explain me physiology of pregancy and birth from guyton
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Guyton. Let me compose the full detailed answer:
Physiology of Pregnancy and Birth - Guyton & Hall
1. Maturation and Fertilization of the Ovum
While still in the ovary, the ovum is in the primary oocyte stage. Just before ovulation, its nucleus undergoes meiosis, expelling the first polar body - the ovum becomes a secondary oocyte with 23 unpaired chromosomes.
Entry into the Fallopian Tube: The ovum, surrounded by ~100 granulosa cells (the corona radiata), is expelled into the peritoneal cavity at ovulation. Ciliated epithelium at the fimbriated ends of the fallopian tube (activated by estrogen) sweeps the ovum toward the ostium. Up to 98% of ova successfully enter the tube.
Fertilization: Sperm deposited in the vagina travel to the ampulla of the fallopian tube within 5-10 minutes, aided by uterine/tubal contractions stimulated by prostaglandins in seminal fluid and oxytocin from the female pituitary. Of ~500 million sperm deposited, only a few thousand reach each ampulla. Fertilization normally occurs in the ampulla. Once a sperm penetrates the zona pellucida, the oocyte completes its second meiotic division and expels the second polar body, forming the mature ovum. The 23 chromosomes of the sperm then combine with the 23 of the ovum to restore the diploid count of 46.
2. Implantation of the Blastocyst
The fertilized ovum, now a zygote, undergoes cleavage as it travels through the fallopian tube. By day 3-4 it reaches the uterus as a morula, then becomes a blastocyst.
Trophoblastic digestion of the endometrium allows implantation, typically in the upper uterus. The outer cell layer (trophoblast) secretes proteolytic enzymes and hyaluronidase that digest and liquefy endometrial cells, which are then absorbed as nutrition for the early embryo. Implantation normally occurs about 7-9 days after fertilization.
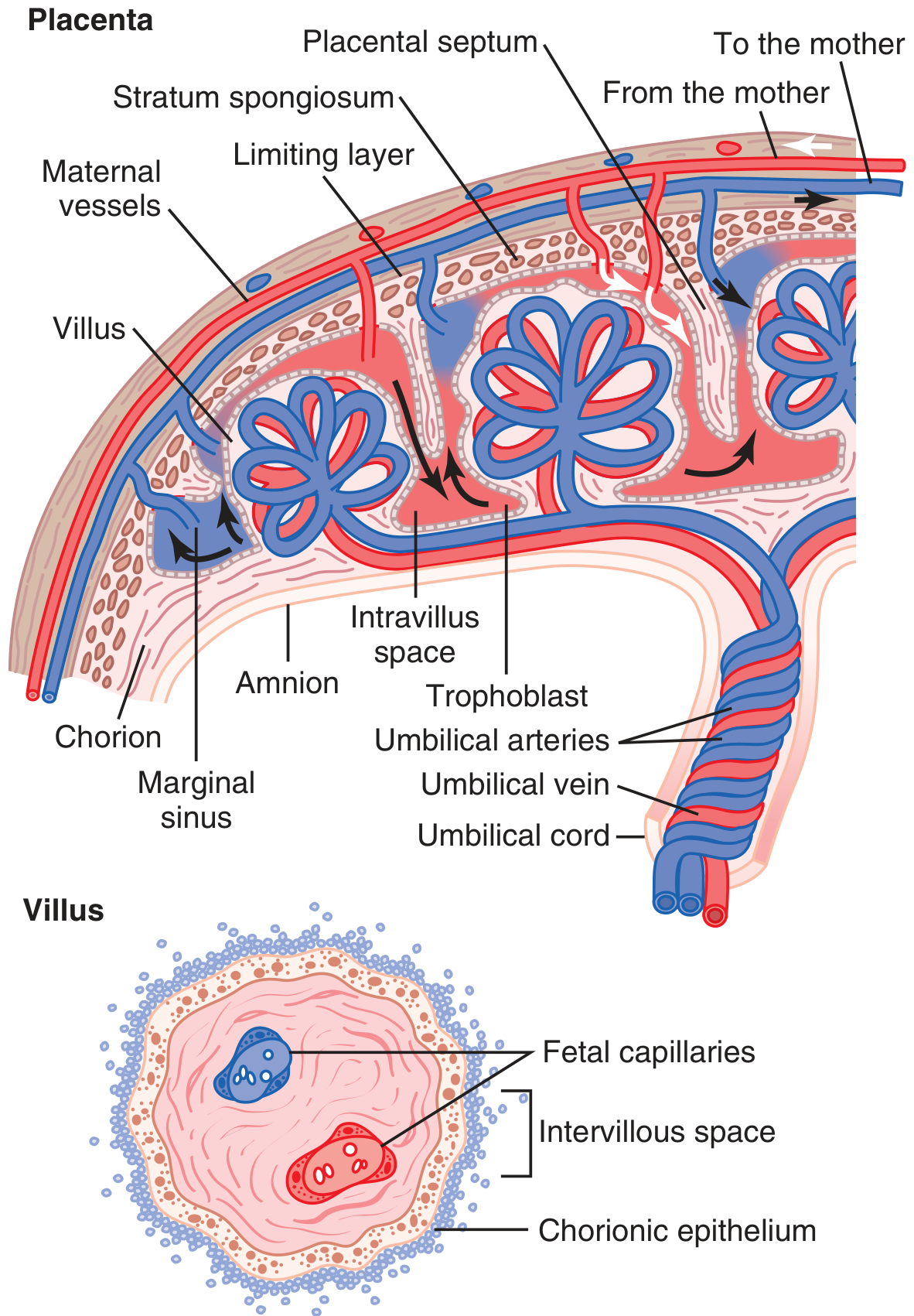
3. Anatomy and Function of the Placenta
The trophoblastic cords from the blastocyst attach to the uterus, and blood capillaries from the forming embryo grow into these cords. By 21-23 days after fertilization, the fetal heart begins pumping blood. The placenta forms the following structure:
- Fetal blood flows via two umbilical arteries → villus capillaries → single umbilical vein back to fetus
- Maternal blood flows from uterine arteries → large maternal sinuses surrounding the villi → uterine veins
The two circulations never mix directly - diffusion across the placental membrane handles all exchange.
Placental Permeability: In early pregnancy the membrane is thick and has low permeability, but it thins markedly as pregnancy advances, and the surface area expands enormously - greatly increasing diffusion conductance across gestation.
The placenta transfers:
- Oxygen by diffusion (fetal hemoglobin has higher O2 affinity than maternal hemoglobin)
- Glucose, amino acids, fatty acids to the fetus
- CO2 and urea from fetus to mother
- IgG antibodies (passive immunity to the neonate)
- Various drugs, alcohol, nicotine, and some viruses can cross the membrane
4. Hormonal Factors in Pregnancy
The placenta secretes four major hormones: hCG, estrogens, progesterone, and human chorionic somatomammotropin (hCS/hPL).
Human Chorionic Gonadotropin (hCG)
- Secreted by syncytial trophoblast cells; detectable in blood 8-9 days after ovulation
- Peaks at 10-12 weeks, then falls to a lower plateau for the rest of pregnancy
- Key function: Prevents involution of the corpus luteum - instead, the corpus luteum grows to ~twice its size and continues secreting progesterone and estrogens, preventing menstruation and maintaining the decidua
- If the corpus luteum is removed before week 7, abortion almost always results; removal between weeks 7-12 risks abortion; after week 12-13, the placenta itself secretes enough progesterone/estrogen
- Also stimulates the fetal testes to produce testosterone (required for male genital development)
- Forms the basis of pregnancy tests (urine/serum hCG)
Estrogens
- Secreted by the placenta, primarily as estriol (unlike ovarian estradiol)
- Require androgenic precursors from both the fetal and maternal adrenal cortices (placenta lacks full steroid synthesis machinery)
- Effects in pregnancy:
- Enlargement of uterus, breasts, and external genitalia
- Breast ductal growth
- Relaxation of pelvic ligaments (pelvis widens for delivery)
- Increased uterine contractility (especially near term)
- Fluid retention
Progesterone
- Secreted in increasing amounts throughout pregnancy
- Inhibits uterine contractility - essential for keeping the fetus in utero
- Promotes decidual cell development for early fetal nutrition
- Prepares the breasts for lactation (alveolar development)
- Suppresses the maternal immune rejection of the fetus
Human Chorionic Somatomammotropin (hCS / hPL)
- Secreted progressively throughout pregnancy; at term, ~1 gram/day (largest hormone output of any endocrine gland)
- Structurally similar to growth hormone
- Decreases maternal insulin sensitivity - causes mild diabetic-like state, sparing glucose for the fetus
- Promotes lipolysis in the mother, providing fatty acids as maternal fuel
- Mild anabolic and lactogenic effects
Other Hormones
- Relaxin (from corpus luteum, then placenta) - relaxes the pubic symphysis and cervical ligaments
- Increased cortisol, aldosterone, thyroxine during pregnancy
- Prolactin rises progressively
5. Response of the Mother's Body to Pregnancy
Body Changes
- Uterus: 50 g → ~1100 g
- Breasts approximately double in size
- Average weight gain: 25-35 lbs - ~8 lb fetus, 4 lb placenta/membranes/fluid, 3 lb uterus, 2 lb breasts, 5 lb extra blood/ECF, 3-13 lb fat stores
Metabolism
- Basal metabolic rate increases ~15% in the latter half of pregnancy due to elevated thyroxine, adrenocortical hormones, sex hormones, and added fetal tissue
Nutrition
- The fetus almost doubles in weight in the last 2 months
- Key needs: protein, calcium, phosphate, iron (fetus needs ~375 mg iron for blood; mother needs ~600 mg extra for her own)
- Hypochromic anemia is common if iron intake is inadequate
- Vitamin D is critical for calcium absorption
- Vitamin K is given near term to prevent neonatal hemorrhage
Circulatory Changes
- Cardiac output increases 30-40% above normal by the third trimester
- Blood volume increases ~30% (extra plasma + red cells)
Respiratory Changes
- Tidal volume and minute ventilation increase significantly (partly due to progesterone acting as a respiratory stimulant)
- Slight respiratory alkalosis is normal
Kidney Function
- Glomerular filtration rate (GFR) increases ~50%
- Renal plasma flow increases
- Glucosuria can occur even with normal blood glucose (due to increased filtered load exceeding tubular reabsorption capacity)
- Aldosterone rises, promoting Na+ retention; but progesterone competes with aldosterone at the tubule
6. Parturition - Birth of the Baby
Near term, two major categories of changes drive the onset of labor:
Hormonal Factors Increasing Uterine Contractility
-
Estrogen/Progesterone ratio shift: From the 7th month onward, estrogen secretion continues rising while progesterone stays flat or slightly decreases. The rising estrogen-to-progesterone ratio increases uterine excitability - estrogen increases gap junctions between uterine smooth muscle cells, synchronizing contractions.
-
Oxytocin: The uterus increases its oxytocin receptors near term, greatly amplifying its response. Oxytocin secretion from the neurohypophysis increases during labor. Cervical irritation/stretching triggers a neuroendocrine reflex through the hypothalamus to increase oxytocin release (Ferguson reflex).
-
Fetal hormones: The fetal pituitary secretes oxytocin; fetal adrenals secrete cortisol; fetal membranes release prostaglandins in high concentrations - all contributing to uterine stimulation.
Mechanical Factors
- Stretch of uterine musculature (smooth muscle contractility increases with stretch) - explains why twins are born ~19 days earlier on average
- Cervical stretch/irritation triggers oxytocin release via the hypothalamus
Positive Feedback Mechanism of Labor (Ferguson Reflex)
This is a classic positive feedback loop in physiology:
- Uterine contractions push the fetal head against the cervix
- Cervical stretching sends nerve signals to the hypothalamus
- Hypothalamus triggers oxytocin release from the neurohypophysis
- Oxytocin causes stronger uterine contractions
- Stronger contractions push the head harder against the cervix
- This continues until the baby is delivered and the cycle breaks
Stages of Labor
Abdominal muscles contribute significantly during pushing, adding to the ~25 lbs of downward force per strong contraction. Contractions initially occur every 30 minutes, eventually every 1-3 minutes with high intensity.
-
First Stage: Progressive cervical dilation until the cervix is as wide as the fetal head. Lasts 8-24 hours in first delivery, may be only minutes in subsequent ones. Pain from uterine muscle hypoxia (visceral pain via hypogastric nerves).
-
Second Stage: After full cervical dilation, fetal membranes rupture, amniotic fluid escapes, and the head descends through the birth canal. Lasts 1 minute to 30+ minutes. Pain is somatic (cervical, perineal, and vaginal stretching via somatic nerves) - much more intense.
-
Third Stage (Placental delivery): Uterus contracts for 10-45 minutes post-delivery, shearing the placenta from the uterine wall. Average blood loss ~350 mL, limited by:
- Figure-of-eight smooth muscle arrangement around uterine vessels - uterine contraction directly compresses the vessels
- Vasoconstrictive prostaglandins at the separation site
In >95% of births, the head presents first (vertex presentation). Buttocks/feet first = breech presentation.
7. Involution of the Uterus After Delivery and Lactation
After delivery:
- Placental hormones drop rapidly
- Uterus involutes back toward normal size over about 4-6 weeks
- Retained fluid (5 lbs extra) is excreted in the first few days postpartum as the fluid-retaining hormones (estrogen, progesterone, aldosterone) fall
Oxytocin released during suckling drives milk ejection and also accelerates uterine involution.
Source: Guyton and Hall Textbook of Medical Physiology (14th ed., ISBN 9780443111013), Chapter 83 - Pregnancy and Lactation, pp. 1032-1048.
This is a shared conversation. Sign in to Orris to start your own chat.