Enumerate the descending tracts of the spinal cord. Describe in detail the pyramidal tract. Mention its function and effects of lesion at different levels
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive information from multiple authoritative textbooks and two excellent diagrams. Let me compile the full detailed answer.
Descending Tracts of the Spinal Cord
(Sources: Gray's Anatomy for Students, Guyton & Hall Medical Physiology, Bradley & Daroff's Neurology in Clinical Practice)
I. Enumeration of Descending Tracts
Descending tracts are organized into two motor systems: lateral and medial.
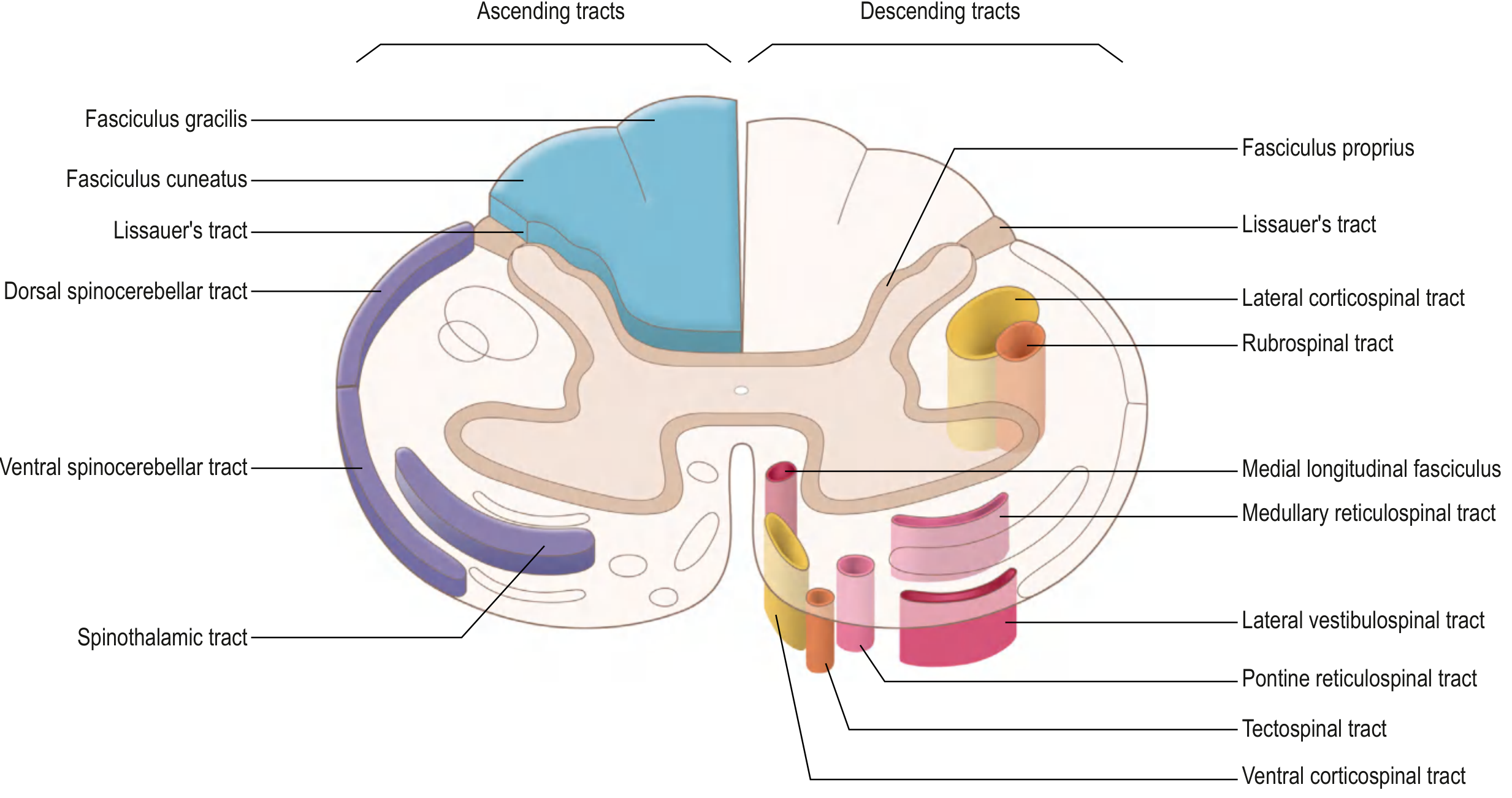
Lateral Motor System (lateral column)
| Tract | Origin | Decussation | Termination | Function |
|---|---|---|---|---|
| Lateral corticospinal tract | Primary motor cortex | Pyramidal decussation at cervicomedullary junction | Entire cord (mainly cervical + lumbosacral enlargements) | Voluntary movement of contralateral limbs |
| Rubrospinal tract | Red nucleus (magnocellular division), midbrain | Ventral tegmental decussation (midbrain) | Cervical cord | Movement of contralateral limbs (minor role in humans) |
Medial Motor System (anterior column)
| Tract | Origin | Decussation | Termination | Function |
|---|---|---|---|---|
| Anterior (ventral) corticospinal tract | Primary motor cortex + SMA | None (crosses at cord level) | Cervical + upper thoracic cord | Bilateral axial and girdle muscles |
| Vestibulospinal tract (lateral) | Lateral vestibular nucleus (Deiters) | None (ipsilateral) | Full length of cord | Facilitates extensors, inhibits flexors; balance |
| Pontine (medial) reticulospinal tract | Reticular formation, pons | Ipsilateral | Full cord | Facilitates voluntary movement, postural tone |
| Medullary (lateral) reticulospinal tract | Reticular formation, medulla | Ipsilateral | Full cord | Regulates voluntary movement and reflex activity |
| Tectospinal tract | Superior colliculus, midbrain | Dorsal tegmental decussation | Cervical cord only | Reflex head/neck turning to visual/auditory stimuli |
The fasciculus proprius (propriospinal tract) contains both ascending and descending fibers and connects cord segments for intersegmental reflexes.
II. The Pyramidal Tract - Detailed Description
Definition and Nomenclature
The pyramidal tract - more precisely called the corticospinal tract - is the most clinically important descending pathway. It gets the name "pyramidal" from the pyramid-shaped swellings it forms on the ventral surface of the medulla oblongata.
A. Origin (Cortical Contributions)
The corticospinal tract does not arise solely from the motor cortex. Its fibers come from:
- ~30% - Primary motor cortex (precentral gyrus, area 4)
- ~30% - Premotor cortex and supplementary motor area (area 6)
- ~40% - Somatosensory areas posterior to the central sulcus (areas 3, 1, 2)
The most important neurons of origin are the Betz cells (giant pyramidal cells) of the primary motor cortex. Key facts about Betz cells:
- ~60 µm in diameter
- ~34,000 Betz cell fibers per corticospinal tract
- Axon diameter ~16 µm; conduction velocity ~70 m/sec (fastest signals from brain to cord)
- Represent only 3% of all corticospinal fibers
- The remaining 97% are fibers <4 µm in diameter carrying tonic background signals
Total fibers per corticospinal tract: >1 million
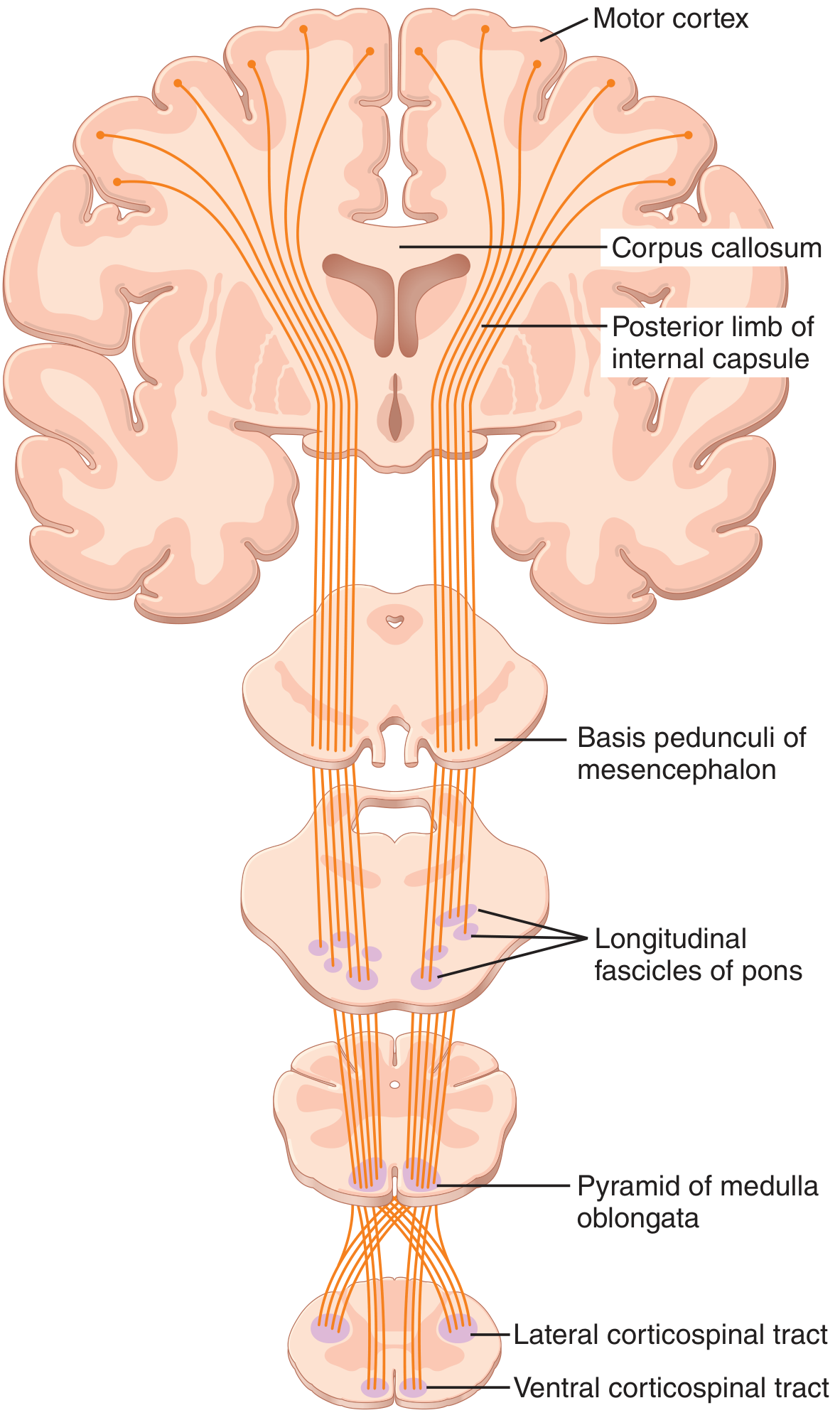
B. Course Through the Brain
Cerebral cortex → Corona radiata → Posterior limb of the internal capsule
- The internal capsule carries corticospinal fibers in a somatotopic arrangement: face and arm anteriorly, leg posteriorly
Internal capsule → Crus cerebri (basis pedunculi) of the midbrain
- Occupies the middle 3/5 of the crus cerebri
Crus cerebri → Pons
- Fibers break into small bundles within the basis pontis to accommodate transverse pontocerebellar fibers
Pons → Medullary pyramid
- Fibers regroup at the medulla to form the prominent ventral pyramids
Pyramidal decussation (cervicomedullary junction)
- ~75-90% of fibers cross the midline → form the lateral corticospinal tract
- ~10-25% remain uncrossed → form the anterior (ventral) corticospinal tract
C. Course in the Spinal Cord
Lateral corticospinal tract:
- Located in the lateral funiculus (white matter)
- Descends the full length of the spinal cord
- Terminates predominantly at cervical and lumbosacral enlargements
- Synapses mainly on interneurons in the intermediate zone (Rexed laminae V-VII), with some direct connections to anterior horn motor neurons (lamina IX) - especially for fine finger movements
Anterior corticospinal tract:
- Located in the anterior funiculus
- Extends only to cervical and upper thoracic cord
- Many fibers eventually cross at segmental level via anterior white commissure before synapsing
- Controls bilateral axial and girdle musculature
D. Fiber Composition and Somatotopy
Within the lateral corticospinal tract, there is somatotopic organization: cervical (arm) fibers are medial, lumbar (leg) fibers are lateral. This is clinically relevant in spinal cord compression - lateral lesions first affect the legs, medial lesions first affect the arms.
E. Corticobulbar Component
Strictly, the "pyramidal tract" includes:
- Corticospinal fibers (to spinal cord motor neurons)
- Corticobulbar fibers (to cranial nerve nuclei III-XII in the brainstem)
Most corticobulbar fibers are bilateral, except for the lower face (CN VII, contralateral only) and the tongue (CN XII, mainly contralateral) - relevant for distinguishing UMN vs. LMN facial palsy.
III. Functions of the Pyramidal Tract
- Voluntary skilled movements - especially fine, fractionated movements of the distal limbs (fingers, hand), which require direct corticomotoneuronal connections
- Speed and precision of movement - fast-conducting Betz cell axons allow rapid initiation of voluntary acts
- Contralateral limb control - lateral corticospinal tract governs contralateral extremities
- Modulation of sensory input - fibers to the dorsal horn modulate incoming sensory signals (sensory gating)
- Muscle tone regulation - descending cortical signals maintain appropriate background excitability of alpha and gamma motor neurons
- Fractionated finger movements - the most evolved function, dependent on direct monosynaptic corticomotoneuronal projections
IV. Effects of Lesion at Different Levels
Distinguishing Features: UMN vs. LMN
Before discussing levels, note that a pyramidal tract lesion at any supraspinal or spinal level above the anterior horn cell produces Upper Motor Neuron (UMN) signs:
| Feature | UMN (Pyramidal) Lesion | LMN Lesion |
|---|---|---|
| Muscle tone | Spasticity (clasp-knife) | Flaccidity |
| Reflexes | Hyperreflexia | Hyporeflexia/absent |
| Plantar response | Extensor (Babinski +) | Flexor (normal) |
| Wasting/fasciculations | Absent (mild disuse atrophy late) | Present |
| Distribution | Pyramidal pattern (extensors in UL, flexors in LL weak) | Segmental/peripheral nerve pattern |
Note: Immediately after an acute pyramidal lesion, spinal shock occurs - transient flaccidity, areflexia, and absent Babinski. Spasticity develops over days to weeks.
Level 1: Internal Capsule
- Contralateral hemiplegia (face, arm, and leg - the homunculus is compact here)
- Corticobulbar involvement causes contralateral lower facial weakness (forehead spared - bilateral supply) and tongue deviation toward the weak side
- Due to tight packing: a small lesion (e.g., lacunar infarct) causes dense hemiplegia - "pure motor stroke"
- Signs: contralateral spastic hemiplegia, hyperreflexia, Babinski sign, dysarthria
Level 2: Midbrain (Crus Cerebri)
- Ipsilateral CN III palsy (ptosis, mydriasis, "down-and-out" gaze) + contralateral hemiplegia = Weber's syndrome
- This occurs because the oculomotor nerve exits medially, adjacent to the descending corticospinal fibers in the crus cerebri
Level 3: Pons
- Ipsilateral CN VI and/or VII palsy + contralateral hemiplegia = Millard-Gubler syndrome (lesion in the basis pontis)
- Ipsilateral CN VI palsy + contralateral hemiplegia = Foville's syndrome (more posterior lesion)
Level 4: Medulla (Pyramid)
- Lesion at or just above the decussation: contralateral hemiplegia (arm and leg) with NO cranial nerve involvement (the pyramids are below CN nuclei)
- Ipsilateral pyramid lesion BELOW the decussation: ipsilateral weakness (rare, before crossing)
- Anterior spinal artery territory infarct: bilateral pyramidal signs + loss of pain/temperature (spinothalamic involved) with dorsal column sparing = medial medullary syndrome
Level 5: Cervical Spinal Cord (above C5)
Complete transection above C5:
- Quadriplegia (all 4 limbs)
- UMN signs below the lesion level
- LMN signs at the level of the lesion (destruction of anterior horn cells at that segment)
- Above C3-C5: respiratory failure (phrenic nerve involvement, diaphragm paralysis)
- Loss of all sensation below the level
- Bladder and bowel dysfunction (initially retention, later automatic/reflex bladder)
Hemisection of cervical cord (Brown-Séquard syndrome):
- Ipsilateral spastic weakness and loss of proprioception/vibration below lesion
- Contralateral loss of pain and temperature below lesion (one to two levels lower)
- Ipsilateral LMN signs at the level of the lesion
Level 6: Thoracic Spinal Cord (T1-T12)
- Paraplegia (lower limbs only - arms are normal, as corticospinal fibers to arms have already exited at cervical level)
- UMN signs in lower limbs: spasticity, hyperreflexia, Babinski sign
- Sensory loss with a dermatomal sensory level
- Bladder/bowel dysfunction; autonomic dysfunction
- At T1: may have Horner syndrome (disruption of sympathetic pathway)
- Above T6: risk of autonomic dysreflexia (exaggerated sympathetic response to stimuli below the lesion)
Level 7: Lumbar Spinal Cord (L1-L5)
- Paraplegia of lower limbs; may be UMN (conus intact) or mixed UMN+LMN depending on exact level
- Below the conus medullaris (L1-L2 in adults), lesions are technically cauda equina (LMN) - flaccid paralysis, areflexia, bladder/bowel dysfunction of LMN type (overflow incontinence, impotence)
Level 8: Sacral Cord / Conus Medullaris
- LMN bladder and bowel (atonic bladder, fecal incontinence)
- Saddle anesthesia (S3-S5 dermatomes)
- Preserved leg strength (lumbar segments above are intact)
Summary Table: Lesion Level vs. Effect
| Level | Motor Deficit | UMN/LMN | Other Features |
|---|---|---|---|
| Internal capsule | Contralateral hemiplegia (face + arm + leg) | UMN | Pure motor stroke; dysarthria |
| Midbrain | Contralateral hemiplegia | UMN | Ipsilateral CN III palsy (Weber's) |
| Pons | Contralateral hemiplegia | UMN | Ipsilateral CN VI/VII palsy |
| Medulla | Contralateral hemiplegia | UMN | No cranial nerve palsy (below nuclei) |
| Cervical (>C5) | Quadriplegia | UMN below; LMN at level | Respiratory failure if above C3 |
| Thoracic | Paraplegia | UMN | Sensory level; autonomic dysfunction |
| Lumbar | Paraplegia (or partial) | UMN or mixed | Varies by exact level |
| Conus/Cauda | Saddle anesthesia ± leg weakness | LMN | Bladder/bowel LMN type |
References:
- Gray's Anatomy for Students - Descending Tracts, pp. 1328-1335
- Guyton and Hall Textbook of Medical Physiology - Corticospinal (Pyramidal) Tract, p. 689
- Bradley and Daroff's Neurology in Clinical Practice - Pyramidal Tract; Anterior Horn and Pyramidal Tract Syndromes; Characteristic clinical features of lesions at different levels, pp. 467, 483-484
This is a shared conversation. Sign in to Orris to start your own chat.