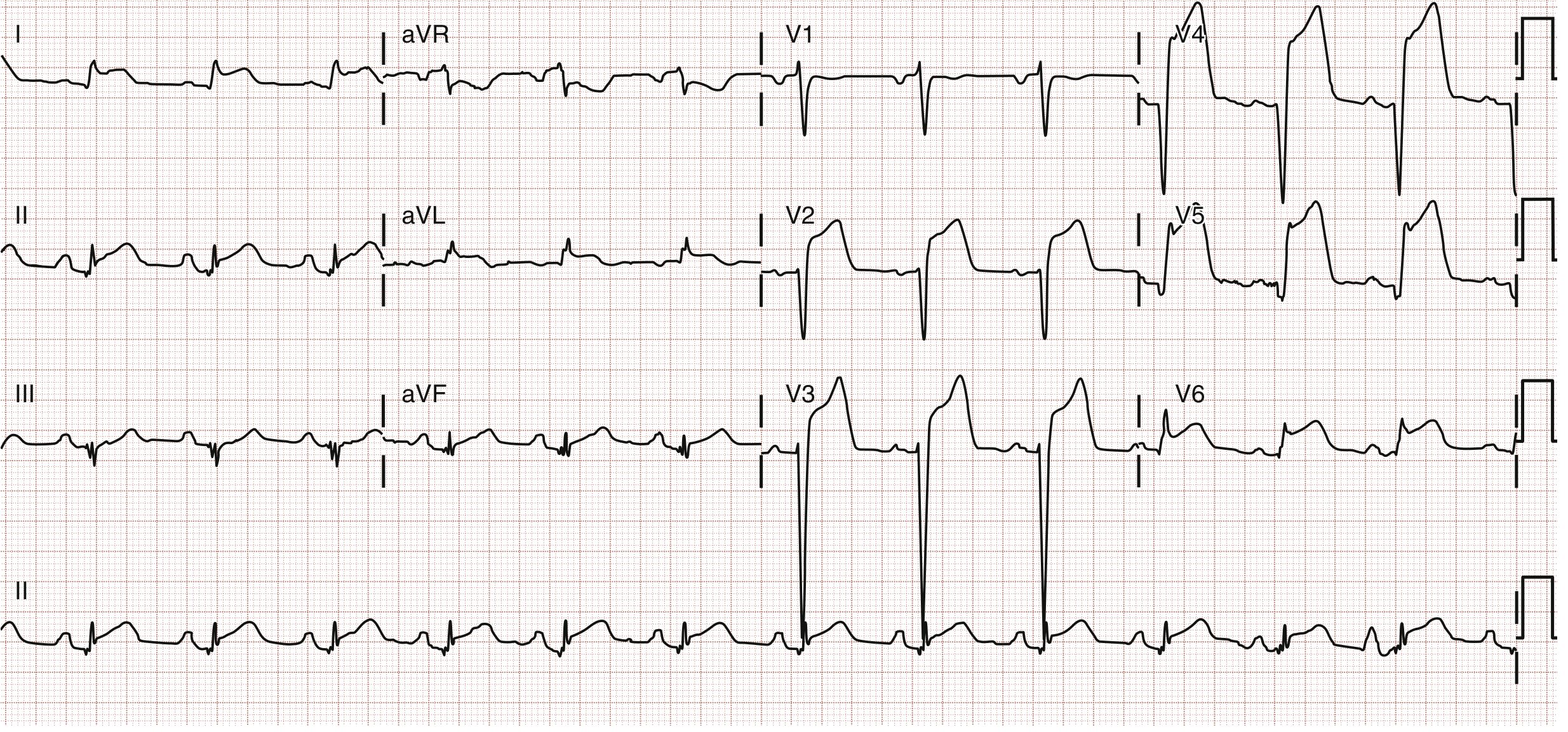
What you're seeing:
- ST elevation spreading across V2-V6, I, and aVL = extensive anterolateral territory
- This is a large territory MI - "widowmaker" territory (proximal LAD)
- Patient had in-stent thrombosis of previous LAD stent
Comparison with ECG 6:
| Feature | Anterior STEMI (ECG 6) | Anterolateral STEMI (ECG 7) |
|---|---|---|
| ST elevation | V1-V4 only | V2-V6 + I + aVL |
| Territory | Anteroseptal | Extensive anterior + lateral |
| Culprit | Mid-LAD | Proximal LAD or wrapping LAD |
| Severity | Significant | Very large - high risk |
ECG 8: Wellens Syndrome (Critical LAD Stenosis Warning)

This ECG can save a life - memorize it.
What you're seeing:
- Deep, symmetric T-wave inversions in V2-V4 (precordial leads)
- Note: no current ST elevation, R waves preserved (no Q waves yet)
- Patient had chest pain that may have resolved
Why this matters: This is the "reperfusion pattern" of a critical proximal LAD stenosis. The artery opened briefly, but will re-occlude causing massive anterior MI.
Wellens Type A: Biphasic T waves in V2-V3 (earlier stage)
Wellens Type B: Deep symmetric T inversions in V2-V4 (shown here - more advanced)
⚠️ DO NOT do a stress test on this patient - can precipitate VF and death. Refer urgently for coronary angiography.
ECG 9: Left Main / Proximal LAD Occlusion - aVR Elevation
What you're seeing:
- ST elevation in aVR > 1 mV (the lead pointing at the right shoulder / LV cavity)
- Widespread ST depression in most other leads (I, II, aVL, V4-V6 at minimum)
- This pattern = diffuse subendocardial ischemia from left main occlusion
Rule of thumb:
ST elevation in aVR + widespread ST depression elsewhere = Left main stenosis (78% sensitive, 83% specific) or severe proximal LAD disease
This is a cardiology emergency - highest-risk STEMI equivalent.
LEVEL 4 - Bundle Branch Blocks
ECG 10: RBBB vs LBBB - The WiLLiaM MaRRow Rule
The following shows the BBB patterns in V1 and V6:
| V1 | V6 | |
|---|---|---|
| RBBB | M-shaped (rSR') = rabbit ears | W-shaped (wide S) |
| LBBB | W-shaped (QS or rS) | M-shaped (broad notched R) |
Mnemonic: WiLLiaM MaRRow
- WiLLiam = LBBB has W in V1, M in V6
- MaRRow = RBBB has M in V1, W in V6
RBBB Diagnostic Criteria:
- QRS ≥ 120 ms
- rSR' ("rabbit ears") in V1
- Wide slurred S in I, aVL, V5, V6
- T wave inverted in V1-V2 (secondary - normal with RBBB, not ischemia)
LBBB Diagnostic Criteria:
- QRS ≥ 120 ms
- Broad monophasic R in I, aVL, V5, V6 (no Q wave, no S wave)
- Deep QS or rS in V1
- T wave inverted in I, aVL, V5, V6 (secondary - normal with LBBB)
Clinical significance:
- RBBB: Often benign; new RBBB in acute anterior MI = proximal LAD (septal branch involvement)
- LBBB: New LBBB + chest pain = treat as STEMI (modified Sgarbossa criteria)
Sgarbossa Criteria for MI in LBBB (score ≥ 3 = MI):
| Finding | Points |
|---|---|
| ST elevation ≥ 1 mm concordant with QRS (same direction) | 5 |
| ST depression ≥ 1 mm in V1-V3 | 3 |
| ST elevation ≥ 5 mm discordant with QRS | 2 |
LEVEL 5 - AV Blocks (Visual Patterns)
ECG 11-13: The Three AV Blocks
1st Degree AV Block:
P----P----P----P (every P conducts)
QRS QRS QRS QRS (every P has a QRS)
↕PR: >200ms (stretched but constant)
Benign. PR > 5 small squares. All P waves conduct.
2nd Degree - Mobitz I (Wenckebach):
P P P P P P P
QRS QRS QRS --- QRS QRS ---
PR: ↑ ↑↑ ↑↑↑ drop ↑ ↑↑ drop
PR gets longer and longer until a QRS is dropped, then resets. "Longer longer longer DROP."
- Benign, usually AV node level
- Common in athletes (high vagal tone) and inferior MI
2nd Degree - Mobitz II:
P P P P P P
QRS QRS --- QRS QRS ---
PR: = = = = (CONSTANT then sudden drop)
Fixed PR, then sudden non-conducted P without warning.
- Dangerous - below the AV node (His-Purkinje)
- Associated with wide QRS, anterior MI
- Requires pacemaker - high risk of complete block
3rd Degree (Complete AV Block):
P P P P P P P P (fast, ~70-80/min)
QRS QRS QRS QRS (slow, 30-50/min)
P waves and QRS complexes march completely independently.
- Narrow QRS escape = junctional (40-60/min) = AV node still working below block
- Wide QRS escape = ventricular (20-40/min) = dangerous, more hemodynamically unstable
- Emergency: atropine (narrow complex), transcutaneous pacing, urgent permanent pacemaker
LEVEL 6 - Metabolic ECGs (Must Know for Exams)
ECG 14: Hyperkalemia - The Deadly Progression
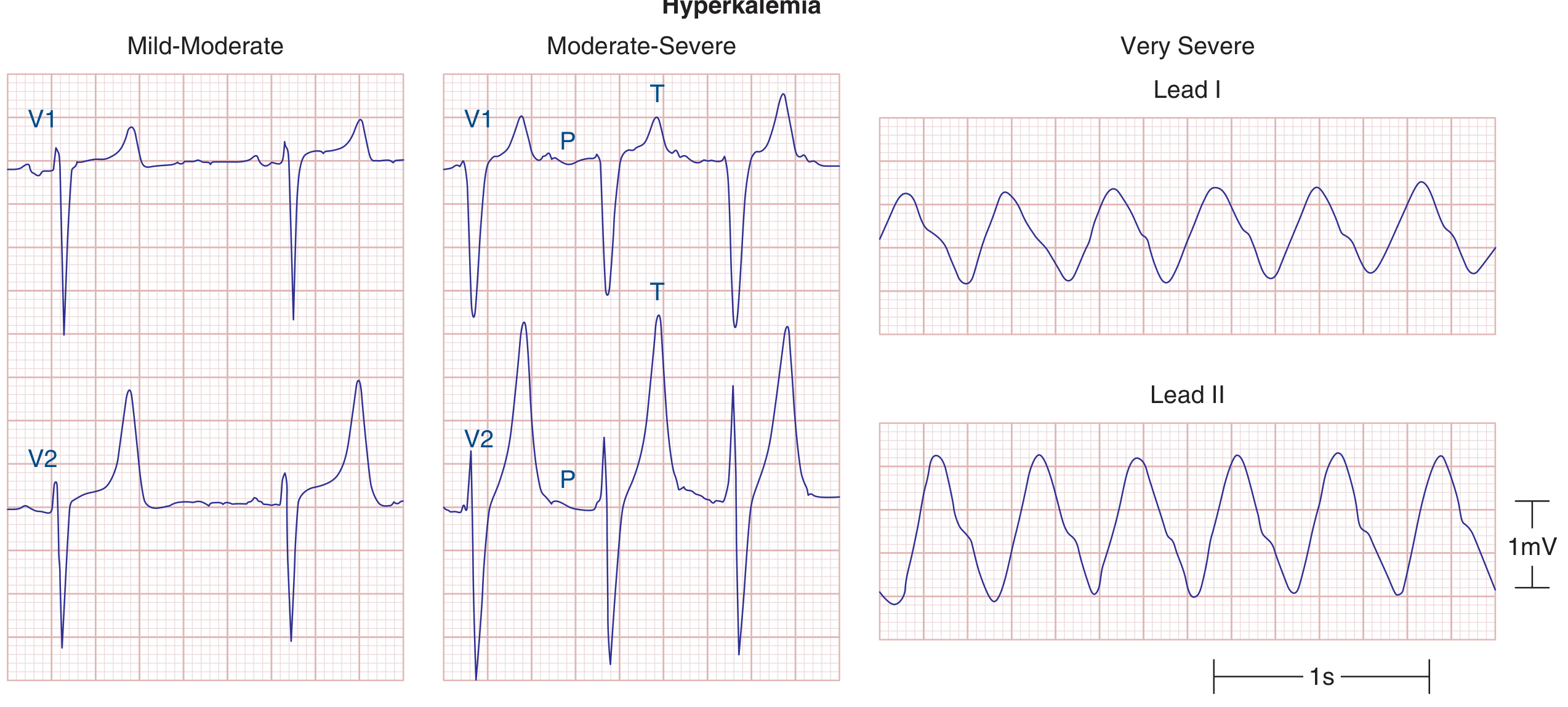
Read this image panel by panel:
| Panel | K+ Level | ECG Changes |
|---|---|---|
| Mild-Moderate (V1, V2 left panel) | 5.5-6.5 mEq/L | Tall, narrow, peaked ("tented") T waves - classic first sign |
| Moderate-Severe (V1, V2 middle panel) | 6.5-8 mEq/L | Wide QRS, flat/absent P waves, peaked T waves still visible |
| Very Severe (Lead I, II right panel) | >8 mEq/L | Sine wave pattern - imminent asystole |
Why this matters clinically:
- Peaked T waves = call for ECG immediately in any CKD/renal patient
- Sine wave = life-threatening emergency - give calcium gluconate NOW
- Treatment sequence: C-BIG-K-D (Calcium, Bicarbonate, Insulin+Glucose, Kayexalate, Dialysis)
ECG 15: Hypokalemia - The U Wave
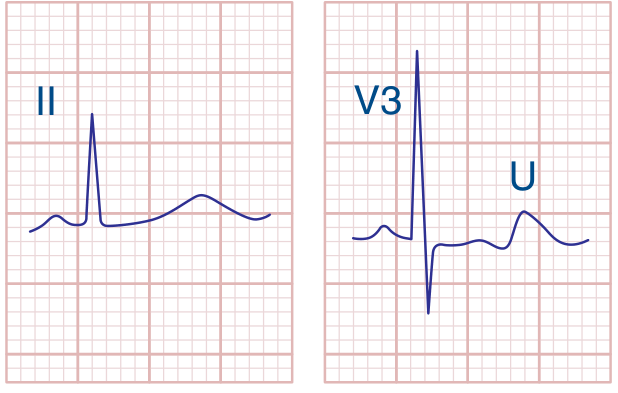
What you're seeing:
- Lead II (left): Flat T wave, barely visible, slight prolongation of the QT interval
- V3 (right): Prominent U wave labeled - note it is taller than the T wave in this lead
Key features of hypokalemia:
- T wave flattening → T wave inversion
- U wave prominence (U > T = significant hypokalemia)
- Apparent QT prolongation (actually QU prolongation - U wave merging with T)
- Risk: Torsades de Pointes especially if on QT-prolonging drugs
Causes to recognize: Diuretics (thiazide, loop), vomiting, diarrhea, Conn's syndrome, hypomagnesemia
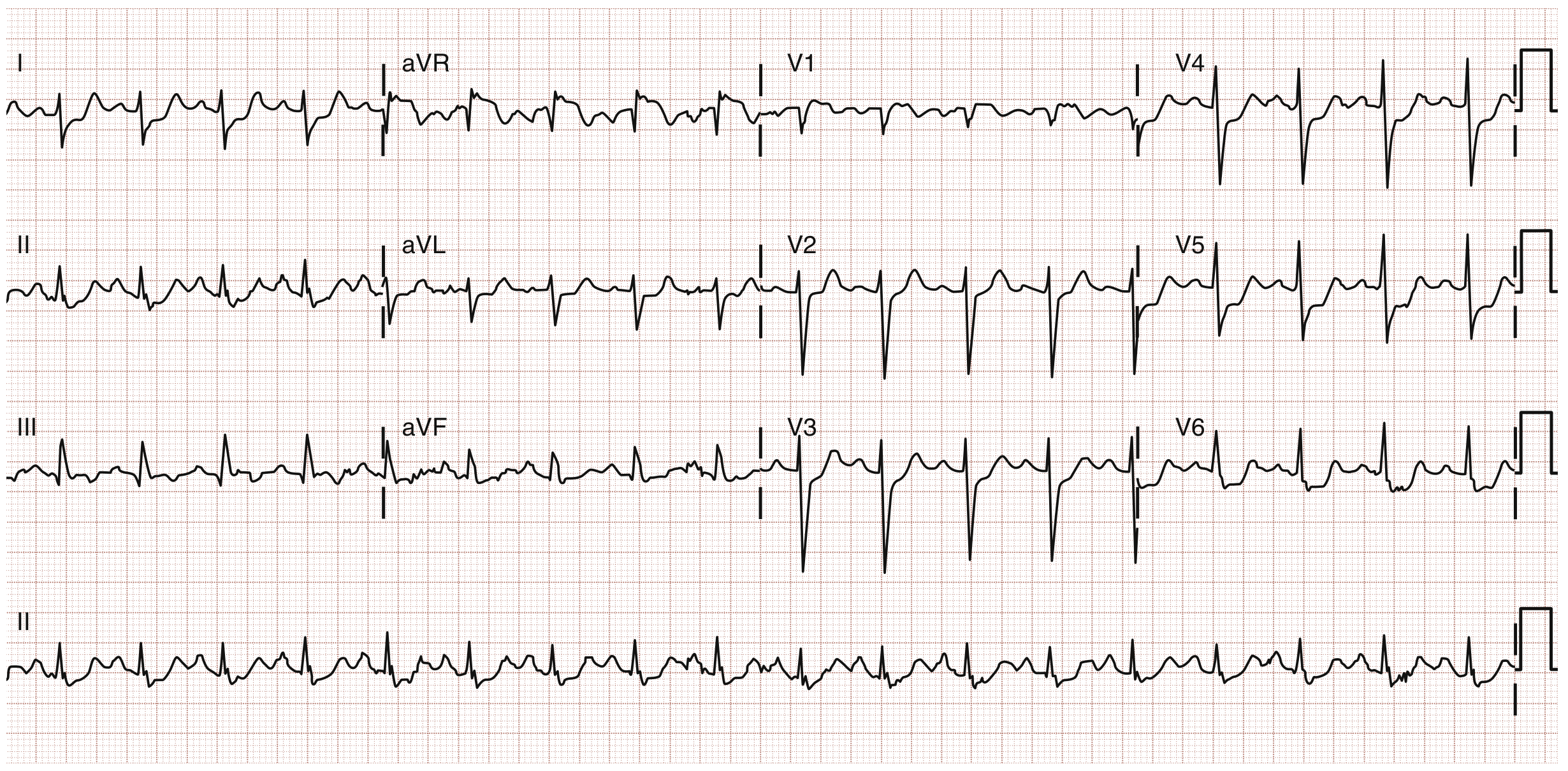
ECG 16: Pericarditis with Cardiac Tamponade - Electrical Alternans
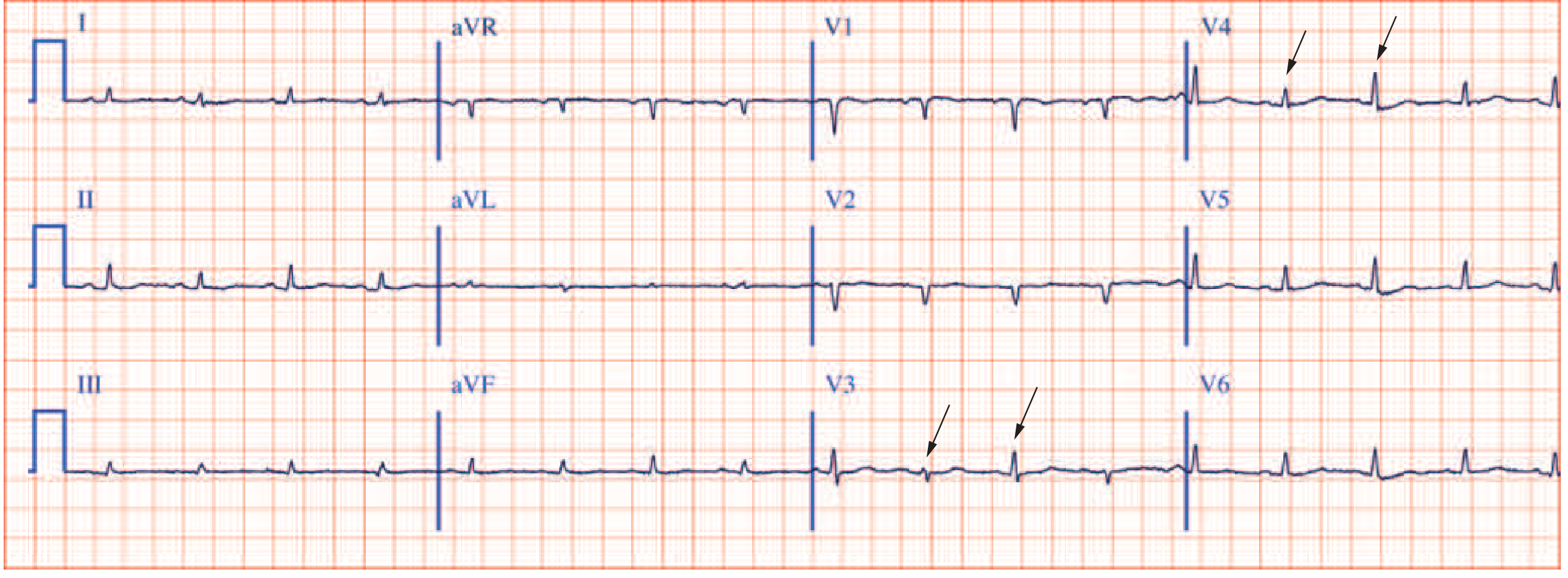
The classic triad of cardiac tamponade on ECG:
- Sinus tachycardia (compensatory, filling impaired)
- Low QRS voltage (<5 mm all limb leads and/or <10 mm chest leads) - fluid insulating the heart
- Electrical alternans - QRS height alternates every other beat (arrows in V2, V4) - heart swinging inside fluid
Acute pericarditis ECG features (before effusion develops):
- Diffuse saddle-shaped (concave) ST elevation in most leads (not just regional)
- PR segment depression (very specific for pericarditis)
- No reciprocal ST depression (except aVR)
- No Q waves
Pericarditis vs STEMI - the critical distinction:
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST shape | Concave (saddle) | Convex (dome/tombstone) |
| Distribution | Diffuse (all leads) | Regional (2+ contiguous) |
| PR depression | Present | Absent |
| Reciprocal ST depression | Absent | Present |
| Q waves | Never | Develop hours-days |
LEVEL 7 - Clinical Syndromes (Advanced)
ECG 17: Inferior STEMI - RCA Occlusion
What to look for:
- ST elevation in II, III, aVF (inferior leads)
- Reciprocal ST depression in I and aVL (lateral leads)
- III > II elevation = more likely RCA (proximal)
- II > III elevation = more likely LCx
Critical associated findings to always check:
- Right-sided leads (V3R, V4R): If ST elevation here = RV infarction (25-40% of inferior STEMIs)
- RV MI = give fluids (not nitrates!), no diuretics, no morphine
- Posterior leads (V7-V9) or V1-V2: Tall R + ST depression in V1-V2 = posterior extension
- Complete AV block: RCA supplies AV node - inferior MI can cause bradycardia / heart block
ECG 18: WPW (Wolff-Parkinson-White) Pattern
What to look for in sinus rhythm:
- Short PR (<120 ms) - bypassing the AV node
- Delta wave - slurred initial upstroke of QRS (most visible in lateral leads)
- Wide QRS (>120 ms) - fusion beat (normal + accessory pathway conduction)
- Pseudo-Q waves and ST-T changes - secondary to abnormal depolarization
Location of pathway by delta wave:
| Delta wave | Lead | Pathway location |
|---|---|---|
| Positive | V1-V3 | Left-sided (most common, type A) |
| Negative | V1 | Right-sided (type B) |
| Negative | II, III, aVF | Posterior/inferior |
The WPW arrhythmia danger:
- Orthodromic AVRT: Narrow complex tachycardia (down AV node, up AP) - treat with adenosine
- Antidromic AVRT: Wide complex tachycardia (down AP, up AV node)
- AF with WPW: Irregular wide complex tachycardia - VERY FAST rate (>250 bpm possible) → risk of VF
⚠️ Never give adenosine, digoxin, verapamil, diltiazem in AF+WPW - these block AV node but not accessory pathway, driving all conduction down the fast AP → VF Use: DC cardioversion (if unstable) or IV procainamide/ibutilide
ECG 19: Pulmonary Embolism - S1Q3T3
PE ECG findings (in order of frequency):
- Sinus tachycardia - most common, most sensitive
- T-wave inversions V1-V4 - right heart strain pattern (right precordial leads)
- New RBBB or RBBB morphology - acute RV pressure overload
- S1Q3T3 - classic but actually uncommon (<20% of PE cases)
- Right axis deviation
- P pulmonale - peaked P waves from acute RA overload
- Atrial fibrillation or flutter
S1Q3T3 breakdown:
- S in lead I (deep S = left lateral lead sees delayed RV activation)
- Q in lead III (inferior lead)
- T inversion in lead III (RV strain)
Exam tip: Normal ECG or just sinus tachycardia does NOT rule out PE. The most sensitive PE ECG finding is sinus tachycardia, not S1Q3T3. ECG in PE is used to increase/decrease probability, not diagnose.
ECG 20: Brugada Pattern
Type 1 (Diagnostic - the only one that counts):
- Coved ST elevation ≥ 2 mm in V1 (and sometimes V2)
- Down-sloping ST segment
- T wave inversion in V1
Types 2 and 3: Saddleback pattern - not diagnostic without Type 1 either spontaneous or after sodium channel blocker challenge
Clinical importance:
- Risk of sudden cardiac death from VF (especially at night, during fever)
- Sodium channel mutation (SCN5A - autosomal dominant)
- Unmasked by: fever, cocaine, alcohol, flecainide, procainamide (sodium channel blockers)
- Treatment: ICD (implantable cardioverter defibrillator) for symptomatic patients
- Quinidine for recurrent VF episodes or fever-triggered events
LEVEL 8 - Arrhythmia Recognition (Rhythm Strips)
How to Systematically Approach Any Rhythm Strip
Use this 4-question framework every time:
1. RATE → Fast? Slow? Normal?
2. REGULAR? → Measure R-R intervals
3. QRS WIDTH → Narrow (<120ms) or Wide (≥120ms)?
4. P WAVES → Present? Before QRS? Normal morphology?
Arrhythmia Quick Recognition Table
| Arrhythmia | Rate | Regular? | QRS | P waves | Distinguishing Feature |
|---|---|---|---|---|---|
| Sinus tach | 100-160 | Yes | Narrow | Normal, before QRS | Gradual onset, normal P morphology |
| AF | 100-160 ventricular | No (irregularly irregular) | Narrow | Absent (fibrillatory baseline) | Irregularly irregular, no P waves |
| AFL | 150 ventricular | Yes (usually 2:1) | Narrow | Sawtooth in II, III, aVF | Rate 150 = think flutter! |
| AVNRT | 150-250 | Yes | Narrow | Buried in QRS or pseudo-R' in V1 | Abrupt onset/offset, no visible P |
| AVRT (WPW) | 150-250 | Yes | Narrow (or wide) | Retrograde P after QRS | Delta wave in sinus rhythm |
| VT | >100 | Yes | Wide (≥120ms) | Dissociated (march independently) | AV dissociation = definitive VT |
| VF | Chaotic | No | No organized QRS | None | No output - cardiac arrest |
| Torsades | Variable | No | Wide, twisting | None visible | QRS alternates direction around baseline |
| 1° AVB | Any | Yes | Normal | Normal | PR >200ms, all P's conduct |
| Wenckebach | Normal-slow | Grouped beating | Normal | Some P's blocked | Progressive PR then dropped QRS |
| Mobitz II | Normal-slow | Mostly | Normal/Wide | Sudden blocked P | Fixed PR, sudden drop |
| 3° AVB | Slow ventricular | P regular, QRS regular but different rates | Wide or narrow | Dissociated from QRS | P rate > QRS rate, independent |
The Wide Complex Tachycardia Decision Tree
Wide Complex Tachycardia (QRS ≥120ms, Rate >100)
↓
Is patient UNSTABLE? (hypotensive, altered consciousness, pulmonary edema)
YES ──────────────────→ SYNCHRONIZED DC CARDIOVERSION
↓NO
Look for AV Dissociation?
YES ──────────────────→ DEFINITELY VT → Amiodarone or Cardioversion
↓NO
Capture beats or Fusion beats?
YES ──────────────────→ DEFINITELY VT → Amiodarone
↓NO
Brugada morphology criteria? QRS >160ms? Concordance?
YES ──────────────────→ LIKELY VT → Amiodarone
↓NO
Could this be AF + WPW? (irregular wide complex + very fast)
YES ──────────────────→ Procainamide or Cardioversion (NOT adenosine/verapamil)
↓NO
LIKELY SVT with aberrancy → Adenosine trial (have crash cart ready)
Rule: When uncertain, treat wide-complex tachycardia as VT. Adenosine is safe for narrow complex. For wide complex, amiodarone is the safest drug.
LEVEL 9 - Special ECG Patterns (Exam Favourites)
Quick Pattern Recognition Summary
| Pattern | Key ECG Finding | Diagnosis |
|---|---|---|
| Sawtooth waves in II, III, aVF at 300/min | Flutter waves | Atrial flutter |
| Irregularly irregular, no P waves | AF | Atrial fibrillation |
| Short PR + delta wave + wide QRS | Pre-excitation | WPW syndrome |
| Coved ST elevation V1-V2 | Type 1 Brugada | Brugada syndrome |
| Peaked T waves → wide QRS → sine wave | Hyperkalemia | Severe hyperkalemia |
| Prominent U waves, flat T | Hypokalemia | Hypokalemia |
| Diffuse concave ST + PR depression | Pericarditis | Acute pericarditis |
| Regional convex ST elevation | Ischemic injury | STEMI |
| Electrical alternans + low voltage + tachycardia | Tamponade | Cardiac tamponade |
| S1Q3T3 + sinus tachycardia + new RBBB | PE pattern | Pulmonary embolism |
| Deep T inversions V2-V4 + no ST elevation | Wellens | Critical LAD stenosis |
| ST elevation V1-V2 + aVR > ST in other leads | Left main / proximal LAD | Left main disease |
| J wave (Osborn wave) at J point | Hypothermia | Hypothermia |
| Scooping ST depression + short QT | Digoxin effect | Digoxin |
| Prolonged QT + polymorphic VT | Torsades | Long QT syndrome |
Clinical Practice Summary Card
Every ECG you pick up, run through this checklist in 30 seconds:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
1. RATE → Count (300 rule) / Irregular → count × 6
2. RHYTHM → P before QRS? Regular? Sinus?
3. PR → 120-200ms? Short (WPW)? Long (AVB)?
4. QRS → <110ms? Wide (BBB/VT/pace)?
5. AXIS → I and aVF upright = normal
6. ST SEGMENTS → Elevation (which leads)? Depression?
7. T WAVES → Inverted (where)? Peaked (hyperK)?
8. QT → Prolonged (drugs/electrolytes/long QT)?
9. P WAVES → Peaked (RAE)? Broad (LAE)?
10. U WAVES → Prominent (hypoK)?
11. COMPARE → With previous ECG!
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Sources: Harrison's Principles of Internal Medicine 22nd ed. (2025) Ch. 247 - Electrocardiography; Rosen's Emergency Medicine 9th ed. Ch. 64 - Acute Coronary Syndromes; Tintinalli's Emergency Medicine.
Next steps: Want me to drill you with ECG cases (show ECG → you diagnose → I explain), or go deeper on any specific pattern - arrhythmias, STEMI localization, BBBs, or electrolyte changes?
This is a shared conversation. Sign in to Orris to start your own chat.