Hernia according to surgery
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Bailey & Love covering all major aspects of hernia in surgery. Let me now compile the full, detailed answer.
Hernia - A Comprehensive Surgical Overview
(Source: Bailey and Love's Short Practice of Surgery 28th Edition; Schwartz's Principles of Surgery 11th Edition)
1. Definition
A hernia is an abnormal protrusion of an organ or tissue through an opening in the layer that normally confines it. Abdominal hernias push from the inside outward, taking with them all coverings of the abdominal wall (though often thinned and attenuated). Not all abdominal hernias have a peritoneal sac - for example, many epigastric hernias arise in interstitial layers and draw peritoneum into the protrusion only secondarily as they enlarge.
2. Anatomy and Causes of Herniation
Anatomical causes are classified as:
| Category | Examples |
|---|---|
| Natural weakness (no muscle) | Lumbar triangles, posterior wall of inguinal canal |
| Structures entering/leaving the abdomen | Inguinal canal, femoral canal, oesophageal hiatus, umbilical cicatrix |
| Developmental/congenital failures | Failure of processus vaginalis closure (indirect inguinal hernia), Bochdalek/Morgagni (diaphragm) |
| Injury/surgical disruption | Incisional (10% of laparotomies), traumatic (high-speed MVA) |
Causes of hernia (summary):
- Anatomical weakness
- Developmental failures (e.g., patent processus vaginalis)
- Genetic weakness of collagen
- Sharp and blunt trauma
- Ageing and pregnancy
- Primary neurological and muscle diseases
3. Pathophysiology
Hernia is strongly linked to a collagen disease - an inherited imbalance in collagen types. Evidence includes histological findings and associations with aortic aneurysm and Ehlers-Danlos syndrome. Smoking impairs collagen maturation, increasing hernia risk.
- A surgical scar has only 70% of original muscle strength even with perfect healing - hence incisional hernia in >10% of laparotomy wounds
- Laparoscopic port-site hernia rate is approximately 1%
4. Components of a Hernia
Every hernia has two essential elements:
- The defect - opening in the fascial/muscular wall (small rigid defects carry highest strangulation risk)
- The content - tissue/organ protruding through (fat, omentum, bowel, bladder)
- The sac - a covering of peritoneum dragged through the defect (not always present)
Types by reducibility:
| Type | Description | Risk |
|---|---|---|
| Reducible | Contents freely move in and out | Low immediate risk |
| Irreducible (Incarcerated) | Contents stuck; cannot be returned | Higher risk |
| Obstructed | Bowel loops within the sac are obstructed but blood supply intact | Bowel obstruction |
| Strangulated | Blood supply to the contents is compromised | Surgical emergency |
| Sliding | Part of the sac wall is formed by the content (e.g., bowel/bladder) | - |
Special types:
- Richter's hernia - Only part of the bowel wall (antimesenteric) is caught in the defect; complete obstruction may be absent but strangulation can still occur silently
- Littre's hernia - Sac contains a Meckel's diverticulum
- Maydl's hernia - Two loops of bowel in the sac; the intervening loop inside the abdomen becomes strangulated ("W" hernia)
5. Classification of Hernia
A. By location:
Groin Hernias:
- Inguinal (indirect / direct)
- Femoral
Ventral Hernias:
| Primary | Secondary |
|---|---|
| Umbilical | Incisional |
| Epigastric | Parastomal |
| Spigelian | - |
| Lumbar | - |
| Traumatic | - |
Others: Hiatus, obturator, perineal, diaphragmatic (Bochdalek/Morgagni)
6. INGUINAL HERNIA
Most common hernia. ~10x more common in men than women.
Anatomy of the Inguinal Canal
- Deep inguinal ring: defect in transversalis fascia, located midway between ASIS and pubic tubercle (~2-3 cm above and lateral to femoral artery pulse)
- Inferior epigastric vessels lie just medial to the deep ring - this is the key anatomical landmark
- Conjoint tendon: fused transversus abdominis + internal oblique, arches over the ring
- Superficial inguinal ring: inverted V-shaped defect in external oblique aponeurosis
Direct vs. Indirect Inguinal Hernia
| Feature | Indirect (Lateral/Oblique) | Direct (Medial) |
|---|---|---|
| Site of origin | Through deep inguinal ring (lateral to inferior epigastric vessels) | Through posterior wall of canal (medial to inferior epigastric vessels) |
| Cause | Congenital - patent processus vaginalis | Acquired - weakness of transversalis fascia |
| Relation to Hesselbach's triangle | Outside | Inside |
| Descent into scrotum | Yes, common | Rarely |
| Age | Any; often young | Middle-aged to elderly |
| Strangulation risk | Higher (narrow neck) | Lower |
| Impulse on cough | Lateral (controlled at deep ring) | Diffuse bulge |
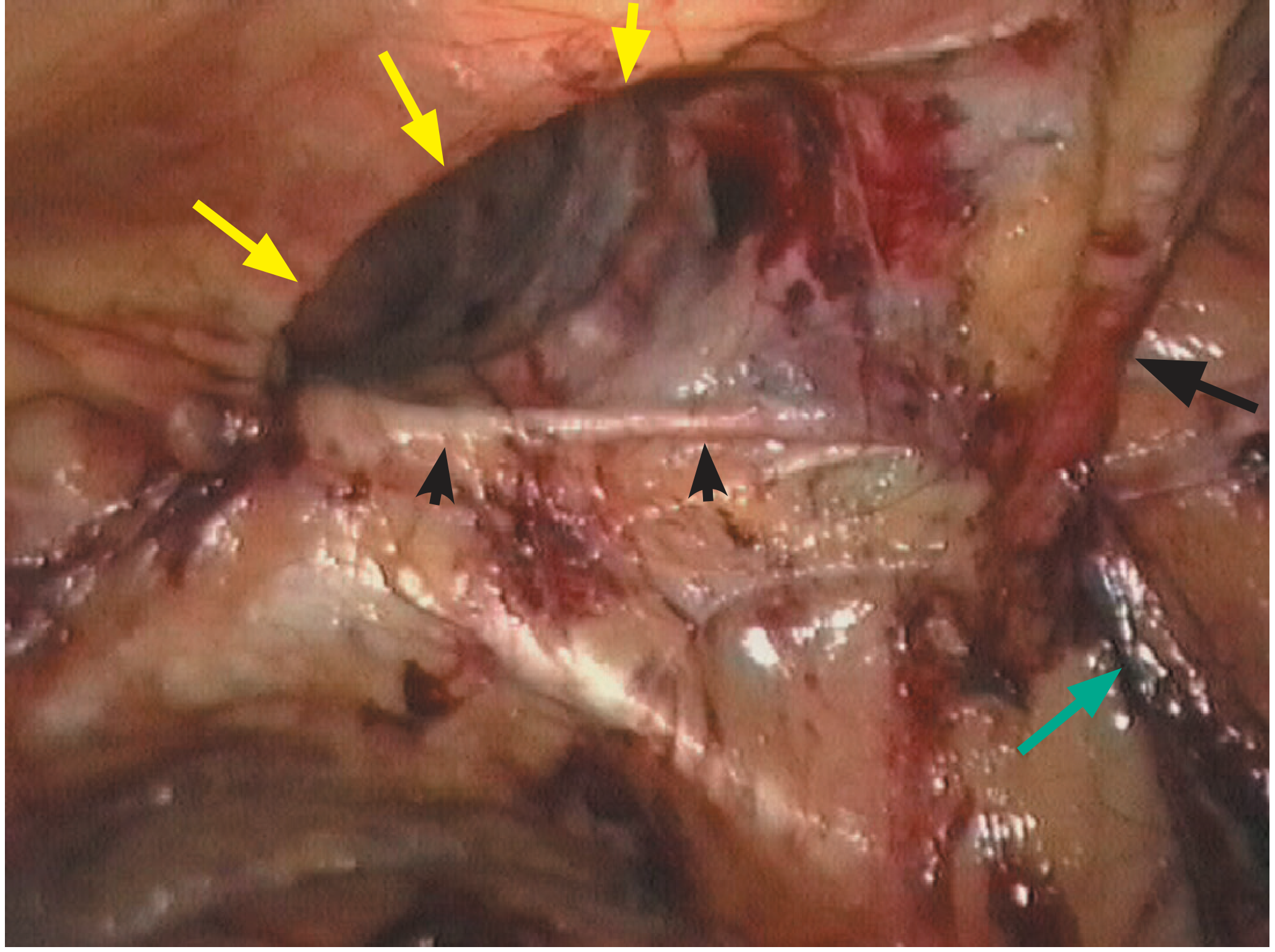
Laparoscopic view of right direct inguinal hernia defect (yellow arrows) above the inguinal ligament - inferior epigastric vessels visible medially:
Diagnosis of Inguinal Hernia
- Usually clinical
- Digital examination: finger in inguinal canal - cough impulse at fingertip = indirect; impulse on dorsum of finger = direct
- Imaging (US, CT, MRI) reserved for ambiguous/occult cases
- Differential: lymph node, hydrocele, varicocele, femoral vessel aneurysm, lipoma, psoas abscess, testicular tumor
Surgical Repair Options
Open Suture Repairs (no mesh)
- Bassini's repair (1890): Sutures between conjoint tendon (above) and inguinal ligament (below), from pubic tubercle to deep ring. Standard for >100 years.
- Shouldice repair: Transversalis fascia opened, then double-breasted closure creates two-layer posterior wall. <2% lifetime failure in expert centres; technically demanding.
- Maloney repair (modified Bassini): Continuous non-absorbable (nylon/polypropylene) darn. Most common in resource-limited settings.
- Desarda repair: Strip of external oblique aponeurosis left attached medially/laterally, sutured to reinforce posterior wall - equivalent to Shouldice.
Open Mesh Repairs
- Lichtenstein tension-free mesh repair (1984): Flat polypropylene mesh (~8x15 cm) placed over the posterior wall behind the cord, slit around the cord at the deep ring. Most common operation for inguinal hernia in resource-rich countries. Lower recurrence but chronic pain reported in up to 20% is a major concern.
- Mesh plug/device: Shaped plugs - risk of meshoma, migration, erosion into bladder. Not recommended by 2018 European Hernia Society guidelines.
- Open preperitoneal (Stoppa): Mesh placed behind transversalis fascia via midline incision. Useful for recurrent hernia. Now largely superseded by TEP.
Laparoscopic Repairs
- TEP (Totally ExtraPeritoneal): Balloon dissection creates preperitoneal space; mesh (~10x15 cm) placed without entering the peritoneal cavity.
- TAPP (TransAbdominal PrePeritoneal): Peritoneal cavity entered, peritoneum incised, mesh placed preperitoneally.
- Both show lower rates of chronic pain and faster return to work than Lichtenstein. Preferred for bilateral and recurrent hernias.
- Robot-assisted laparoscopic repair is an emerging approach with similar outcomes.
7. FEMORAL HERNIA
Anatomy
The femoral canal is the space just medial to the femoral vein, bounded by:
- Laterally: Femoral vein
- Anteriorly: Inguinal ligament
- Posteriorly: Iliopectineal (Astley Cooper's) ligament
- Medially: Lacunar (Gimbernat's) ligament - this sharp, unyielding curved edge impedes reduction
Key Features
- Less common than inguinal hernia
- More common in women (wider femoral canal due to female pelvis shape)
- Appears below and lateral to the pubic tubercle (vs. inguinal hernia which is above and medial)
- Diagnostic error is common
- 50% present as emergencies with very high risk of strangulation - the rigid bony/ligamentous boundaries trap the content
Repair
Three approaches: femoral (low), inguinal (high), and preperitoneal. Emergency repair is mandatory. In strangulated cases, the lacunar ligament must be divided carefully (cavernous vessels lie on its medial side).
8. VENTRAL HERNIAS
Umbilical Hernia
- Children: Occurs in ~10% of infants. 95% resolve spontaneously by age 2. Conservative management recommended under age 2 years. Surgery if persists beyond age 2. (Strangulation extremely rare under age 3)
- Adults: Re-opening of umbilical ring; associated with obesity, ascites, multiple pregnancies. Repair with suture or mesh depending on size.
- Surgery: Small curved infra-umbilical incision; sac identified, reduced, and closed; defect closed with interrupted slowly-absorbable sutures.
Epigastric Hernia
- Protrusion of extraperitoneal fat (and sometimes peritoneum) through defects in the linea alba between the xiphoid process and umbilicus
- Often multiple, frequently asymptomatic. May cause epigastric pain (entrapped fat)
- Treated surgically; suture repair for small defects
Spigelian Hernia
- Protrudes through the spigelian fascia (aponeurosis of transversus abdominis) at the lateral border of the rectus at the semilunar line
- Often interparietal/interstitial - no visible lump; presents with pain and high risk of strangulation
- Diagnosis often requires CT or US; treated surgically
Lumbar Hernia
- Protrudes through the lumbar triangles:
- Superior lumbar triangle (Grynfeltt): Bounded by 12th rib, internal oblique, and sacrospinalis
- Inferior lumbar triangle (Petit's): Bounded by iliac crest, latissimus dorsi, external oblique
- Rare; may be congenital or acquired (post-surgery/trauma)
Incisional Hernia
- Occurs in >10% of laparotomies; laparoscopic port sites ~1%
- Risk factors: wound infection, obesity, steroids, poor technique, excessive tension, diabetes
- May be large and complex, requiring mesh repair
- Often managed with component separation techniques or bridging mesh for giant hernias
Parastomal Hernia
- Hernia through the abdominal wall around a stoma (colostomy/ileostomy) site
- Very common; most do not require repair unless symptomatic or causing stoma dysfunction
9. Other Important Hernias
Hiatus Hernia
- Type I (Sliding): Gastro-oesophageal junction slides into the thorax through the oesophageal hiatus. Most common (~95%). Associated with GERD.
- Type II (Rolling/Para-oesophageal): Fundus rolls up into thorax while GEJ remains in normal position. Risk of gastric volvulus, strangulation.
- Type III: Mixed (both GEJ and fundus herniate)
- Type IV: Other organs (colon, spleen, small bowel) also herniate
Obturator Hernia
- Through the obturator foramen in elderly, multiparous, thin women
- Classic sign: Howship-Romberg sign - medial thigh pain aggravated by hip extension/abduction/internal rotation
- Usually presents as small bowel obstruction; preoperative diagnosis rare
Perineal Hernia
- Protrudes through the floor of the pelvis; usually post-abdominoperineal resection or pelvic floor weakness
Diaphragmatic Hernias
- Bochdalek: Posterior (pleuroperitoneal canal); commonest congenital diaphragmatic hernia; bowel herniates into left chest; presents at birth with respiratory distress
- Morgagni: Anterior (through foramen of Morgagni); usually asymptomatic, discovered incidentally
10. Complications of Hernia Repair
(Source: Schwartz's Principles of Surgery)
- Recurrence: Most common long-term complication. Rates: Bassini ~5-10%, Lichtenstein <1-2%, Shouldice <2% in expert centres, TEP/TAPP ~1%
- Chronic pain/neuralgia: Up to 20% with open mesh (ilioinguinal, iliohypogastric, genitofemoral nerve injury/entrapment)
- Wound infection/seroma: Fluid collection in the hernia sac remnant
- Injury to vas deferens / testicular atrophy: Rare; risk with recurrent surgery
- Mesh complications: Infection, migration (meshoma), erosion into bowel/bladder
- Urinary retention: Especially post-inguinal/femoral repair in elderly males
- Haematoma: Inguinal/scrotal blood collection
11. Key Surgical Mnemonics
Complications of strangulated hernia:
NAILS - Necrosis, Abscess, Intestinal obstruction, Leak/fistula, Systemic sepsis
Boundaries of femoral canal:
NAIL - Nerve (femoral, lateral), Artery, vein (Inside the sheath), Lymphatics (medially = canal content)
Structures at deep inguinal ring (from lateral to medial):
"My Precious Darling Dear" - Muscle of transversalis, Peritoneal sac, Ductus deferens, Deferent artery
Bailey and Love's Short Practice of Surgery 28th Edition, p. 1080-1110 | Schwartz's Principles of Surgery 11th Edition, p. 37
Generate a surgical reference quick-guide for hernia complications and management
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.