Dysgerminoma treatment
Reading File
Finding Sources
Searching PubMed
dysgerminoma treatment chemotherapy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have a complete picture from both textbooks plus the management flowchart. Here is the full, organized answer.
Dysgerminoma - Treatment
Background
Dysgerminoma is the ovarian counterpart of testicular seminoma and is the most common malignant ovarian germ cell tumor (30-40% of all malignant germ cell tumors; ~2% of all ovarian cancers). Seventy-five percent occur between ages 10-30. It is the only ovarian germ cell tumor with a significant bilaterality rate (~10-15% of stage I cases). About 65% present at stage I.
Histology:
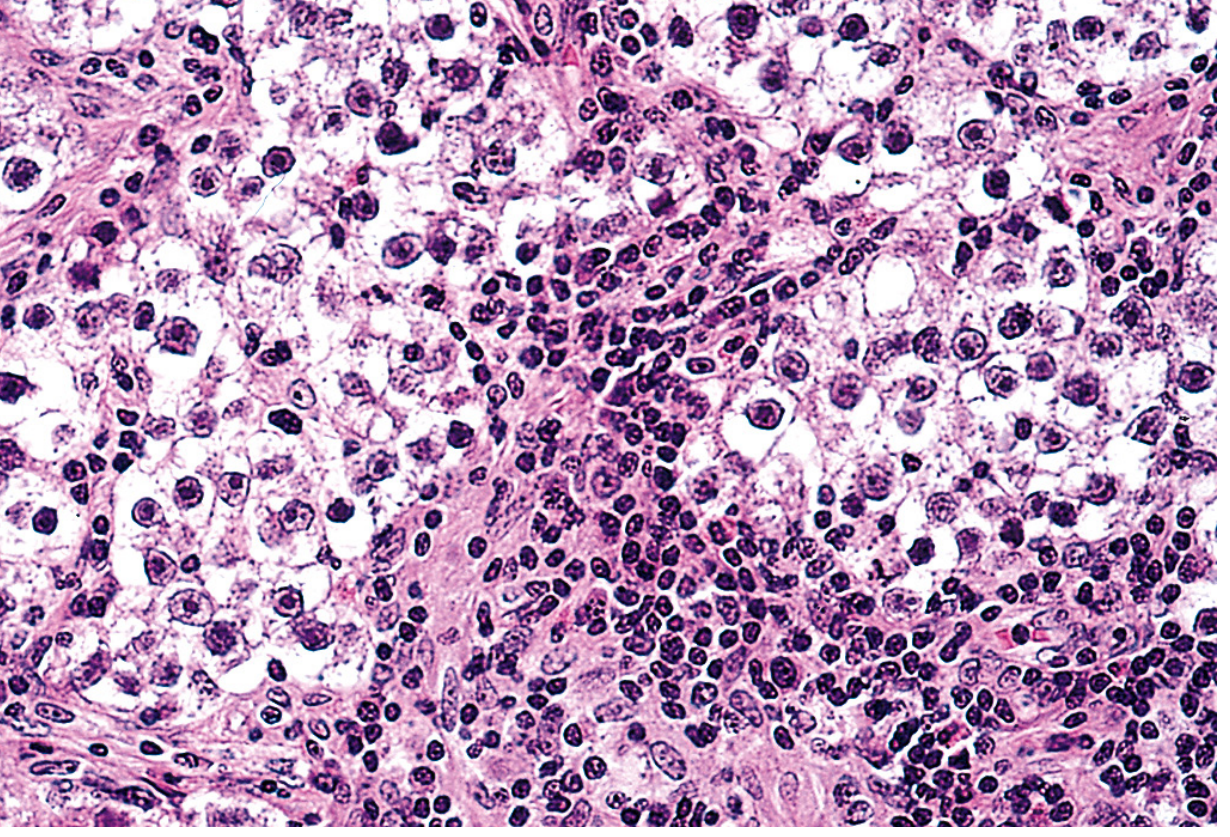
Large vesicular cells with clear cytoplasm in sheets/cords, separated by fibrous stroma infiltrated by lymphocytes and sometimes granulomas. Expresses OCT3/4, NANOG, KIT (~30-50% activating KIT mutations).
Management Algorithm
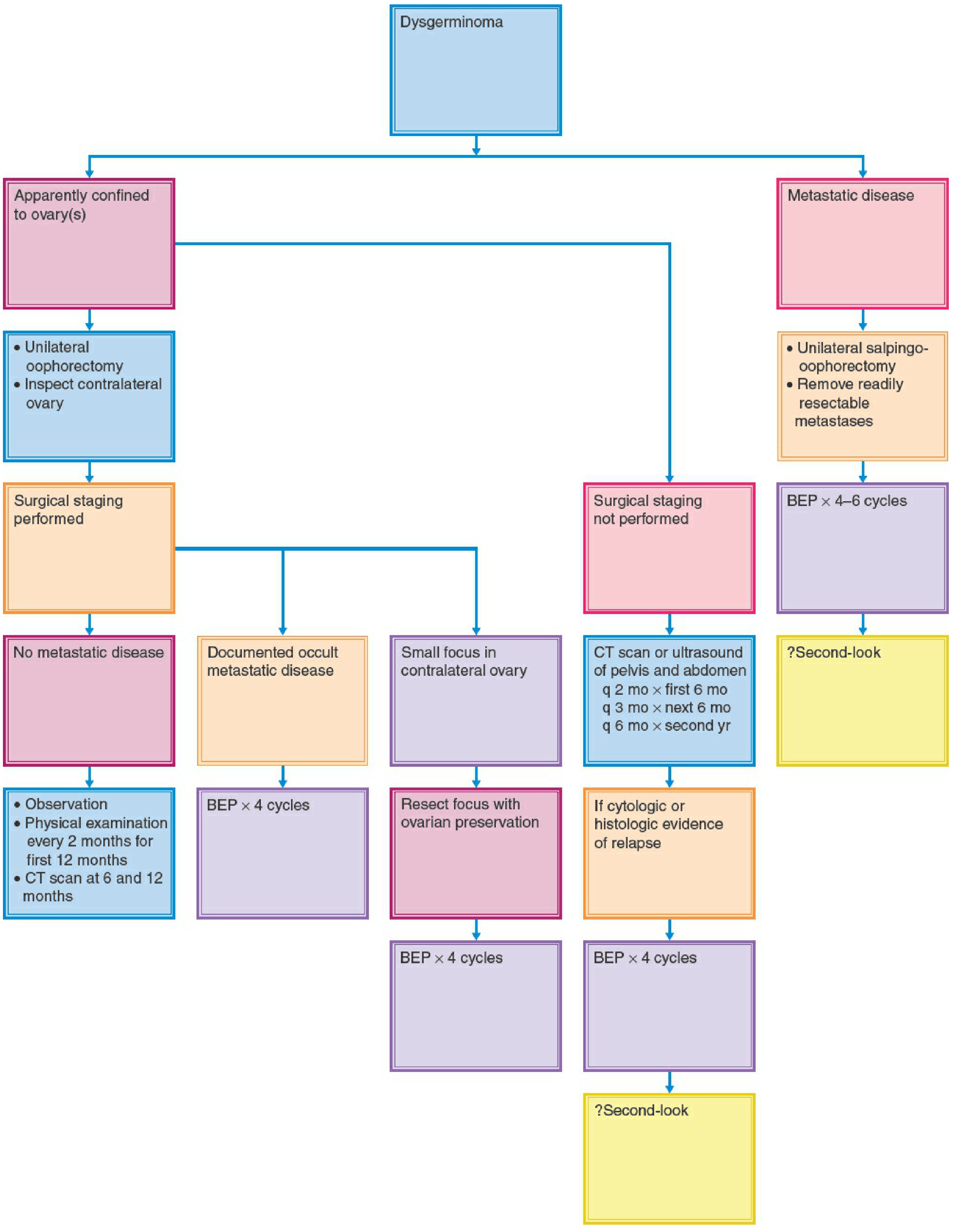
1. Surgery (Primary Treatment for Early Disease)
The minimum surgical procedure is unilateral oophorectomy (or unilateral salpingo-oophorectomy). Fertility preservation is almost always the goal since this tumor predominantly affects young women.
Key surgical principles:
| Situation | Approach |
|---|---|
| Apparent stage I, fertility desired | Unilateral oophorectomy + thorough surgical staging |
| Fertility not desired, advanced disease | Total abdominal hysterectomy + bilateral salpingo-oophorectomy |
| Y chromosome in karyotype (gonadal dysgenesis) | Bilateral oophorectomy; uterus may be preserved for future embryo transfer |
| Small focus in contralateral ovary | Resect focus with ovarian preservation |
| Metastatic disease, fertility desired | Unilateral salpingo-oophorectomy + remove readily resectable metastases |
Staging includes: Inspection and palpation of all peritoneal surfaces, unilateral pelvic lymphadenectomy, palpation/biopsy of para-aortic nodes (tumors metastasize to para-aortic nodes near the renal vessels), and biopsy of any suspicious lesions.
2. Post-Surgical Management by Stage
Stage IA (unilateral, encapsulated - no staging performed)
- Options:
- Completion surgical staging (preferred - stage IA does not require adjuvant chemo)
- Close surveillance - CT pelvis/abdomen and tumor markers (LDH, AFP, beta-hCG) at q2 months x 6 months, q3 months x next 6 months, q6 months x second year
- Adjuvant chemotherapy if capsular rupture or more advanced stage found
Stage IA (surgically staged, no metastatic disease)
- Observation - physical exam every 2 months for 12 months, CT at 6 and 12 months
- 5-year disease-free survival >95% with surgery alone
Stage IB/IC, II, III (occult or documented metastatic disease)
- BEP x 4 cycles (see regimen below)
Stage III/IV (advanced, incompletely resected)
- BEP x 3-4 cycles (risk-stratified based on testicular germ cell tumor data)
- GOG data: 19/20 patients with stage III/IV dysgerminoma treated with cisplatin-based regimens were alive and disease-free at median 26 months
3. Chemotherapy
Platinum-based chemotherapy is the treatment of choice, with the major advantage of fertility preservation.
First-Line Regimens
| Regimen | Drugs and Doses |
|---|---|
| BEP (standard) | Bleomycin 30,000 IU IV on days 1, 8, 15 q3wk; Etoposide 100 mg/m²/day x 5 days q3wk; Cisplatin 20 mg/m²/day x 5 days (or 100 mg/m² x 1 day) q3wk |
| EP | Etoposide + Cisplatin (without bleomycin) |
| EC (GOG protocol) | Etoposide 120 mg/m² IV days 1-3 q4wk; Carboplatin 400 mg/m² IV day 1 q4wk - 100% disease-free remission in completely resected stage IB-III |
- Standard: 3-4 cycles of BEP, number determined by risk stratification analogous to seminoma protocols
- VBP (vinblastine, bleomycin, cisplatin) was used historically but is now largely replaced by BEP
4. Radiation Therapy
Dysgerminomas are highly radiosensitive (2,500-3,500 cGy can be curative even for gross metastatic disease). However, radiation is rarely used as first-line treatment because:
- Loss of fertility (if pelvic/abdominal fields required)
- Chemotherapy achieves equivalent or superior cure rates while preserving fertility
Radiation may be considered in very selected subsets with recurrent disease.
5. Recurrent Disease
- ~75% of recurrences occur within the first year; most common sites are the peritoneal cavity and retroperitoneal lymph nodes
- Patients not previously treated with chemotherapy: standard first-line BEP
- Patients who relapse after BEP:
- TIP (paclitaxel, ifosfamide, cisplatin)
- VIP (vinblastine, ifosfamide, cisplatin)
- High-dose chemotherapy (in selected patients) - manage in specialized centers
- Radiation as a last resort
6. Special Considerations
- Tumor markers: LDH (primary marker), AFP, beta-hCG should be monitored even in pure dysgerminoma because occult mixed germ cell elements (e.g., yolk sac tumor) may produce AFP elevation
- Syncytiotrophoblastic giant cells in the tumor may elevate beta-hCG; this does not alter prognosis
- Gonadal dysgenesis patients (45,X/46,XY; androgen insensitivity): dysgerminomas commonly arise in gonadoblastomas; if gonadoblastoma is left in situ, >50% develop into ovarian malignancy - bilateral gonadectomy recommended
- KIT mutations (~30-50%) represent a potential target for imatinib, though this remains investigational
- Features predicting higher recurrence risk: tumor >10-15 cm, age <20, high mitotic index, anaplastic or medullary histologic pattern
Prognosis
| Stage | Outcome |
|---|---|
| Stage IA (unilateral, encapsulated) | >95% 5-year disease-free survival after oophorectomy alone |
| All stages (chemo-treated) | Excellent; even stage III/IV disease is often curable |
Overall, dysgerminoma has one of the best prognoses of any malignant ovarian tumor due to its exquisite sensitivity to both chemotherapy and radiation.
Sources:
- Berek & Novak's Gynecology, pp. 2379-2387
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 947
- Recent reviews: Dysgerminoma of the ovary (Minerva Obstet Gynecol, 2025; PMID 38953909), Malignant germ cell tumors of the ovary (J Gynecol Oncol, 2025; PMID 40275685)
This is a shared conversation. Sign in to Orris to start your own chat.