Difference between ulcer and wound
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from the textbooks. Here is a thorough comparison:
Wound vs. Ulcer
Definitions
Wound
A wound is any disruption of tissue integrity — it is a broad term encompassing any break caused by physical, mechanical, chemical, thermal, or surgical means. By definition, wounding disrupts tissue integrity, leading to division of blood vessels and direct exposure of the extracellular matrix. — Schwartz's Principles of Surgery, 11e
Ulcer
An ulcer is specifically a break in the continuity of the covering epithelium — skin or mucous membrane — which may follow molecular death of the surface epithelium or its traumatic removal. — S. Das: A Manual on Clinical Surgery, 13e
In short: All ulcers are wounds, but not all wounds are ulcers. An ulcer is a specific type of wound defined by epithelial loss with underlying tissue exposure, typically persisting due to an underlying pathological cause.
Key Differences at a Glance
| Feature | Wound | Ulcer |
|---|---|---|
| Definition | Any disruption of tissue integrity | Loss of epithelial continuity (skin/mucosa) |
| Cause | Acute trauma, surgery, burns, lacerations | Ischemia, venous stasis, neuropathy, infection, malignancy |
| Onset | Usually acute | Acute or (more often) chronic/spontaneous |
| Healing tendency | Normally heals in predictable phases | Often fails or is slow to heal due to underlying pathology |
| Time course | Acute: heals within ~3 weeks | Chronic: > 3 weeks; may persist for months/years |
| Tissue layers affected | Can involve any layer (skin, muscle, bone) | Primarily epithelium + dermis ± deeper tissue |
| Underlying cause | Usually mechanical disruption | Usually systemic disease or vascular insufficiency |
| Pain | Usually present | Variable — absent in neuropathic/trophic ulcers |
| Infection risk | Depends on classification (clean vs. contaminated) | High; often colonized chronically |
| Examples | Laceration, surgical incision, abrasion, burn | Venous ulcer, arterial ulcer, pressure ulcer, diabetic ulcer, peptic ulcer, tuberculous ulcer |
Wound Healing Phases (Wounds)
Wounds heal through three overlapping phases (Schwartz's / Cummings Otolaryngology):
- Hemostasis & Inflammation — Platelet aggregation, fibrin clot formation, neutrophil and macrophage infiltration (peaks at 24–96 h)
- Proliferation — Fibroblast migration, collagen synthesis, angiogenesis, epithelialization
- Maturation & Remodeling — Collagen reorganization; wound strength reaches ~80% of normal at 3 months; remodeling continues 1–2 years
An acute wound becomes a chronic wound when healing is delayed beyond 3 weeks, or when it fails to return to anatomic integrity. Chronic wounds show:
- Decreased keratinocyte and fibroblast migration
- Elevated proteases and reactive oxygen species
- Senescent cells unresponsive to growth factors
- Microbial colonization
Types of Ulcers
Clinical classification (Das):
| Type | Description |
|---|---|
| Spreading ulcer | Inflamed edge, purulent slough, no granulation tissue, painful |
| Healing ulcer | Pink/red granulation, serous discharge, bluish epithelializing margin |
| Callous (chronic) ulcer | Pale granulation or wash-leather slough, scanty discharge, indurated base — refuses to heal |
Pathological classification (Das):
- Traumatic — mechanical, physical (burn/radiation), chemical
- Arterial — atherosclerosis, Buerger's disease, Raynaud's
- Venous — varicose/post-phlebitic (typically medial malleolus)
- Neurogenic/Trophic — pressure ulcers, perforating ulcers (sensory neuropathy, e.g., diabetes, tabes dorsalis)
- Nutritional/Systemic — tropical ulcers, diabetic ulcers, gouty ulcers
- Specific (infective) — tuberculous, syphilitic (gummatous/chancre), actinomycosis
- Malignant — squamous cell carcinoma, Marjolin's ulcer (arising in burn scar), rodent ulcer (BCC)
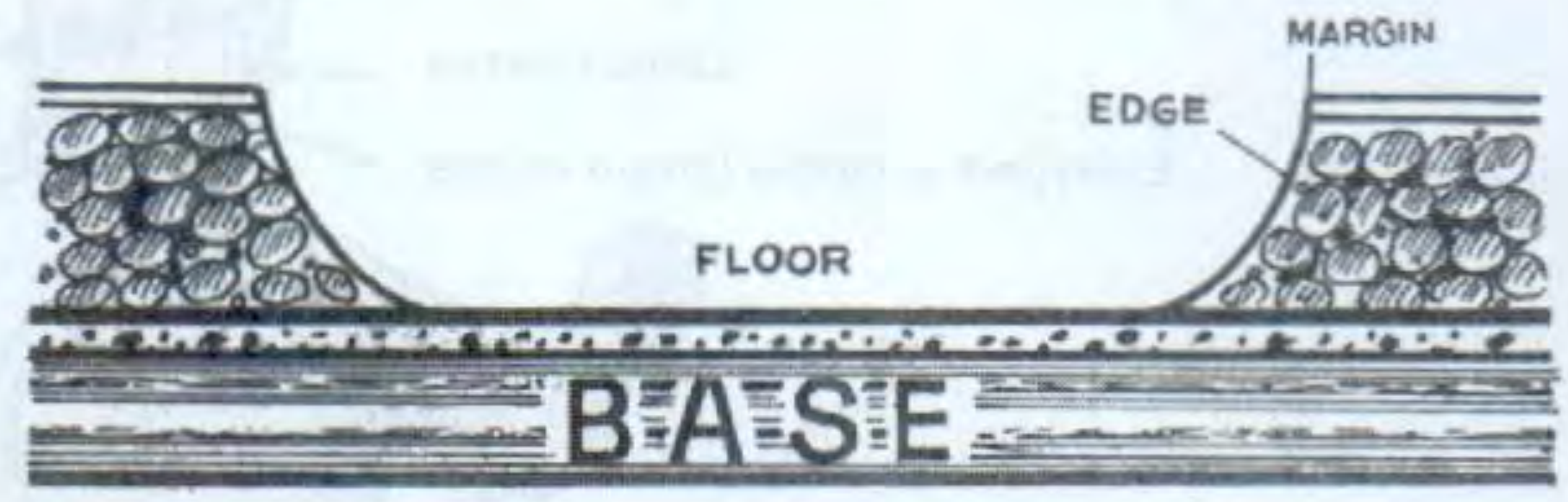
Parts of an Ulcer
An ulcer has distinct anatomical parts that aid diagnosis (Das):
- Margin — junction of normal epithelium with ulcer edge
- Edge — between margin and floor; varies by type (undermined = TB; everted = carcinoma; sloping = healing traumatic)
- Floor — base of the ulcer visible from above (red granulation = healing; wash-leather slough = gumma)
- Base — the tissue on which the ulcer rests (indurated = carcinoma; bone = trophic ulcer)
Clinical Takeaway
A wound is the overarching term — any tissue disruption from any cause, expected to heal. An ulcer implies a specific pathological process: loss of epithelial covering that persists because of an underlying systemic, vascular, neurological, or infective condition. Management therefore targets not only the local wound bed but also the underlying cause (e.g., revascularization for arterial ulcers, compression for venous ulcers, offloading for diabetic neuropathic ulcers).
This is a shared conversation. Sign in to Orris to start your own chat.