Pneumothorax Detail explanations in Hinglish
Reading File
Finding Sources
Searching PubMed
pneumothorax management
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Ab main saari information ko mila ke ek complete Hinglish explanation present karta hoon.
🫁 PNEUMOTHORAX - Poori Detail Hinglish Mein
1. PNEUMOTHORAX KYA HAI? (Definition)
"Pneumo" = Air (hawa) | "Thorax" = Chest cavity (seene ki jagah)
Seedha baat karo toh - pleural space mein hawa ghus jaana hi Pneumothorax hai.
Normal mein, humare lungs ke bahar ek double layer hoti hai - Visceral Pleura (lung se chipki) aur Parietal Pleura (chest wall se chipki). In dono ke beech ka space normally bahut tight hota hai aur negative pressure (vacuum jaisa) maintain hota hai. Jab is space mein hawa aa jaati hai, toh lung collapse (pichak jaata) ho jaata hai.
Sochlo jaise ek balloon ho - agar uske bahar hawa bharo, toh balloon pichak jayega. Exactly waisa hi lung ke saath hota hai.
"Air in the pleural space is a common clinical problem" - Murray & Nadel's Respiratory Medicine
2. TYPES (Prakar)
A. 🌟 Primary Spontaneous Pneumothorax (PSP)
- Kise hota hai: Healthy young log, koi known lung disease nahi
- Classic patient: Tall (lamba), thin (patla) young male
- Reason: Subpleural blebs ya bullae (choti choti hawa ki theli) phoot jaati hain
- Men mein women se 3 guna zyada common
- Marfan syndrome aur mitral valve prolapse mein risk badha hua
B. 🏥 Secondary Spontaneous Pneumothorax (SSP)
- Kise hota hai: Jo pehle se kisi lung disease se peedit hain
- Primary se 15-20 saal zyada umra ke patients mein
- Zyada serious hota hai kyunki lungs pehle se weak hain - dyspnea hamesha hogi chahe pneumothorax chota ho
SSP ke causes (Karan):
| Category | Disease |
|---|---|
| Airway Disease | COPD (sabse common in USA), Asthma, Cystic Fibrosis |
| Infections | TB (developing countries mein #1), PCP (HIV patients mein), Lung Abscess |
| Interstitial | Sarcoidosis, IPF, Lymphangiomyomatosis |
| Cancer | Primary lung cancer, Metastases |
| Connective Tissue | Marfan syndrome, Ehlers-Danlos, Scleroderma, RA |
C. ⚠️ Tension Pneumothorax - LIFE THREATENING!
- One-way valve mechanism - Hawa andar jaati hai, bahar nahi nikal sakti
- Har breath ke saath pleural space mein hawa badhti rehti hai
- Mediastinal shift hota hai (heart doosri taraf khisak jaata hai)
- Venous return rukt jaata hai - Cardiovascular collapse aur death ho sakti hai
- EMERGENCY hai - diagnosis clinical hai, X-ray ka wait mat karo!
D. 🔧 Traumatic Pneumothorax
- Chest injury se (rib fracture, knife wound, bullet)
- CPR ya bag-valve-mask ventilation se bhi ho sakta hai
E. 💉 Iatrogenic Pneumothorax
- Medical procedure se - Central line, pacemaker insertion, lung biopsy
F. 🩸 Catamenial Pneumothorax
- Menstrual cycle ke saath associated (endometriosis se related)
- Rare but interesting entity
3. PATHOPHYSIOLOGY (Andar kya hota hai?)
Normal state:
Visceral pleura + Parietal pleura = Negative intrapleural pressure
↓
Lung phule rehta hai
Pneumothorax mein:
Alveolar-pleural barrier toot jaata hai
↓
Hawa pleural space mein enter karti hai
↓
Negative pressure khatam ho jaata hai
↓
Lung pichak jaata hai (collapse)
PSP mein: Subpleural bleb/bulla rupture hoti hai. Smoking aur chronic bronchospasm se intraalveolar pressure badh jaata hai jo in blebs ko phod deta hai.
Tension Pneumothorax mein: Defect ek one-way valve ki tarah kaam karta hai:
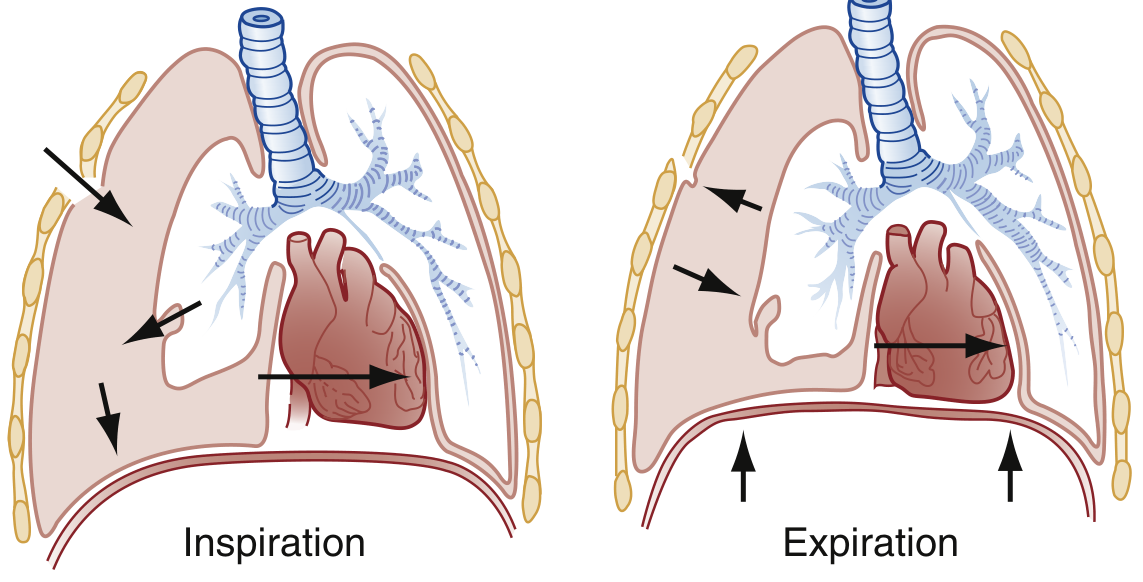
Diagram: Inspiration mein hawa pleural space mein ghus jaati hai, expiration mein woh trapped reh jaati hai. Progressive accumulation se mediastinal shift aur cardiovascular collapse hota hai.
4. CLINICAL FEATURES (Symptoms - Kya feel hoga?)
Simple Pneumothorax mein:
- Sudden onset chest pain - ipsilateral side pe, pleuritic (saans lete waqt badhta hai)
- Dyspnea (saans phoolna) - degree varies
- Pehle sharp pain, baad mein dull ache ho jaati hai
- Kai baar symptoms mild hote hain, patient 1-2 din baad hospital aata hai
- 24-72 hours mein symptoms khud improve ho sakte hain (par pneumothorax remain karta hai)
Physical Examination:
- Sinus tachycardia - sabse pehla sign
- Decreased/absent breath sounds - affected side pe
- Hyper-resonance on percussion (dhak dhak sound)
- Absent tactile fremitus
- Unequal chest movement
- Hypoxia - large pneumothorax mein
⚡ Tension Pneumothorax mein (CRITICAL SIGNS):
- Tachycardia (har dhad kaanpna)
- Hypotension (late finding)
- JVD - Jugular Vein Distension (gardan ki naseein ubhar aana)
- Tracheal deviation - doosri taraf (late finding)
- Elevated peak airway pressure (ventilated patient mein)
- Absent breath sounds - affected side
- Cardiovascular collapse - agar treat na karo
Yaad rakho: Sab signs ek saath nahi milenge. Clinical judgement se treat karo!
5. DIAGNOSIS (Pehchaan kaise karein?)
Chest X-ray (Sabse pehle):
Classic finding: Chest wall ke parallel ek thin visceral pleural line dikh rahi hogi, uske baad ek radiolucent band (kala area without lung markings)

Chest X-ray: Pleural line aur radiolucent band clearly visible
Size estimate (BTS Guidelines):
- Small: < 1 cm intrapleural distance at hilum level
- Moderate: 1-2 cm
- Large: > 2 cm
American ACCP Guidelines:
- Small: < 3 cm (apex to cupola)
- Large: ≥ 3 cm
Ultrasound (POCUS - Bedside):
- Pleural sliding present = Pneumothorax nahi hai (rule out)
- Pleural sliding absent = Suspicious (but confirm karna padega)
- "Lung point" - sliding ka ek jagah hona aur doosri jagah na hona = highly specific for pneumothorax
- "Seashore sign" = Normal
- "Barcode/Stratosphere sign" = Pneumothorax
CT Scan:
- Loculated (pocketed) collections ke liye best
- Exact size aur anatomy deta hai
⚡ IMPORTANT: Tension pneumothorax mein X-ray ka wait mat karo! Clinical diagnosis pe immediately treat karo.
6. DIFFERENTIAL DIAGNOSIS (In conditions se alag karna padega)
- Pulmonary Embolism - same symptoms, similar presentation
- Acute MI - ECG changes pneumothorax mein bhi aa sakte hain
- Pleuritis/Pleural Effusion - X-ray se distinguish
- Pericarditis/Cardiac Tamponade - ultrasound se alag karo
- Pneumomediastinum - subcutaneous emphysema pe dhyan do
- Hemopneumothorax - hawa + blood dono hain pleural space mein
7. TREATMENT (Ilaj)
🟢 Conservative (Small, Stable, No symptoms):
- Small spontaneous pneumothorax in otherwise healthy patient
- 4-6 hours baad repeat X-ray lo
- Agar expand nahi ho raha - observe karo
- NOTE: Ye option ventilated patients mein mat use karna! (Simple se Tension ban sakta hai)
- Supplemental oxygen dene se hawa reabsorb zyada quickly hoti hai
🟡 Needle Aspiration:
- Simple pneumothorax mein
- 2nd intercostal space, midclavicular line pe needle
🟠 Chest Tube (Tube Thoracostomy):
Indications:
- Traumatic pneumothorax (asymptomatic apical ke alawa)
- Moderate-large pneumothorax
- Respiratory symptoms chahe size koi bhi ho
- Size increasing on serial X-rays
- Recurrence after previous chest tube
- Ventilated patient
- Small-bore tube (24 Fr) ya pigtail catheter - Seldinger technique se
- Water seal chamber use karo
- Persistent air leak ke liye continuous suction (20 cm H2O)
🔴 Tension Pneumothorax - IMMEDIATE ACTION:
Step 1: Needle Decompression (Emergency)
- 2nd ICS, midclavicular line - needle se hawa nikaalo
- Recent meta-analysis (2025) ke according needle length aur site pe naye guidelines aa rahe hain (PMID: 40383767)
Step 2: Chest Tube
- Needle ke baad definitive management ke liye chest tube
🔵 Surgical (Recurrence prevention):
- Indications: 2nd ipsilateral pneumothorax, bilateral, persistent air leak
- VATS (Video-Assisted Thoracoscopic Surgery) - blebs ko surgically remove karna
- Pleurodesis - pleural surfaces ko permanently seal karna (talc ya chemical)
8. SPECIAL POPULATIONS
Ventilated Patients mein:
- Always drain karo - simple se tension mein convert hone ka risk zyada
- COPD aur asthma patients mein risk higher
- Loculated collections ke liye CT-guided drainage
Children mein:
- PSP aur SSP ke principles same hain adults ki tarah
- Breath sounds dhyan se sunna - children mein distributed hote hain
- Routine X-ray sab chest pain mein nahi, par suspicion ho toh zaroor
9. QUICK SUMMARY TABLE
| Feature | PSP | SSP | Tension |
|---|---|---|---|
| Age | Young (15-34) | Older (>50) | Any |
| Lung disease | None | Present (COPD, TB etc.) | Any pneumothorax |
| Severity | Mild-Moderate | Serious | Life-threatening |
| Dyspnea | Variable | Always | Severe |
| Tracheal deviation | No | No | Yes (late) |
| BP | Normal | Normal | Low (late) |
| Treatment | Conservative/Aspiration | Chest tube | IMMEDIATE decompression |
10. MNEMONIC (Yaad rakhne ke liye)
Tension Pneumothorax signs = "3T + ABCD"
- Tachycardia
- Tracheal deviation (away from affected side)
- Tympanic (hyper-resonant) percussion
- Absent breath sounds
- BP low (hypotension - late)
- Cyanosis
- Distended neck veins (JVD)
Sources: Rosen's Emergency Medicine (9th ed.), Murray & Nadel's Textbook of Respiratory Medicine, Roberts & Hedges' Clinical Procedures in Emergency Medicine
Recent evidence: 2025 meta-analysis (PMID: 40383767) ne needle decompression ke optimal length aur site pe naye consensus recommendations diye hain jo ATLS guidelines ko update karte hain.
This is a shared conversation. Sign in to Orris to start your own chat.