Malignant malanoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"melanoma"[MeSH Terms] AND ("treatment" OR "management")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content. Let me compile the full answer.
Malignant Melanoma
Malignant melanoma is the most dangerous form of skin cancer, arising from melanocytes - the pigment-producing cells at the dermoepidermal junction (DEJ). Although it represents only ~1% of skin cancers, it accounts for the majority of skin cancer deaths due to its high metastatic potential.
Epidemiology & Risk Factors
The incidence of melanoma has been rising steadily in light-skinned populations. Key risk factors include:
Phenotypic/Constitutional:
- Light complexion, blue/green eyes, blond or red hair
- Tendency to sunburn easily and tan poorly
- Heavy freckling
- Blistering sunburns in childhood
- Immunosuppression (increases risk 20-30-fold)
- Male gender (associated with thicker tumors at diagnosis)
Acquired/Environmental:
- Excessive UV radiation (solar or tanning salon)
- High number of common or dysplastic nevi (>50)
- Giant congenital nevi
- Prior history of melanoma or family history
- PUVA therapy, xeroderma pigmentosum, burn scars
Molecular Genetics:
- BRAF V600E mutations - present in 50-60% of cutaneous melanomas, especially on non-chronically sun-exposed skin in Caucasians
- KIT gene mutations and cyclin D1/CDK4 amplifications - associated with acral and mucosal lentiginous melanomas
- p16/CDKN2A mutations - potent risk factor; familial forms
Acral lesions account for a disproportionate share of melanomas in darker-skinned individuals. The lowest overall incidence is in Asians.
Pathogenesis & Growth Phases
Melanomas arise predominantly from melanocytes at the DEJ. About 10-20% develop in pre-existing nevi; the rest arise de novo on previously normal skin.
There are two distinct growth phases:
- Radial (horizontal) growth phase - cells spread laterally along the DEJ with little dermal invasion; low metastatic potential
- Vertical growth phase - invasion into the dermis; metastatic potential increases substantially with depth
The single greatest risk factor for metastasis is depth of invasion (Breslow thickness).
Clinical Types
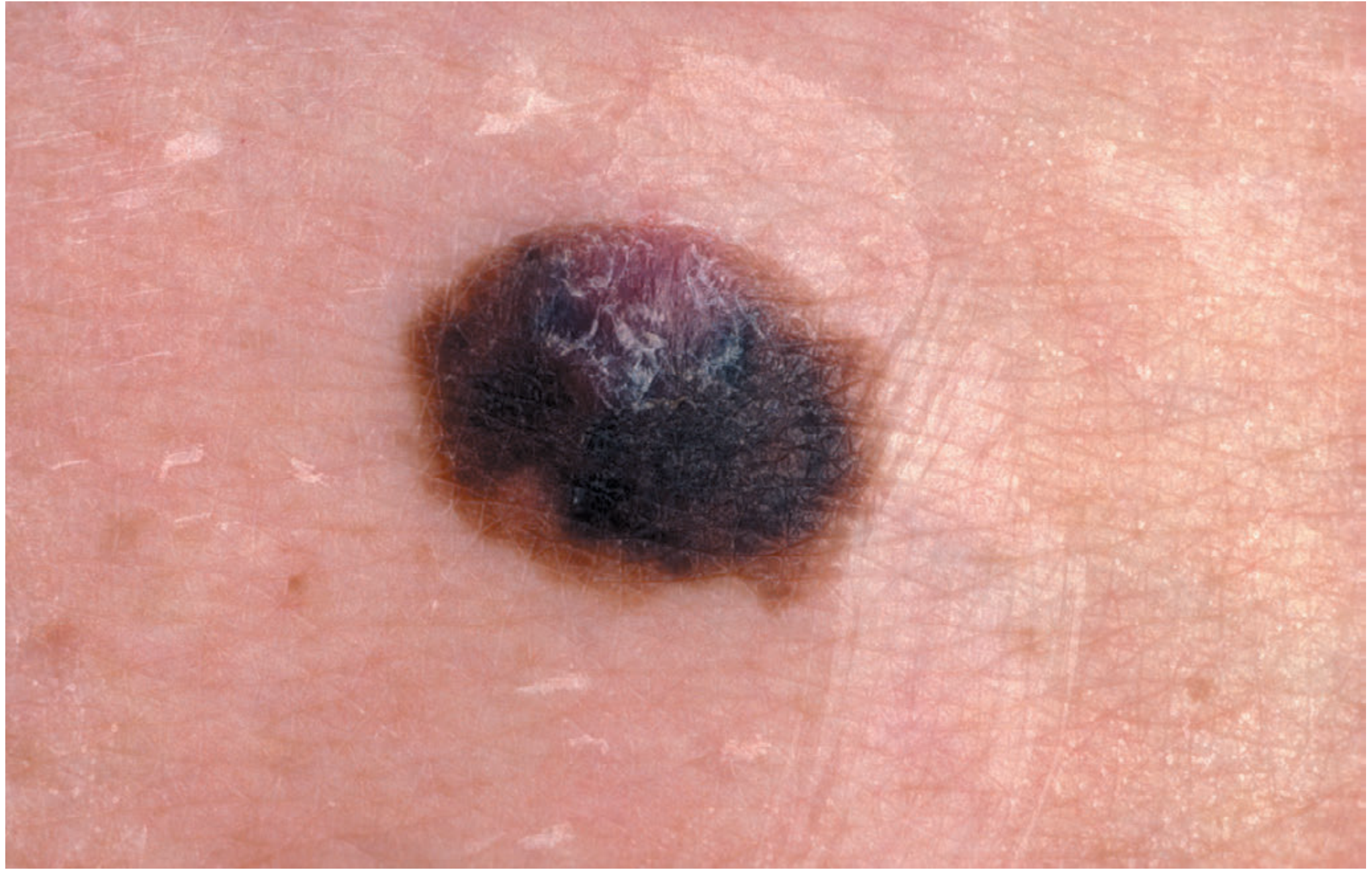
1. Superficial Spreading Melanoma (SSM) - Most Common (70%)
Usually arises in a pre-existing nevus after years of slow change, followed by rapid growth. Nodularity within SSM heralds the vertical growth phase.
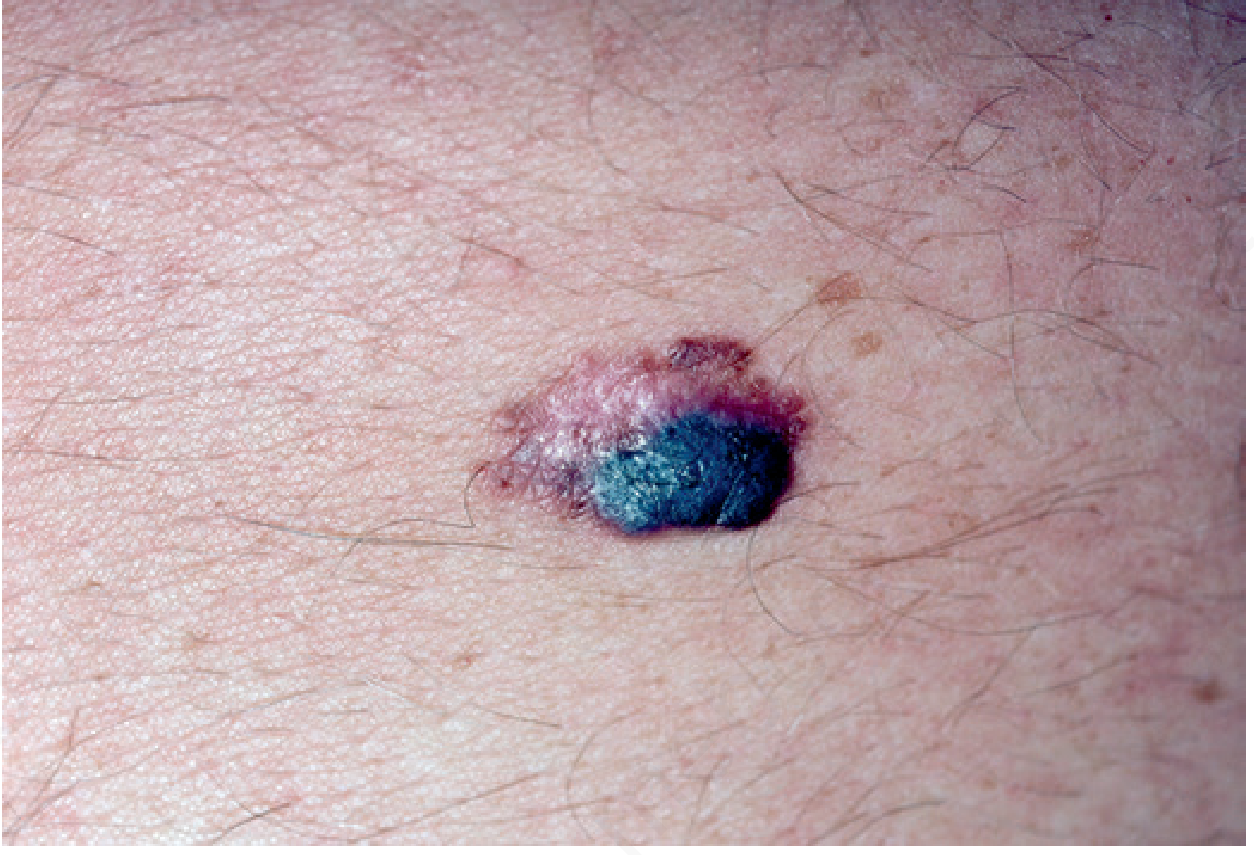
2. Nodular Melanoma (NM) - 15%
More aggressive; shorter clinical onset; often arises de novo. Typically a blue/black papule 1-2 cm on the trunk, head, or neck in middle-aged men. Lacks a horizontal growth phase, so it tends to be sharply demarcated. Up to 5% are amelanotic.
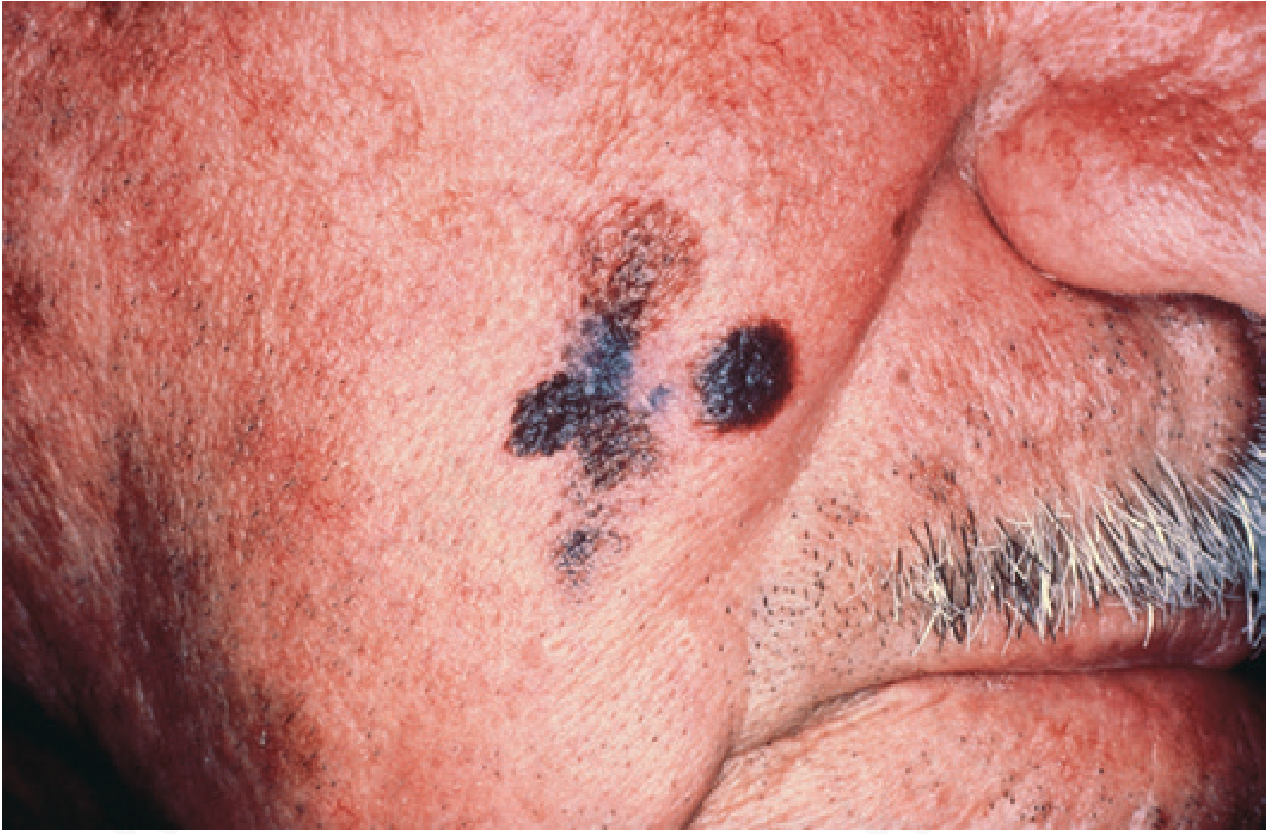
3. Lentigo Maligna Melanoma (LMM) - 5-10%
Also called Hutchinson's melanotic freckle. Slow-growing, variegated brown macule on the face, neck, or hands of the elderly. Correlates with prolonged sun exposure; more common in women. Has a long radial growth phase (5-20 years) before vertical invasion. Once it invades, metastatic potential equals other variants.
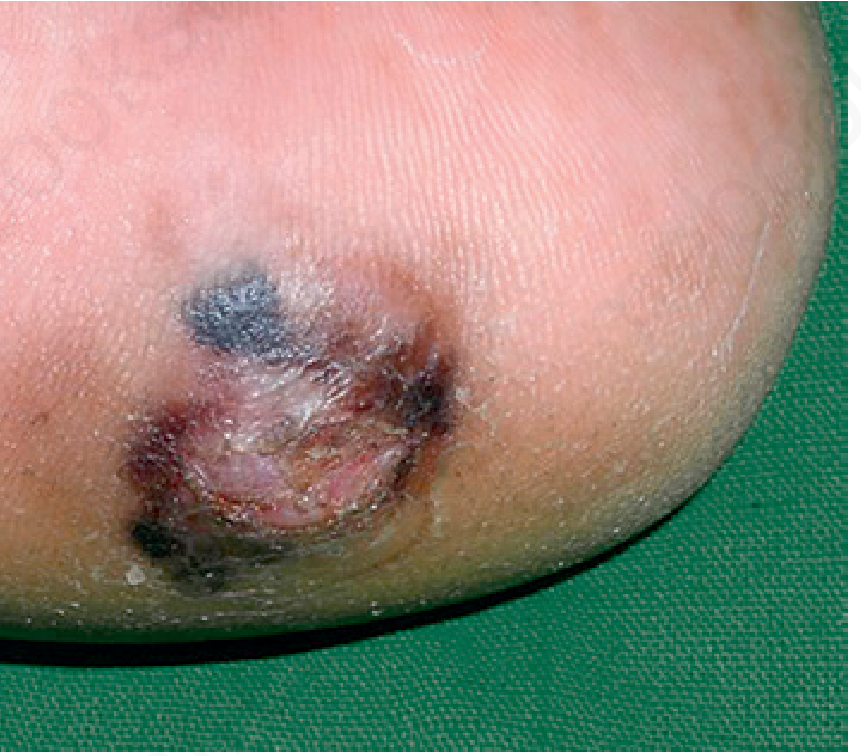
4. Acral Lentiginous Melanoma (ALM) - 2-8% in whites; 35-60% in Afro-Caribbean/Hispanic/Asian
Affects soles and palms. Presents as a flat, irregular macule in later life. 25% are amelanotic (may mimic fungal infection or pyogenic granuloma). Associated with KIT mutations and cyclin D1 amplifications.
Other Subtypes
- Desmoplastic melanoma - head/neck; propensity for perineural infiltration; often amelanotic; high local recurrence if not widely excised
- Mucosal melanoma - rare; arises from mucosal melanocytes; head and neck (15-20%) and anogenital region
- Uveal (ocular) melanoma - most common primary intraocular malignancy in adults; arises in uveal tract; metastasizes predominantly to liver
- Conjunctival melanoma - arises from primary acquired melanosis; early metastasis possible even at small tumor size
Clinical Recognition: The ABCDE Criteria
| Letter | Feature |
|---|---|
| A | Asymmetry |
| B | Border irregularity |
| C | Color variegation |
| D | Diameter >6 mm |
| E | Evolution (change over time) |
Additional warning signs in pre-existing nevi: change in size, shape, color, thickness (elevation/ulceration), satellite lesions, tingling/itching/serosanguineous discharge.
Dermoscopy (epiluminescence microscopy) makes subsurface structures visible and, in experienced hands, improves diagnostic accuracy.
Diagnosis & Biopsy
- Excision biopsy with 2-3 mm margin of skin and subdermal fat is the standard
- Incision biopsy is acceptable for large facial lesions where full excision would be disfiguring
- Pathological examination provides Breslow thickness - measured to the nearest 0.1 mm from the granular layer to the base of the tumor
- Sentinel node biopsy (SNB) is used for staging regional lymph node involvement
AJCC Staging (T Classification)
| Stage | Thickness | Notes |
|---|---|---|
| Tis | In situ | Confined to epidermis |
| T1a | <0.8 mm | No ulceration |
| T1b | <0.8 mm with ulceration, OR 0.8-1.0 mm | |
| T2a | 1.01-2.0 mm | No ulceration |
| T2b | 1.01-2.0 mm | With ulceration |
| T3a | 2.01-4.0 mm | No ulceration |
| T3b | 2.01-4.0 mm | With ulceration |
| T4a | >4.0 mm | No ulceration |
| T4b | >4.0 mm | With ulceration |
Breslow thickness is the most important prognostic indicator in the absence of lymph node metastases. Ulceration upstages the tumor.
Treatment
Surgery
- Wide local excision with margins determined by Breslow thickness
- Sentinel lymph node biopsy for staging
Adjuvant Therapy (High-Risk Resected Disease)
For nearly 25 years, high-dose interferon-alfa (IFN-alpha) was the only adjuvant option. This has now been replaced by:
- Immune checkpoint inhibitors: nivolumab, pembrolizumab (anti-PD-1), ipilimumab (anti-CTLA-4) - approved as single agents
- Targeted therapy (BRAF V600E/K mutant + lymph node involvement): dabrafenib + trametinib combination
Metastatic Disease
Immunotherapy:
- Ipilimumab (anti-CTLA-4): enhances T-cell activation/proliferation; approved for metastatic melanoma
- Nivolumab and pembrolizumab (anti-PD-1 IgG4 antibodies): block PD-L1/PD-L2 interaction, restoring T-cell anti-tumor response; approved as monotherapy
- Nivolumab + ipilimumab combination: approved for unresectable/metastatic melanoma
- High-dose IL-2: can produce durable responses in a small subset
BRAF-targeted therapy (for BRAF V600E/V600K mutant tumors ~50-60%):
- BRAF inhibitors: vemurafenib, dabrafenib, encorafenib
- MEK inhibitors (combined with BRAF inhibitors): trametinib, cobimetinib, binimetinib
- Combination BRAF + MEK inhibition is the preferred approach
Cytotoxic agents (now rarely used): dacarbazine, temozolomide, cisplatin - historically the backbone but low response rates
Uveal melanoma metastases: tebentafusp (bispecific T-cell engager targeting gp100 via a TCR-anti-CD3 fusion) prolongs survival
Prognosis
- Breslow thickness remains the key prognostic factor
- Patients with distant metastases have approximately 40% 5-year survival
- Uveal melanoma: survival as low as 50% at 15 years for large lesions; most metastases go to liver
- Conjunctival melanoma has worse prognosis than cutaneous forms due to early metastasis at small tumor size
Special Situations
Pregnancy: Nevi may uniformly darken due to estrogen/progesterone receptor changes. Any irregular pigmentation or asymmetric growth warrants biopsy. Women who develop melanoma during pregnancy have a shorter disease-free interval but no adverse overall survival effect.
Pediatric melanoma: Rare; occurs >50% of the time from previously normal skin. Recognition often delayed. May develop within giant congenital nevi.
Sources:
- Andrews' Diseases of the Skin: Clinical Dermatology, Ch. 30
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 45
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Ch. 11
- Goldman-Cecil Medicine, International Ed., Ch. 391
Recent evidence note (2026): A 2026 meta-analysis (PMID 41478279) identified immune signatures that can potentially uncouple checkpoint inhibitor efficacy from toxicity in melanoma - a potentially important development for personalizing immunotherapy selection.
This is a shared conversation. Sign in to Orris to start your own chat.