1. resuscitation in pregnant women , surviving sepsis guidlines 2. LFT and their significane, child pugh score 3. usg guided adductor canal block, renal replacement therapy 4. types of labour analgesia, pain pathway in labour pain 5. anaesthesia challenges and mgt of posterior fossa tumour 6. airway management of maxillofacial trauma plus manual inline stabilization 7. anaesthesia mgt of 2 year old paediatric who has foreign body insertion taken for emergency 8. biochemical changes of stored blood, indication and complication of blood transfusion 9. link 25, electrical safety of OT 10. post op analgesia for paediatric in lower abdominal surgery and thoracotomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
surviving sepsis campaign 2024 guidelines resuscitation pregnant women
Here is a comprehensive structured review of all 10 topics:
Anaesthesia Comprehensive Review
1. Resuscitation in Pregnant Women + Surviving Sepsis Guidelines
Physiological Adaptations Relevant to Resuscitation
- Aortocaval compression: From 20 weeks gestation, the gravid uterus compresses the IVC → reduced venous return → left lateral tilt 15–30° (wedge under right hip) is mandatory during CPR/resuscitation
- Airway: Oedematous, Mallampati increases, higher risk of aspiration (reduced LOS tone, delayed gastric emptying) → early RSI with cricoid pressure
- Respiratory: Increased O₂ consumption (20%), reduced FRC (20%) → desaturates faster; PaCO₂ normally 30 mmHg (respiratory alkalosis)
- Cardiovascular: CO increases 40–50%, HR +15–20 bpm, SVR falls; BP normally lower
- Blood: Dilutional anaemia (Hb ~11 g/dL), physiological hypercoagulability
Cardiac Arrest in Pregnancy — 4H4T + Perimortem Caesarean (PMCS)
| Step | Action |
|---|---|
| Position | Left lateral tilt or manual uterine displacement |
| Airway | Early intubation (aspiration risk), waveform capnography |
| Compressions | Standard 30:2, hard & fast, full chest recoil |
| PMCS | If no ROSC within 4 minutes → deliver baby by 5 minutes (improves maternal resuscitation) |
| Defibrillation | Same energy as non-pregnant; remove fetal monitors first |
Causes unique to pregnancy: Eclampsia/PE, peripartum cardiomyopathy, amniotic fluid embolism, Mg toxicity, aortocaval compression, haemorrhage
Surviving Sepsis Campaign Guidelines (SSC 2021 — "Hour-1 Bundle")
Definitions: Sepsis = life-threatening organ dysfunction caused by dysregulated host response to infection. Septic shock = vasopressor needed to maintain MAP ≥65 mmHg + lactate >2 mmol/L despite adequate resuscitation.
Hour-1 Bundle (initiate within 1 hour of recognition)
- Measure lactate (remeasure if >2 mmol/L)
- Blood cultures ×2 (before antibiotics; don't delay antibiotics >45 min)
- Broad-spectrum antibiotics within 1 hour
- 30 mL/kg crystalloid IV if hypotensive or lactate ≥4 mmol/L
- Vasopressors if MAP <65 mmHg during/after fluid — noradrenaline first-line
Additional SSC Targets
- MAP ≥65 mmHg
- ScvO₂ ≥70%, CVP 8–12 mmHg (or 12–15 if mechanically ventilated)
- Urine output ≥0.5 mL/kg/hr
- Glycaemic control: maintain blood glucose <10 mmol/L (180 mg/dL)
- Corticosteroids: Hydrocortisone 200 mg/day IV if vasopressor-refractory shock
- Lung-protective ventilation: Tidal volume 6 mL/kg IBW, Pplat <30 cmH₂O, PEEP as needed
- Prone ventilation ≥16 hours/day if PaO₂/FiO₂ <150
Sepsis in Pregnancy — Special Considerations
- Most common organisms: Group A Strep, E. coli, GBS
- Avoid aminoglycosides if possible (nephrotoxicity)
- Hydrocortisone safe in pregnancy
- Delivery may be required to treat source (chorioamnionitis)
- Normal WBC in pregnancy is 9,000–15,000 → sepsis harder to detect biochemically
2. Liver Function Tests (LFTs) and Significance + Child-Pugh Score
LFTs and Clinical Significance
| Test | Normal | Significance |
|---|---|---|
| Bilirubin (total) | <17 µmol/L | Jaundice if >34; pre-hepatic (haemolysis), hepatic, post-hepatic (obstruction) |
| Bilirubin (direct/conjugated) | <7 µmol/L | Elevated in hepatocellular disease or cholestasis |
| ALT (SGPT) | 7–56 U/L | Hepatocyte damage (liver-specific); hallmark of hepatitis |
| AST (SGOT) | 10–40 U/L | Less specific — liver, heart, muscle; AST:ALT >2:1 → alcoholic liver disease |
| ALP | 30–120 U/L | Cholestasis, bone disease; isolated rise → biliary/infiltrative |
| GGT | <55 U/L | Alcohol abuse, biliary, enzyme inducer; sensitive marker |
| Albumin | 35–50 g/L | Synthetic function; half-life 21 days — chronic disease marker |
| PT / INR | INR <1.2 | Clotting factor synthesis (Factors I, II, V, VII, X); acutely sensitive to liver failure |
| Total Protein | 60–80 g/L | Includes albumin + globulins |
Patterns:
- Hepatocellular: ↑↑ ALT/AST, ↑ bilirubin, ↓ albumin, ↑ PT
- Cholestatic: ↑↑ ALP/GGT, ↑ bilirubin, normal/mild ↑ transaminases
- Synthetic failure: ↓ Albumin, ↑ INR/PT, ↑ bilirubin → suggests cirrhosis/acute liver failure
Anaesthetic Implications of LFT Abnormalities
- Coagulopathy: Fresh frozen plasma, vitamin K, platelet transfusion
- Hypoalbuminaemia: ↑ free fraction of protein-bound drugs (e.g. thiopental, benzodiazepines)
- Ascites: Risk of regurgitation, diaphragm splinting, ↓ FRC
- Hepatic encephalopathy: Avoid morphine, benzodiazepines
- Avoid: Halothane (hepatotoxic), NSAIDS (renal + GI effects)
- Drug metabolism: Reduced CYP450 activity → prolonged drug effects
Child-Pugh Score
Used to assess severity of liver disease and predict operative mortality.
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Bilirubin (µmol/L) | <34 | 34–51 | >51 |
| Albumin (g/L) | >35 | 28–35 | <28 |
| PT Prolongation (sec) | <4 | 4–6 | >6 |
| Ascites | None | Mild/controlled | Severe/refractory |
| Encephalopathy | None | Grade 1–2 | Grade 3–4 |
| Class | Score | 1-year survival | Operative mortality |
|---|---|---|---|
| A | 5–6 | 100% | 2–10% |
| B | 7–9 | 80% | ~30% |
| C | 10–15 | 45% | ~75–82% |
Child-Pugh C patients are high surgical risk; elective surgery should be deferred. MELD score (Model for End-stage Liver Disease) is now preferred for transplant allocation.
3. USG-Guided Adductor Canal Block + Renal Replacement Therapy
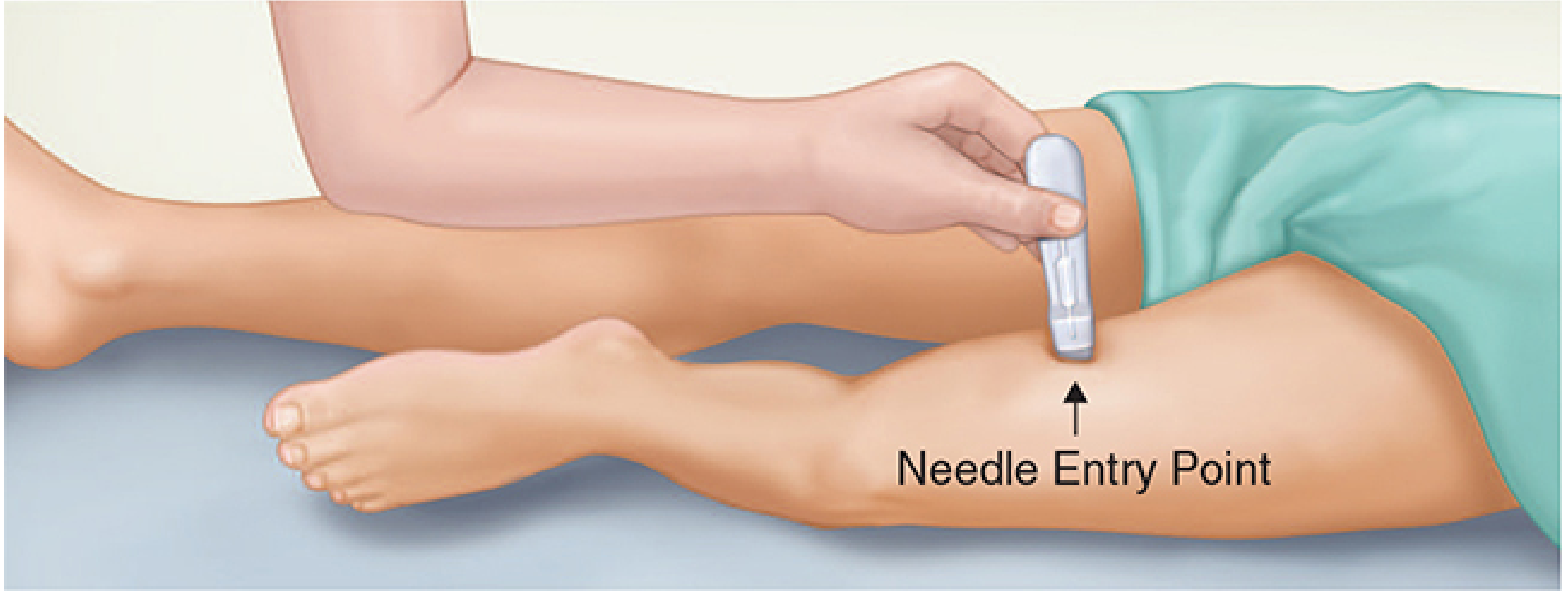
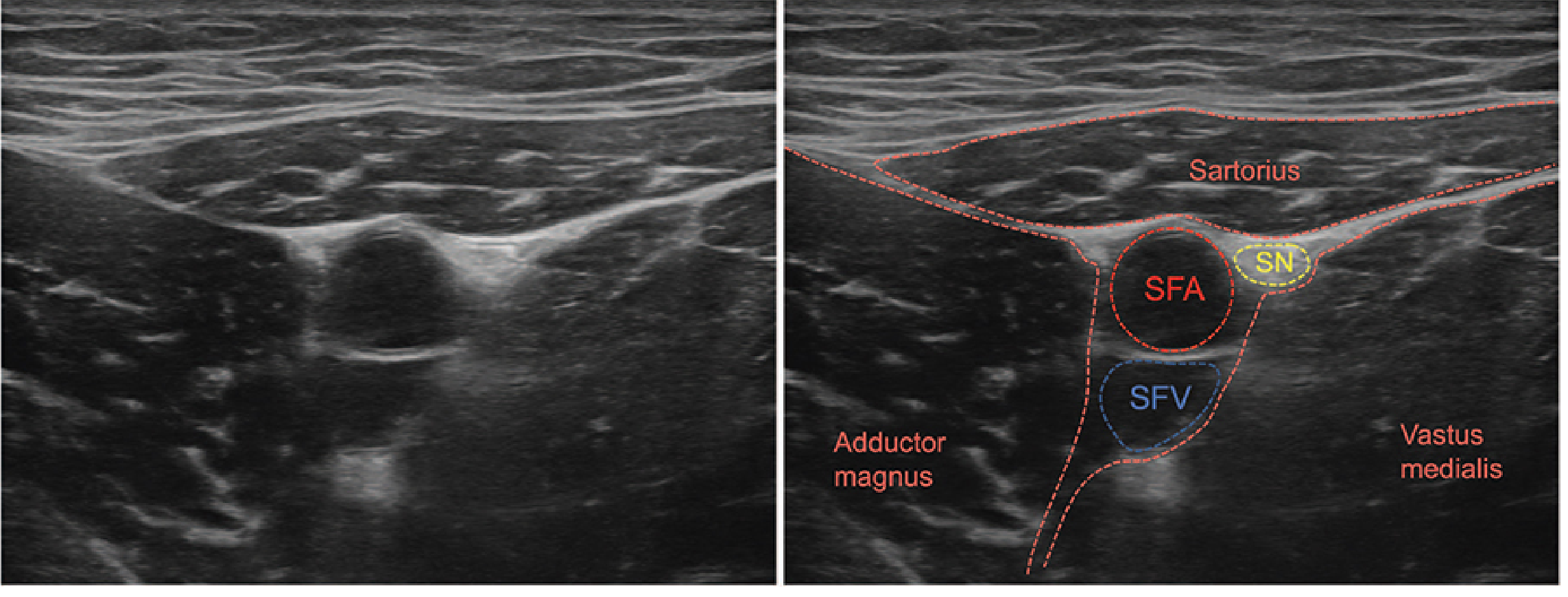
USG-Guided Adductor Canal Block (ACB)
(Source: Morgan & Mikhail's Clinical Anesthesiology, 7e)
Anatomy: The adductor canal (Hunter's canal) is bounded by:
- Sartorius muscle — medially
- Vastus medialis — anteriorly
- Adductor magnus & longus — posteriorly
Contents: Saphenous nerve, posterior branch of obturator nerve, nerve to vastus medialis, superficial femoral artery & vein
Indications: Knee surgery (TKA, ACL repair, meniscectomy), medial leg/ankle surgery; preferred over femoral nerve block as it preserves quadriceps strength, allowing earlier ambulation.
Technique (USG-guided):
- Position: Supine, leg externally rotated, knee slightly flexed
- Probe: High-frequency linear probe, transverse orientation, mid-thigh (halfway between ASIS and superior patellar pole)
- Identify: Femoral artery (pulsatile), vein (compressible), sartorius muscle superficially; saphenous nerve lies anterior to the artery (hyperechoic structure)
- Needle: In-plane technique, insert 2–3 cm lateral to probe, advance medially into the triangular space deep to sartorius, anterior to artery
- Confirm: Negative aspiration, spread of LA around nerve/artery
- Volume: 15–20 mL local anaesthetic (0.25–0.5% bupivacaine or 0.2% ropivacaine)
Advantages over femoral nerve block: No quadriceps weakness → earlier mobilisation; equivalent analgesia for knee surgery.
Continuous ACB: Catheter placed; useful post-TKA for 24–48 hours.
Renal Replacement Therapy (RRT)
Indications (mnemonic AEIOU):
- A — Acidosis (metabolic, pH <7.1, refractory)
- E — Electrolyte disturbance (hyperkalaemia >6.5, refractory)
- I — Intoxication (dialysable toxins: lithium, salicylates, methanol, ethylene glycol, theophylline)
- O — Overload (fluid overload refractory to diuretics)
- U — Uraemia (uraemic pericarditis, encephalopathy, Urea >30 mmol/L)
Modalities:
| Mode | Mechanism | Rate | Use |
|---|---|---|---|
| IHD (Intermittent Haemodialysis) | Diffusion | Fast | Stable CKD/AKI, toxin removal |
| CVVH (Continuous Veno-venous Haemofiltration) | Convection | Slow | Haemodynamically unstable ICU |
| CVVHD (+ Dialysis) | Diffusion + convection | Slow | ICU with metabolic derangement |
| CAVH | Arterio-venous (no pump) | Slow | Rarely used |
| PD (Peritoneal Dialysis) | Diffusion across peritoneum | Slow | Paediatric, home dialysis |
| SLED (Sustained Low Efficiency Dialysis) | Hybrid | Medium | Haemodynamic instability |
Continuous RRT (CRRT) is preferred in ICU because:
- Better haemodynamic tolerance
- Gradual fluid removal avoids cerebral oedema
- Allows large volumes of IV drugs/nutrition
Anticoagulation for RRT: Unfractioned heparin (systemic), regional citrate anticoagulation (preferred — less bleeding risk), or no anticoagulation (high bleeding risk patients).
4. Types of Labour Analgesia + Pain Pathway in Labour Pain
Pain Pathway in Labour
First Stage of Labour (latent + active):
- Pain from uterine contractions and cervical dilation
- Transmitted via visceral afferents (C-fibres) → enter cord at T10–L1
- Travel with sympathetic fibres through uterine and cervical plexuses → inferior hypogastric plexus → lumbar sympathetic chain → thoracic sympathetic chain → spinal cord T10–L1
Second Stage of Labour:
- Pain from perineal distension and vaginal/pelvic floor stretching
- Transmitted via somatic afferents (pudendal nerve, S2–4)
- Combined visceral (T10–L1) + somatic (S2–4) pain
Pain character: First stage — dull, crampy, referred to lower abdomen, back, thighs; Second stage — sharp, perineal, burning
Types of Labour Analgesia
1. Neuraxial (Regional) — Gold Standard
a) Epidural Analgesia
- Most commonly used; flexible
- Space: L2-3 or L3-4; loss of resistance technique
- Drug: Low-concentration bupivacaine (0.0625–0.1%) + fentanyl (2 µg/mL) or sufentanil
- Techniques: Continuous infusion (CEI), PCEA (patient-controlled epidural), PIEB (programmed intermittent epidural bolus — superior)
- Covers T10–L1 (1st stage) and S2–4 (2nd stage)
- Side effects: Hypotension (treat with IV fluids, vasopressors), motor block, PDPH (dural puncture headache), instrumental delivery rate
b) Spinal Analgesia
- Low-dose intrathecal: Bupivacaine 2.5 mg + fentanyl 25 µg
- Rapid onset but limited duration (1.5–2 hours); not preferred alone for labour
c) Combined Spinal-Epidural (CSE)
- Best of both: rapid onset of spinal + flexibility of epidural
- Needle-through-needle technique
- Intrathecal dose: bupivacaine 2.5 mg + fentanyl 25 µg
- Ideal for advanced labour or when rapid analgesia needed
d) Dural Puncture Epidural (DPE)
- Epidural needle + deliberate dural puncture (without injection); enhances epidural spread
- Lower risk of PDPH than CSE
2. Systemic Opioid Analgesia
| Drug | Route | Notes |
|---|---|---|
| Pethidine (Meperidine) | IM/IV | Most used; CNS depression in neonate (norpethidine); avoid if delivery <4 hours |
| Morphine | IM | Less titratable; neonatal respiratory depression |
| Fentanyl | IV/PCA | Short-acting, better titratable; neonatal depression less |
| Remifentanil PCA | IV PCA | Growing evidence; watch maternal respiratory depression; 1:1 nurse monitoring required |
Remifentanil PCA: Bolus 0.25–0.5 µg/kg; lockout 2 min; comparable to epidural in some studies.
3. Inhaled Analgesia
- Entonox (50% N₂O + 50% O₂): Self-administered; onset in 30–45 seconds; partial, not complete analgesia; nausea
- Methoxyflurane (Penthrox): Inhaler device; effective, rapid onset
4. Regional Nerve Blocks
- Pudendal nerve block: 2nd stage/instrumental delivery; 10 mL 1% lignocaine at ischial spine bilaterally; covers S2–4 (perineum only)
- Paracervical block: Covers cervical afferents T10–L1; risk of fetal bradycardia (vasoconstriction of uterine artery); largely abandoned
- Lumbar sympathetic block: Covers 1st stage (T10–L1) via bilateral L2–3 block
5. Non-Pharmacological
- Hydrotherapy, TENS, massage, acupuncture, hypnobirthing — limited but real analgesic effect
5. Anaesthesia Challenges & Management of Posterior Fossa Tumour
Challenges
1. Positioning
- Sitting position (most common for posterior fossa): Risk of Venous Air Embolism (VAE) — most dangerous complication; also risk of paradoxical air embolism if PFO present (check with bubble echo preop)
- Other positions: Prone (Concorde), lateral, park-bench
- Sitting position: Also risks pneumocephalus, haemodynamic instability, quadriplegia from neck flexion (≥2 finger-breadths between chin and chest)
2. Raised Intracranial Pressure (ICP)
- Posterior fossa tumours → hydrocephalus (4th ventricle obstruction)
- Manage: Head up 30°, avoid hypercapnia (PaCO₂ 34–38 mmHg), avoid hypoxia, judicious fluids (isotonic solutions, avoid glucose), mannitol 0.5–1 g/kg, dexamethasone
3. Venous Air Embolism (VAE)
- Risk highest in sitting position (surgical site above heart level)
- Detection (in order of sensitivity): TOE > precordial Doppler > capnography (ETCO₂ drop) > pulmonary artery catheter > CVP > clinical signs
- Management of VAE: Flood field with saline, N₂O off immediately, left lateral Trendelenburg (Durant manoeuvre), aspiration via CVP catheter, vasopressors, CPR if cardiac arrest
4. Cranial Nerve & Brainstem Proximity
- Risk of intraoperative injury to V, VI, VII, IX, X, XI, XII
- Neuromonitoring: SSEP (somatosensory evoked potentials), BAEP (brainstem auditory), MEP (motor), facial nerve EMG — requires TIVA (avoid volatile agents which suppress evoked potentials)
5. Pneumocephalus
- Air enters cranial vault during surgery; worsens with N₂O (enlarges air pockets) → avoid N₂O in sitting craniotomy; use TIVA
Anaesthesia Management
Preoperative:
- Review MRI, assess ICP signs (headache, vomiting, papilloedema)
- Neurological baseline
- Steroids (dexamethasone 4–8 mg q6h) pre-operatively
- Consent for sitting position: Doppler + CVC placement
Induction:
- TIVA preferred (propofol + remifentanil infusion) — maintains neurological monitoring
- Avoid ketamine (increases ICP)
- Smooth induction: Prevent coughing/straining → IV lidocaine 1.5 mg/kg or remifentanil bolus before laryngoscopy
- Hyperventilate mildly (PaCO₂ 34–36 mmHg)
Maintenance:
- TIVA (propofol + remifentanil) if neuromonitoring in use
- Or low-dose volatile (<0.5 MAC) + opioid if monitoring not required
- Glucose-free isotonic fluids; avoid hypo-osmolar solutions
- Maintain MAP 60–90 mmHg; cerebral perfusion pressure >60 mmHg
Monitoring:
- Arterial line (BP beat-to-beat), CVC (VAE aspiration catheter at cavoatrial junction), ETCO₂, precordial Doppler, BIS/depth of anaesthesia, neuromonitoring probes, temperature
Sitting Position Precautions:
- Avoid hypovolaemia before sitting (leg elevation, sequential compression devices)
- Precordial Doppler or TOE in place before positioning
- Adequate neck flexion check (2-finger breadth chin-chest distance)
Postoperative:
- Awake extubation preferred (assess neurological status)
- ICU/HDU
- Dexamethasone continued
- Monitor for: haematoma, pneumocephalus, cranial nerve deficits, hydrocephalus, cerebellar oedema
- Tension pneumocephalus → causes "Mount Fuji sign" on CT → neurosurgical emergency
6. Airway Management of Maxillofacial Trauma + Manual Inline Stabilisation (MILS)
Challenges in Maxillofacial Trauma Airway
- Distorted anatomy: Fractures (Le Fort I/II/III, mandibular, zygomatic), oedema, haematoma → difficult laryngoscopy
- Blood in airway: Clots, active haemorrhage obscure the view
- Trismus: Limited mouth opening
- Aspiration risk: Blood, secretions, gastric contents (full stomach)
- Associated C-spine injury: ~2–5% of maxillofacial trauma; assume C-spine injury until cleared
- Unstable fractures: Mid-face fractures may allow inadvertent passage of instruments into cranial vault (cribriform plate breach)
Approach
Assessment (ABCDE first):
- Check SpO₂, airway patency, respiratory rate
- GCS, C-spine status, facial anatomy
- Airway predictors: Blood, trismus, facial swelling, ability to open mouth, Mallampati (if possible), neck mobility
Airway Management Options (stepwise):
| Option | Indication |
|---|---|
| RSI + direct laryngoscopy | Adequate mouth opening, manageable haemorrhage |
| Video laryngoscopy (VL) | First-line in anticipated difficult airway; improves C-spine alignment view |
| Awake Fibreoptic Intubation (AFOI) | Anticipated very difficult airway, time permits, cooperative patient |
| Nasotracheal intubation | Trismus; CONTRAINDICATED if cribriform plate fracture suspected (Le Fort II/III, basal skull fracture signs) |
| Surgical airway | Cannot intubate, cannot oxygenate (CICO) → emergency cricothyroidotomy |
Cricothyroidotomy (CICO):
- Scalpel–bougie technique (preferred over needle): vertical skin incision → horizontal stab into CTM → bougie insertion → tube railroaded
- Cannula cricothyroidotomy (4 mm kink-resistant catheter) as bridge
Manual Inline Stabilisation (MILS)
Principle: Maintains cervical spine in neutral position during laryngoscopy when C-spine collar is removed.
Why collar removed?: Rigid collar reduces mouth opening and worsens laryngoscopy → must remove it but must still protect C-spine.
Technique:
- A second operator stands to the side facing the patient's head
- Hands placed on mastoid processes (not mandible) and occiput — bilateral grip
- Applies gentle, firm counter-force against head/neck movement during laryngoscopy
- Does NOT improve the laryngoscopic view — may actually worsen glottic view (by preventing atlanto-occipital extension)
- Neutral position maintained, not immobilisation — allows mouth to open
Key Point: MILS does not prevent all spinal cord injury — it reduces excessive movement. If laryngoscopy view is poor, video laryngoscopy (hyperangulated blade) or flexible scope should be used.
RSI in C-spine injury:
- Remove collar, apply MILS
- Preoxygenate (high-flow O₂ 3 min or 8 vital capacity breaths)
- Induction: Ketamine 1.5 mg/kg or thiopentone 3–5 mg/kg + suxamethonium 1.5 mg/kg
- Sellick's manoeuvre (cricoid pressure) if aspiration risk
- Video laryngoscopy preferred (GlideScope, C-MAC)
- Have surgical airway immediately available
7. Anaesthesia Management of a 2-Year-Old with Foreign Body (Emergency)
Preoperative Assessment
History:
- Nature, size, shape of foreign body (FB); when ingested
- Airway vs oesophageal FB (stridor, wheeze, drooling vs dysphagia)
- Last oral intake (full stomach — emergency)
- Symptoms: Respiratory distress, cyanosis, drooling, complete vs partial obstruction
Examination:
- SpO₂ on room air, RR, work of breathing, air entry
- Stridor (inspiratory = supraglottic; expiratory = subglottic/tracheal; biphasic = fixed obstruction)
- Signs of complete obstruction (silent chest, cyanosis) → immediate intervention
Investigations:
- CXR (inspiratory/expiratory): Air trapping, hyperinflation, mediastinal shift (ball-valve FB in bronchus)
- Lateral neck X-ray (radio-opaque FB)
- CT scan if needed
Anaesthetic Challenges in a 2-Year-Old
- Small airway → easy obstruction
- High O₂ consumption → rapid desaturation
- Small functional residual capacity
- Uncooperative
- Full stomach
- Risk of pushing FB further or dislodging during induction
Anaesthetic Management
1. Preparation:
- Senior anaesthetist, ENT surgeon scrubbed and ready, paediatric resuscitation equipment
- Airway trolley: Range of ETT (uncuffed 4.5 for 2-year-old; ID = age/4 + 4 = 4.5), bronchoscopes (rigid + flexible), laryngoscopes (straight blade Miller 1–2)
- Drugs: Atropine (0.02 mg/kg IV, minimum 0.1 mg — prevent bradycardia), induction agents
- IV access established (EMLA cream)
2. Induction:
- Gaseous induction with 100% O₂ + sevoflurane if IV access not established (maintains spontaneous ventilation, less likely to dislodge FB)
- OR IV induction if IV access in place and child stable:
- Propofol 2–3 mg/kg + dexamethasone 0.15 mg/kg (airway oedema)
- Avoid suxamethonium if partial obstruction (loss of tone → complete obstruction risk — controversial; use clinical judgement)
- Atropine before induction (bradycardia with sevo/rigid scope)
3. Airway Technique:
- Rigid bronchoscopy (ENT/paediatric surgeons): For subglottic/tracheal/bronchial FB — maintain spontaneous or controlled ventilation through side port of bronchoscope
- Direct laryngoscopy for supraglottic/laryngeal FB
- Topical lignocaine on larynx (1 mg/kg max) to reduce laryngospasm
4. Ventilation Strategy:
- Spontaneous ventilation preferred for airway FB (reduces risk of complete obstruction with positive pressure)
- TPPR (Total intravenous + preserve respiration): Propofol + dexmedetomidine/remifentanil infusion
- If IPPV needed: Low tidal volume, watch for air trapping
5. Emergency Considerations:
- If complete obstruction: Back blows/chest thrusts (Paediatric BLS), emergency laryngoscopy
- CICO: Needle cricothyroidotomy in child <12 years, jet ventilation
- Post-extraction: Check for second FB, mucosal oedema (nebulised adrenaline 0.5 mL of 1:1000)
Postoperative:
- Extubate awake, upright
- Observe for laryngospasm, bronchospasm, oedema
- Dexamethasone 0.15–0.3 mg/kg reduces post-extubation stridor
- Nebulised adrenaline if stridor present
8. Biochemical Changes in Stored Blood + Indications & Complications of Blood Transfusion
Biochemical Changes in Stored Blood
Blood is stored in CPDA-1 (citrate-phosphate-dextrose-adenine) at 2–6°C for up to 35 days (SAGM up to 42 days).
| Parameter | Change with Storage | Clinical Significance |
|---|---|---|
| pH | ↓ (7.4 → ~6.7) | Metabolic acidosis (citric acid, lactic acid accumulation) |
| pCO₂ | ↑ | |
| pO₂ | ↓ | |
| Potassium (K⁺) | ↑ (rises to 30–40 mmol/L) | Hyperkalaemia — risk in rapid/massive transfusion, neonates, renal failure |
| Sodium (Na⁺) | Slightly ↓ | |
| Calcium (Ca²⁺) | ↓ (citrate binds Ca²⁺) | Hypocalcaemia → myocardial depression, coagulopathy |
| 2,3-DPG | ↓↓ (significant after 1–2 weeks) | Leftward shift of O₂ dissociation curve → ↓ O₂ delivery to tissues |
| ATP | ↓ | ↓ RBC deformability, ↑ haemolysis |
| Haemoglobin | Unchanged but function impaired | |
| Clotting factors | ↓ significantly | After 5–7 days; FFP needed with massive transfusion |
| Platelets | Non-functional by day 1 | Platelets not present in packed RBCs (removed) |
| Ammonia | ↑ | Hepatic encephalopathy risk |
| Microaggregates | Form over time | Microemboli to lungs (filter with 40 µm filter for large volumes) |
| Temperature | Cold (2–6°C) | Hypothermia → worsens coagulopathy; use blood warmer |
Storage lesion: Overall deterioration of RBC function (↑ haemolysis, ↓ deformability, ↑ adhesion, ↑ proinflammatory mediators, ↓ NO bioavailability).
Indications for Blood Transfusion
Packed Red Blood Cells (pRBCs):
- Hb <7 g/dL (stable non-cardiac patients) — Restrictive trigger (TRICC criteria)
- Hb <8 g/dL in cardiac surgery, ACS, orthopaedic surgery
- Hb <10 g/dL in symptomatic patients (angina, dyspnoea, tachycardia)
- Acute haemorrhage with haemodynamic instability (Class III/IV shock)
- Symptomatic anaemia regardless of Hb level
FFP (Fresh Frozen Plasma):
- PT/APTT >1.5× normal with active bleeding
- Massive transfusion (1:1:1 ratio with RBCs:FFP:Platelets in military/trauma protocols)
- Reversal of warfarin in emergency
- DIC
- TTP (plasma exchange)
Platelets:
- Plt <10 × 10⁹/L (prophylactic)
- Plt <50 × 10⁹/L with active bleeding or surgery
- Plt <100 × 10⁹/L for neurosurgery/ophthalmic surgery
Cryoprecipitate:
- Fibrinogen <1.5 g/L with bleeding
- Haemophilia A, vWD, hypofibrinogenaemia, DIC
Complications of Blood Transfusion
IMMEDIATE (<24 hours):
| Complication | Mechanism | Features |
|---|---|---|
| AHTR (Acute Haemolytic Transfusion Reaction) | ABO incompatibility; IgM antibody-mediated | Fever, rigors, flank pain, haemoglobinuria, DIC, renal failure; STOP transfusion immediately |
| FNHTR (Febrile Non-Haemolytic) | Recipient antibodies to donor WBCs/HLA | Fever, chills; most common; treat with paracetamol |
| Allergic/Anaphylactic | Antibodies to donor plasma proteins (IgA deficiency) | Urticaria → anaphylaxis; adrenaline |
| TRALI (Transfusion-Related Acute Lung Injury) | Donor anti-HLA antibodies → neutrophil activation in lungs | Acute hypoxia within 6 hours; non-cardiogenic pulmonary oedema; leading cause of transfusion death |
| TACO (Transfusion-Associated Circulatory Overload) | Volume overload | Hypertension, pulmonary oedema; diuretics |
| Hypothermia | Cold blood | Arrhythmias, coagulopathy; use blood warmer |
| Hyperkalaemia | K⁺ leakage from stored RBCs | Cardiac arrest especially in neonates/renal failure |
| Hypocalcaemia | Citrate chelates Ca²⁺ | Tetany, myocardial depression; Ca gluconate IV |
| DIC | Haemolytic reaction or massive transfusion |
DELAYED (>24 hours):
- DHTR (Delayed Haemolytic): Non-ABO antibodies; mild, self-limited
- TRALI (can be late)
- Post-transfusion purpura: Platelet antibody, day 5–10
- Graft-vs-Host Disease (TA-GvHD): Immunocompromised patients; fatal; prevent with irradiated blood
- Infection: HIV, Hep B, Hep C, CMV, variant CJD, bacterial contamination (platelets at room temp → highest bacterial risk)
- Iron overload: Repeated transfusions → haemosiderosis (chelation therapy)
- Immunosuppression: Transfusion-related immunomodulation (TRIM)
9. Link 25 + Electrical Safety in the Operating Theatre
LINK 25 (Isolated Power Supply System)
Link 25 refers to the line isolation monitor (LIM) — part of the isolated (ungrounded) power supply system mandated in operating theatres in the UK (HTM 2007/HTM 06-01) and elsewhere.
Why isolated power in OT?
- Standard grounded electrical systems: Any single fault can complete a circuit via earth → person touching live equipment is electrocuted (macroshock)
- Isolated power system: The power supply transformer secondary winding is not connected to earth → a single fault to ground causes NO shock and no circuit breaker trip (power continues — essential in OT)
- The LIM continuously monitors for total hazard current between isolated line conductors and earth
How Link 25 works:
- When first fault occurs → LIM alarm activates (Link 25 panel shows alarm) but power NOT interrupted
- This alerts staff to find and remove faulty equipment before a second fault creates a complete circuit
- If a second fault occurs → circuit IS completed → shock hazard
- LIM alarm threshold: 5 mA hazard current (some systems 2 mA)
In practice:
- When Link 25 alarms → do not panic; power continues
- Systematically identify and unplug equipment one by one until alarm clears
- The last device unplugged is the faulty one
Electrical Safety in the Operating Theatre
Types of Electric Shock
| Type | Current | Mechanism |
|---|---|---|
| Macroshock | >1 mA felt; >100 mA VF | Current through body surface → skin resistance; household current |
| Microshock | >0.1 mA (100 µA) → VF | Current directly to heart (pacing wires, intracardiac catheters) → bypasses skin resistance |
Microshock is the primary OT concern — patients with intracardiac catheters are at risk from currents too small to feel.
Classification of OT Electrical Zones
- Zone 1: General patient environment — standard safety
- Zone 2: Cardiac procedures — isolated power supply, extra protection (IEC 60364-7-710)
- All equipment must be Type CF (cardiac float protection) for procedures with intracardiac connection
Equipment Classifications
| Class | Protection | Examples |
|---|---|---|
| Class I | Earthing | Most mains-powered devices |
| Class II | Double insulation (no earth needed) | Portable tools |
| Class III | Safety extra-low voltage <25V AC | Battery-operated |
| Type B | General patient contact | BP cuff, ECG |
| Type BF | Floating (isolated) patient circuit | Standard monitoring |
| Type CF | Cardiac floating circuit (microshock safe) | Intracardiac devices, pacemakers |
Diathermy Safety
- Monopolar diathermy: Current enters via active electrode → disperses through body → exits via large patient plate (return electrode)
- Plate must have full contact (burns if partial contact → current density ↑)
- Avoid placing over bony prominences, scar tissue, implants
- Interference with pacemakers → use bipolar diathermy or use asynchronous pacing mode
- Bipolar diathermy: Current flows between two tips; localised; safer for cardiac devices and small structures
- Capacitive coupling: In laparoscopy → current through insulation of laparoscopic instruments → bowel/vessel injury
Fire Triangle in OT
- Oxidiser: O₂ or N₂O (enriched atmospheres)
- Ignition: Diathermy, laser, cautery
- Fuel: Surgical drapes, alcohol preps, ETT
- Prevention: Use aqueous skin prep (not alcohol) near diathermy; no pooling of alcohol; oxygen-enriched atmosphere avoidance around ignition sources
Other Electrical Hazards
- Static electricity: Detonation of flammable anaesthetic agents (historically with ether/cyclopropane — now abolished)
- Lasers: CO₂, Nd:YAG — risk of ETT fire; use laser-resistant ETT, lowest FiO₂ possible
- MRI: Ferromagnetic objects, pacemaker interference → specific MRI-compatible equipment required
10. Post-operative Analgesia for Paediatric Lower Abdominal Surgery & Thoracotomy
Principles of Paediatric Analgesia
- Multimodal analgesia: Combining agents reduces total opioid requirements ("opioid-sparing")
- WHO analgesic ladder (paediatric modification): Non-opioid → weak opioid → strong opioid
- Doses are weight-based; children are NOT small adults
- Pain assessment tools: FLACC (0–2 years), Wong-Baker FACES (3–7 years), NRS (>7 years)
Lower Abdominal Surgery (Inguinal Hernia, Circumcision, Orchidopexy, Appendicectomy)
Regional Techniques
| Block | Coverage | Technique | Dose |
|---|---|---|---|
| Caudal epidural | S2–T10 (depending on volume) | Landmark or USG; sacral hiatus; 1–1.25 mL/kg | 0.2% bupivacaine (max 2 mg/kg); add adjuvants |
| Ilioinguinal/iliohypogastric nerve block | T12-L1; inguinal region | USG-guided; lateral to ASIS; in-plane needle | 0.25% bupivacaine 0.1 mL/kg each side |
| TAP block (Transversus Abdominis Plane) | T8-L1; anterior abdominal wall | USG; between internal oblique & TA | 0.25% bupivacaine 0.3 mL/kg each side (max 2.5 mg/kg total) |
| Penile nerve block | Dorsal nerve of penis (for circumcision) | Sub-pubic symphysis bilateral; avoid adrenaline | 0.25% bupivacaine 0.1 mL/kg |
| Rectus sheath block | Periumbilical (T9–11) | USG; lateral edge of rectus | For umbilical/midline incisions |
Caudal epidural is the most commonly used single-shot regional technique for infants/children undergoing lower abdominal and perineal surgery. Adjuvants to prolong caudal:
- Dexamethasone 0.1 mg/kg: Prolongs duration to ~12 hours
- Dexmedetomidine 1 µg/kg: Prolongs to 10–14 hours
- Clonidine 1–2 µg/kg: Prolongs to 6–10 hours
- Ketamine 0.5 mg/kg (preservative-free): Prolongs to ~8 hours
Systemic Analgesia (all paediatric surgery)
- Paracetamol: 15 mg/kg PO/IV q6h (max 60 mg/kg/day); safe in all ages
- NSAIDS: Ibuprofen 5–10 mg/kg q6h (>3 months); diclofenac 1 mg/kg; avoid in neonates, renal impairment, asthma
- Opioids (if needed): Morphine 0.1 mg/kg IV/IM (avoid in neonates <6 months — respiratory depression); consider PCA in >5 years
Thoracotomy in Paediatrics
Thoracotomy causes severe post-operative pain → impairs coughing, deep breathing → atelectasis, pneumonia. Aggressive analgesia is essential.
1. Thoracic Epidural Analgesia (TEA) — Gold Standard
- Most effective for thoracotomy pain
- Insert at T4–6 level (target dermatomal level T2–8)
- Drug: Bupivacaine 0.1–0.125% + fentanyl 1–2 µg/mL infusion
- Rate: 0.1–0.2 mL/kg/hr
- Provides excellent post-op analgesia 48–72 hours
- Facilitates early extubation, reduces lung complications
- Risks: PDPH, epidural haematoma/abscess, hypotension, motor block
2. Paravertebral Block (PVB)
- Excellent alternative if thoracic epidural contraindicated
- Single injection or catheter
- Unilateral analgesia (unlike bilateral epidural); less hypotension
- USG-guided: Identify paravertebral space (loss of resistance / USG visualisation of pleural displacement)
- Drug: 0.5 mL/kg bupivacaine 0.25–0.5% (max 2 mg/kg) per level; or catheter infusion
- Advantages over TEA: Less haemodynamic instability, no urinary retention, easier in coagulopathy
3. Intercostal Nerve Blocks
- Simple, effective; surgeon can inject under direct vision
- Bupivacaine 0.25% 0.5 mL/kg per level (max 2 mg/kg total)
- Short duration (4–6 hours); multiple levels required
- Significant systemic absorption from intercostal space → toxicity risk (highest absorption rate of any block site)
4. Serratus Anterior Plane Block (SAPB)
- USG-guided; between serratus anterior and latissimus dorsi
- Covers T2–T9 lateral chest wall
- Technically easier; no neuraxial risks
- Increasing use in paediatric thoracic surgery
5. PECS II Block
- USG-guided; covers medial/lateral pectoral nerves + intercostobrachial
- Less evidence in children; used in older paediatric patients
6. Systemic Adjuncts
- IV paracetamol 15 mg/kg q6h
- Ketorolac 0.5 mg/kg q6h (>1 year; short course only)
- IV morphine PCA (>5 years) or NCA (nurse-controlled) in younger
- Dexmedetomidine infusion 0.2–0.5 µg/kg/hr (opioid-sparing, anxiolysis)
- Gabapentin (limited paediatric evidence for post-thoracotomy)
ERAS for Paediatric Thoracotomy
- Preoperative education, premedication (midazolam 0.5 mg/kg PO)
- Regional anaesthesia first
- Multimodal analgesia
- Early oral feeding
- Early physiotherapy and ambulation
Quick Reference Summary Table
| Topic | Key Points |
|---|---|
| Resuscitation in pregnancy | Left lateral tilt, early intubation, PMCS at 4 min; Surviving Sepsis Hour-1 bundle: lactate, cultures, antibiotics, 30 mL/kg fluid, noradrenaline |
| LFTs + Child-Pugh | ALT=hepatocellular; ALP=cholestatic; Albumin+PT=synthetic function; Child-Pugh A/B/C based on 5 parameters |
| Adductor canal block | Supine, linear probe mid-thigh, saphenous nerve anterior to SFA, 15–20 mL LA; preserves quadriceps |
| RRT | AEIOU indications; CRRT preferred in ICU; CVVH (convection) vs IHD (diffusion) |
| Labour analgesia | CSE=gold standard (rapid onset + flexibility); pain T10–L1 (1st stage) + S2–4 (2nd stage) |
| Posterior fossa | Sitting position = VAE risk; TIVA for neuromonitoring; avoid N₂O; precordial Doppler; PMCS at 4 min → surgeon ready |
| Maxillofacial trauma | MILS + collar off; VL preferred; avoid nasal intubation if basal skull fracture; scalpel-bougie for CICO |
| Paediatric FB | Gaseous induction (preserve spontaneous ventilation); rigid bronchoscopy; atropine premedication |
| Stored blood changes | ↓ pH, ↑ K⁺, ↑ CO₂, ↓ 2,3-DPG, ↓ Ca²⁺, ↓ clotting factors; TRALI = leading transfusion death |
| Link 25 + electrical safety | Isolated power supply; LIM alarms but doesn't cut power; macroshock vs microshock; Type CF for intracardiac |
| Paediatric post-op analgesia | Lower abdominal: caudal ± adjuvants, TAP/ilioinguinal; Thoracotomy: thoracic epidural or paravertebral (gold standard) |
This is a shared conversation. Sign in to Orris to start your own chat.