Wilm's Tumor. (4 marks) (GMC)*** *Wilm's tumors. (2 marks) (NAMO)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed for a comprehensive, exam-ready answer. Here is the full write-up:
Wilms' Tumor (Nephroblastoma)
Definition
Wilms' tumor (nephroblastoma) is the most common primary malignant renal tumor of childhood and the fourth most common pediatric malignancy overall. It is an embryonal tumor that develops from remnants of immature metanephric kidney tissue.
Epidemiology
- Incidence: ~1 in 10,000 children
- Peak age: 2-5 years (95% of cases before age 10)
- 5-10% are bilateral (synchronous or metachronous)
- Bilateral tumors present ~10 months earlier - suggesting a germline mutation
- ~500 new cases/year in the US
- Overall cure rate: ~90% (one of the great successes of pediatric oncology, up from ~30% decades ago)
Pathogenesis and Genetics
Associated Syndromes (10% of cases - but key to understanding)
| Syndrome | Features | Gene/Locus | Wilms' Risk |
|---|---|---|---|
| WAGR syndrome | Wilms' tumor, Aniridia, Genital anomalies, mental Retardation | WT1 deletion + PAX6 deletion at 11p13 | ~33% |
| Denys-Drash syndrome (DDS) | Gonadal dysgenesis (male pseudohermaphroditism), diffuse mesangial sclerosis, early renal failure | Dominant-negative missense mutation in WT1 (zinc-finger region), 11p13 | ~90% |
| Beckwith-Wiedemann syndrome (BWS) | Visceromegaly, macroglossia, hemihypertrophy, hyperinsulinemic hypoglycemia | WT2 locus (11p15.5) - loss of imprinting of IGF2 gene; paternal allele overexpressed | Increased |
WAGR and DDS involve WT1 inactivation (two-hit mechanism for tumorigenesis). BWS involves IGF2 overexpression due to loss of imprinting - also predisposes to hepatoblastoma, adrenocortical tumors, rhabdomyosarcoma, and pancreatic tumors.
Sporadic (90%) Molecular Alterations
- ~10%: gain-of-function mutations in β-catenin
- 15-20%: mutations in genes encoding microRNA processing proteins, reducing levels of mature miRNAs involved in mesenchymal-to-epithelial transformation - leading to persistent blastemal rests
- TP53 mutations: associated with anaplastic histology and poor prognosis
Morphology
Gross Pathology
- Typically large, solitary, well-circumscribed mass replacing renal parenchyma
- 10% are bilateral or multicentric
- Cut surface: soft, homogeneous, tan-to-gray, with occasional hemorrhage, cystic degeneration, and necrosis
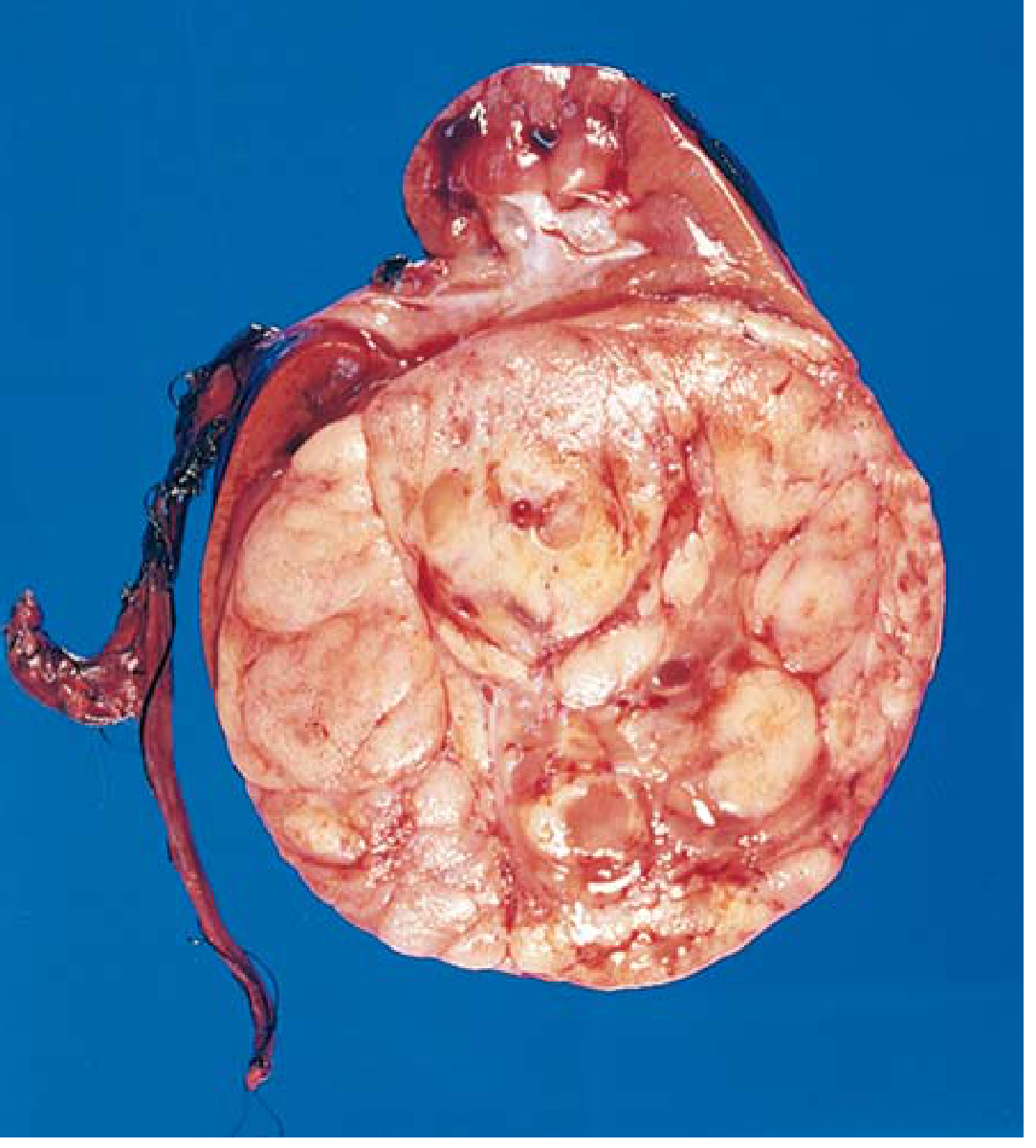
Gross specimen: Wilms' tumor occupying the lower pole of the kidney, showing the characteristic tan-to-gray color and well-circumscribed margins. - Robbins & Kumar Basic Pathology
Histology - Classic TRIPHASIC Pattern
The hallmark is recapitulation of different stages of nephrogenesis:
- Blastemal component - sheets of small, round, blue cells with scant cytoplasm (resembling embryonic metanephric blastema)
- Epithelial component - abortive tubules or primitive glomeruli
- Stromal component - fibroblastic or myxoid cells; skeletal muscle differentiation is not uncommon
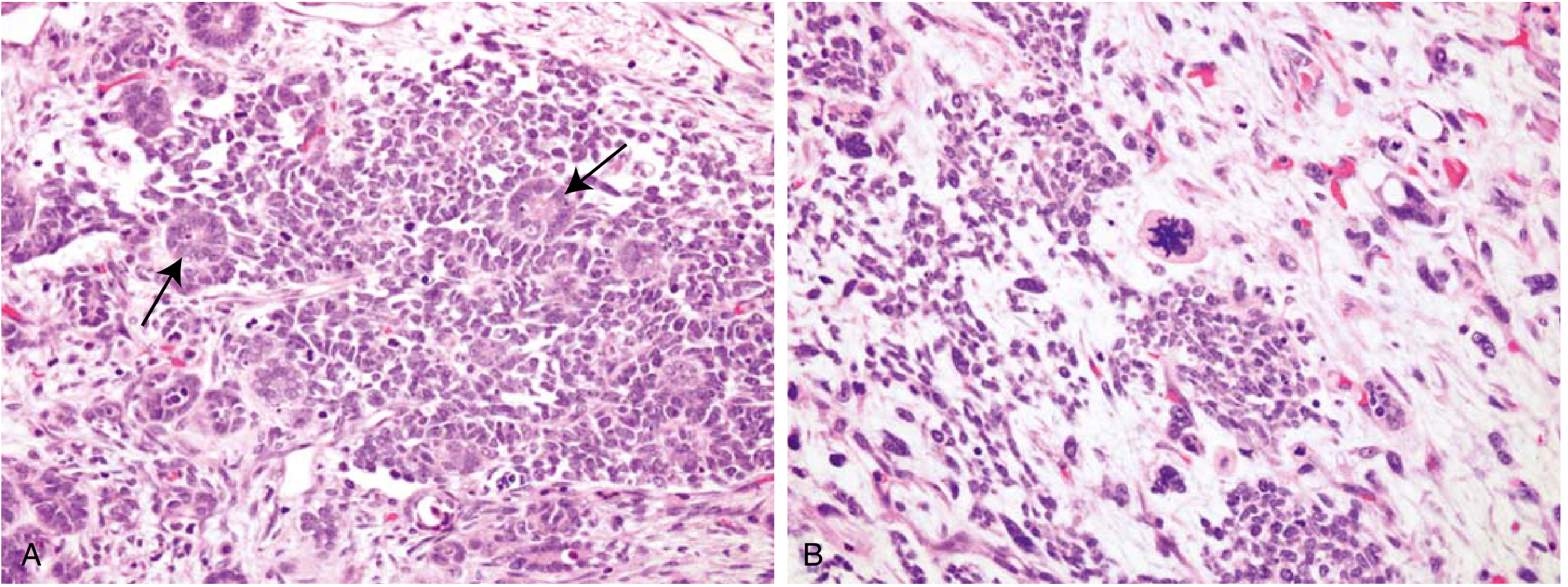
Fig A: Classic triphasic Wilms' tumor - tightly packed blue blastemal cells with interspersed primitive tubules (arrows). Fig B: Focal anaplasia - hyperchromatic pleomorphic nuclei and abnormal mitosis (center). - Robbins & Kumar Basic Pathology
Anaplasia (~5% of tumors)
- Cells with large, hyperchromatic, pleomorphic nuclei and abnormal mitoses
- Correlates with acquired TP53 mutations
- Associated with chemotherapy resistance and adverse prognosis
- Diffuse anaplasia = indicator of unfavorable histology
Nephrogenic Rests
- Precursor lesions of Wilms' tumor (putative)
- Present in renal parenchyma adjacent to the tumor
- Contain immature tubules, glomeruli, and cells resembling Wilms' tumor
- Their presence mandates close surveillance of the contralateral kidney
Clinical Features
- Asymptomatic abdominal/flank mass - most common presentation; often discovered by parent while bathing/dressing the child
- Hypertension
- Hematuria
- Abdominal pain, fever
- Intestinal obstruction (from tumor pressure)
- Occasionally discovered after blunt abdominal trauma
Staging (NWTSG)
| Stage | Description |
|---|---|
| Stage I | Tumor limited to kidney, completely excised |
| Stage II | Extends beyond kidney but completely excised (capsule penetration, renal sinus involvement) |
| Stage III | Residual non-hematogenous tumor in abdomen (positive nodes, peritoneal contamination, incomplete excision) |
| Stage IV | Hematogenous metastases (lung, liver, bone, brain) |
| Stage V | Bilateral renal involvement at diagnosis |
Investigations
- Abdominal + chest CT scan - characterizes the mass, detects metastases, evaluates the contralateral kidney, identifies nephrogenic rests
- Abdominal ultrasound - evaluates renal vein or inferior vena cava extension
- Urine catecholamines - to exclude neuroblastoma
Treatment
Surgery
- Radical nephroureterectomy with transperitoneal approach through a large transverse incision
- Early control of the renal pedicle (to prevent hematogenous spread)
- Sampling of regional lymph nodes mandatory
- Tumor rupture must be avoided (upstages to Stage III)
- Bilateral disease: biopsy both lesions → preoperative chemo → nephron-sparing surgery
Chemotherapy
- Actinomycin D + Vincristine (favourable histology, early stages)
- Adding Doxorubicin for higher stages
- Radiation for Stage III/IV or unfavorable histology
Two Major Study Group Approaches
- NWTSG (North America): Surgery first, then chemo ± radiation
- SIOP (Europe): Preoperative chemotherapy to shrink tumor first, then surgery
- Both groups agree on preoperative chemo for: bilateral disease, IVC involvement above hepatic veins, or solitary kidney involvement
Prognosis
- Stage I/II with favorable histology: ~97% 4-year survival
- Overall survival: ~90%
- Unfavorable histology (diffuse anaplasia, blastemal predominance): significantly worse
- Diffuse anaplasia is the most important adverse prognostic factor
Key Summary (for 2-mark questions)
- Definition: Most common primary renal tumor of childhood; embryonal tumor (nephroblastoma); peak age 2-5 years
- Associated syndromes: WAGR (WT1 deletion, 11p13), Denys-Drash (WT1 mutation, 90% risk), Beckwith-Wiedemann (IGF2 imprinting, 11p15)
- Histology: Classic triphasic pattern - blastemal + epithelial + stromal; anaplasia = poor prognosis
- Presentation: Asymptomatic flank mass in a young child
- Treatment: Nephrectomy + chemotherapy ± radiotherapy; ~90% cure rate
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Schwartz's Principles of Surgery 11e; Campbell-Walsh-Wein Urology
Wilm's Tumor. (4 marks) (GMC)*** *Wilm's tumors. (2 marks) (NAMO
I already covered this topic in full detail in the previous response. Here is a clean, exam-focused version formatted for both the 4-mark (GMC) and 2-mark (NAMO) weightings:
Wilms' Tumor (Nephroblastoma)
For 2-mark answer (NAMO)
Definition: Wilms' tumor (nephroblastoma) is the most common primary malignant renal tumor of childhood, arising from remnants of immature metanephric kidney (embryonal tumor). Peak age: 2-5 years. Presents as a large, asymptomatic abdominal mass in a young child. Histologically shows a classic triphasic pattern - blastemal + epithelial + stromal cells. Treatment: nephrectomy + chemotherapy. Overall cure rate ~90%.
For 4-mark answer (GMC)
Definition & Epidemiology
- Most common primary renal tumor of childhood; 4th most common pediatric malignancy
- Incidence: ~1 in 10,000 children; peak age 2-5 years
- 5-10% bilateral (synchronous or metachronous)
- Cure rate: ~90% (up from 30% decades ago)
Associated Syndromes & Genetics
| Syndrome | Features | Gene | Risk |
|---|---|---|---|
| WAGR | Wilms', Aniridia, Genital anomalies, mental Retardation | WT1 deletion + PAX6, 11p13 | ~33% |
| Denys-Drash (DDS) | Gonadal dysgenesis, diffuse mesangial sclerosis, early renal failure | WT1 dominant-negative mutation, 11p13 | ~90% |
| Beckwith-Wiedemann | Visceromegaly, macroglossia, hemihypertrophy | Loss of imprinting of IGF2, 11p15.5 | Increased |
- 90% of cases are sporadic - β-catenin gain-of-function (~10%), miRNA processing mutations (15-20%)
- TP53 mutations → anaplastic histology → worst prognosis
Morphology
Gross:
- Large, solitary, well-circumscribed mass
- Soft, tan-to-gray on cut section; with hemorrhage and necrosis
Microscopy - Classic Triphasic Pattern:
- Blastemal - sheets of small round blue cells (resembles embryonic metanephric blastema)
- Epithelial - abortive tubules or primitive glomeruli
- Stromal - fibroblastic/myxoid cells; skeletal muscle differentiation may occur
Anaplasia (~5%):
- Large hyperchromatic pleomorphic nuclei + abnormal mitoses
- Linked to TP53 mutations; indicates chemotherapy resistance and poor prognosis
Nephrogenic rests:
- Putative precursor lesions of Wilms' tumor
- Presence warrants surveillance of the contralateral kidney
Clinical Features
- Asymptomatic flank/abdominal mass - most common (often found by parent while bathing child)
- Hypertension, hematuria, abdominal pain, fever
- Occasionally after blunt abdominal trauma
Staging (NWTSG)
| Stage | Description |
|---|---|
| I | Confined to kidney, completely excised |
| II | Beyond kidney but completely excised |
| III | Residual abdominal tumor (nodes, spillage, incomplete excision) |
| IV | Hematogenous metastases (lung, liver) |
| V | Bilateral renal involvement |
Treatment
| Component | Details |
|---|---|
| Surgery | Radical nephroureterectomy; transperitoneal approach; early renal pedicle control; lymph node sampling |
| Chemotherapy | Actinomycin D + Vincristine (± Doxorubicin for higher stages) |
| Radiotherapy | Stage III/IV or unfavorable histology |
| Bilateral disease | Biopsy → chemo → nephron-sparing surgery |
- NWTSG approach: surgery first, then chemo
- SIOP (European) approach: preoperative chemo to shrink tumor, then surgery
- Both agree on preoperative chemo for bilateral disease, IVC involvement above hepatic veins, or solitary kidney
Prognosis
- Stage I/II, favorable histology: ~97% 4-year survival
- Overall: ~90% survival
- Diffuse anaplasia = most important adverse prognostic indicator
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Schwartz's Principles of Surgery 11e; Campbell-Walsh-Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.