Explain Heparin according to kdt and shanbhag
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed to write a thorough, well-structured answer on Heparin as covered in standard Indian pharmacology textbooks (KDT/Shanbhag style). Let me note upfront that the library does not have the exact KDT (Tripathi) or Shanbhag books, but I have their content covered through Katzung and Lippincott Pharmacology, which follow the same curriculum framework. I'll present this in the KDT/Shanbhag teaching format.
Heparin - As per KDT & Shanbhag
Note: The library does not contain the KDT (Tripathi's Essentials of Medical Pharmacology) or Shanbhag textbooks directly. The following is compiled from Katzung's Basic & Clinical Pharmacology (16th ed.) and Lippincott Illustrated Reviews: Pharmacology - both of which cover the same content in the standard format used by KDT and Shanbhag for Indian pharmacology teaching.
1. Introduction
Heparin is a naturally occurring, rapidly acting parenteral anticoagulant. It occurs in mast cells complexed with histamine, though its physiologic role there is unknown. Commercially, it is extracted from porcine intestinal mucosa or bovine lung.
2. Chemistry
- Heparin is a heterogeneous mixture of sulfated mucopolysaccharides (glycosaminoglycans)
- It is strongly acidic due to sulfate and carboxylic acid groups
- Molecular weight range: 5,000-30,000 Da (unfractionated heparin, UFH)
- Contains repeating sulfated disaccharide units of D-glucosamine - D-iduronic acid and D-glucosamine - D-glucuronic acid
- Only ~1/3 of commercial heparin molecules have anticoagulant activity - those possessing the unique pentasaccharide sequence required for high-affinity antithrombin binding
Low-Molecular-Weight Heparins (LMWHs): Produced by depolymerization of UFH. Examples: enoxaparin, dalteparin, tinzaparin. MW ~1/3 that of UFH.
3. Mechanism of Action
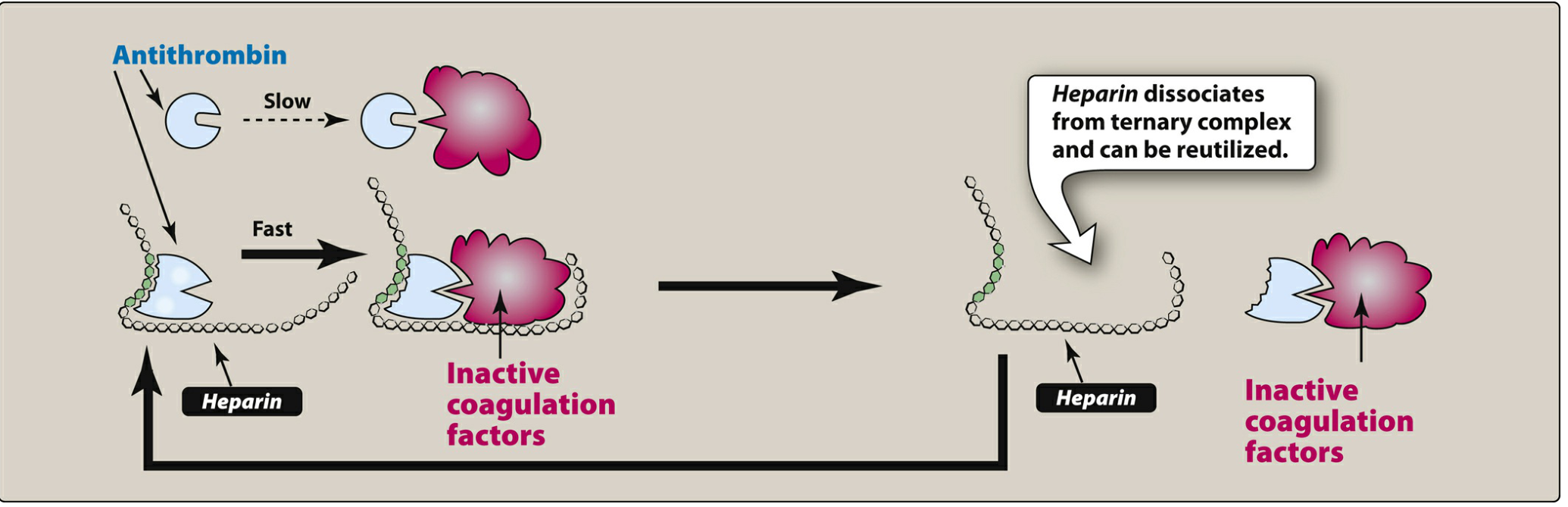
Figure: Heparin acts as a cofactor - it binds antithrombin, triggers a conformational change, and greatly accelerates inactivation of coagulation factors. Heparin is then released intact for reuse.
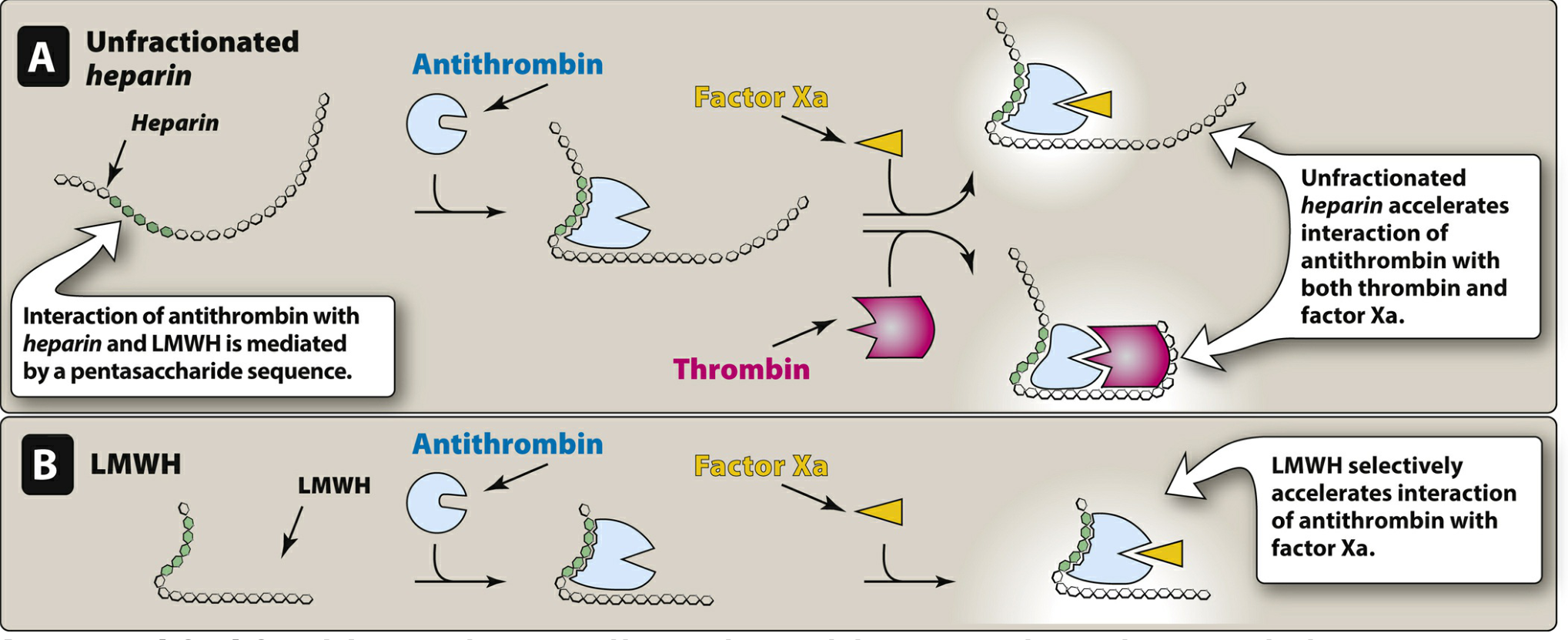
Figure: (A) UFH accelerates antithrombin inactivation of both thrombin AND Factor Xa. (B) LMWH selectively accelerates inactivation of Factor Xa only.
Step-by-step mechanism:
- Antithrombin III (AT-III) is an alpha-globulin that slowly inhibits serine proteases - thrombin (IIa), factor IXa, and factor Xa
- Heparin binds to AT-III via its unique pentasaccharide sequence, causing a conformational change in AT-III
- This change exposes AT-III's active site, accelerating inactivation of clotting factors by 1000-fold
- Once the AT-III-protease complex forms, heparin is released intact and acts as a true catalytic cofactor (not consumed)
- UFH inhibits thrombin (IIa), IXa, and Xa (requires chain long enough to bridge AT-III and thrombin simultaneously)
- LMWH inhibits factor Xa selectively - the short chain can bind AT-III but cannot simultaneously bridge thrombin
Key point: Heparin does not dissolve existing clots - it prevents new clot formation and extension of existing thrombi.
4. Pharmacokinetics
| Feature | UFH | LMWH |
|---|---|---|
| Route | IV or SC (not IM) | SC (enoxaparin also IV in MI) |
| Onset | Within minutes (IV) | 1-2 hrs (SC) |
| Half-life | ~1.5 hours | 3-12 hours |
| Monitoring | aPTT (intrinsic pathway) | Usually not required |
| Protein binding | Extensive, variable, unpredictable | More predictable |
| Elimination | Monocyte/macrophage uptake + renal excretion | Primarily renal |
| Renal failure | Dose-dependent; use cautiously | Dose reduction required (accumulates) |
| Bioavailability (SC) | ~30% (variable) | ~90% (predictable) |
- aPTT therapeutic target for UFH: 1.5-2.5x control (institution specific)
- UFH plasma level: 0.2-0.4 unit/mL (protamine titration) or 0.3-0.7 unit/mL (anti-Xa)
- LMWH anti-Xa monitoring required in: obesity, renal impairment, pregnancy
5. Uses / Indications
- Deep Vein Thrombosis (DVT) - treatment and prophylaxis
- Pulmonary Embolism (PE) - acute treatment
- Acute Coronary Syndromes (STEMI, NSTEMI, unstable angina) - including during percutaneous coronary intervention (PCI)
- Prophylaxis of postoperative venous thrombosis - e.g., hip/knee replacement surgeries
- Arterial thromboembolism - prevention and treatment
- Cardiac and arterial surgery - maintaining patency of circuits
- Anticoagulant of choice in pregnancy - does not cross the placenta due to large size and negative charge
- Hemodialysis - prevention of clotting in extracorporeal circuits
- Peripheral arterial occlusion - thromboembolic events
- Bridging anticoagulation - when transitioning to/from warfarin
6. Adverse Effects
6.1 Bleeding (Most Common)
- The major adverse effect of heparin
- Risk factors: elderly women, renal failure, high doses, prolonged therapy
- Management: discontinue heparin; protamine sulfate for reversal
6.2 Heparin-Induced Thrombocytopenia (HIT)
- Immune-mediated reaction
- Type I (non-immune): mild, transient thrombocytopenia in first 1-2 days, benign
- Type II (immune): occurs 5-10 days after starting heparin; antibodies against heparin-PF4 complex form, activating platelets
- Paradoxically causes thrombosis (venous and arterial), not just bleeding
- Platelet count must be monitored frequently
- Management: Stop heparin immediately; switch to argatroban (direct thrombin inhibitor) or other non-heparin anticoagulant
- LMWHs are not recommended in HIT (cross-sensitivity possible)
6.3 Osteoporosis
- With long-term use (>3 months), especially in pregnancy
- More common with UFH than LMWH
6.4 Hypersensitivity Reactions
- Heparin is derived from porcine sources - antigenic
- Reactions: chills, fever, urticaria, anaphylactic shock
6.5 Hypoaldosteronism
- Rare; heparin suppresses aldosterone synthesis - may cause hyperkalemia
7. Contraindications
- Active bleeding or high bleeding risk
- Severe thrombocytopenia
- History of HIT
- Hypersensitivity to heparin
- Intracranial hemorrhage
- Uncontrolled hypertension
- Patients undergoing spinal/epidural anesthesia (increased risk of spinal hematoma)
8. Drug Interactions
- Aspirin, NSAIDs, antiplatelet drugs: Increased bleeding risk
- Warfarin: Additive anticoagulation
- Protamine sulfate: Antidote - directly antagonizes heparin
- Drugs that decrease heparin effect: digitalis, tetracyclines, antihistamines, nicotine
9. Antidote - Protamine Sulfate
- A basic protein derived from fish sperm/testes, rich in arginine
- The positively charged protamine forms a stable 1:1 ionic complex with negatively charged heparin, inactivating it
- Dose: 1 mg protamine neutralizes 100 units of heparin
- Given by slow IV infusion (rapid infusion causes hypotension, bradycardia)
- Excess protamine itself acts as a weak anticoagulant - avoid overdosage
- Protamine has incomplete neutralization of LMWH anti-Xa activity (~60%)
10. UFH vs LMWH - Comparison
| Feature | UFH | LMWH (e.g., Enoxaparin) |
|---|---|---|
| MW | 5,000-30,000 Da | 1,000-10,000 Da |
| Anti-Xa : Anti-IIa | 1:1 | 4:1 (Xa selective) |
| SC bioavailability | ~30% | ~90% |
| Plasma t½ | ~1.5 hr | 3-12 hr |
| Monitoring | aPTT needed | Not usually required |
| Dosing | Weight-based, frequent | Once or twice daily |
| Reversal | Fully reversed by protamine | Partially reversed |
| Renal failure | Safer (hepatic clearance) | Use with caution |
| HIT risk | Higher | Lower (but cross-reaction possible) |
| Osteoporosis | More likely | Less likely |
| Cost | Cheaper | More expensive |
| Preferred in pregnancy | Both used; UFH traditionally preferred | LMWH now preferred |
11. Preparations and Doses
UFH:
- IV bolus: 5,000 units, followed by continuous infusion of 1,000-1,500 units/hour (titrated to aPTT)
- SC (prophylaxis): 5,000 units every 8-12 hours
- Available as: Heparin sodium injection 1,000, 5,000, 10,000, 25,000 units/mL
LMWH (Enoxaparin - most common):
- DVT prophylaxis: 40 mg SC once daily
- DVT/PE treatment: 1 mg/kg SC every 12 hours (or 1.5 mg/kg SC once daily)
- ACS: 1 mg/kg SC every 12 hours
Summary Points (High-Yield for Exams)
| Point | Detail |
|---|---|
| Class | Sulfated mucopolysaccharide, indirect anticoagulant |
| Mechanism | Potentiates AT-III → inactivates IIa, IXa, Xa (x1000) |
| Route | Only parenteral (IV/SC) - not oral, not IM |
| Monitor | aPTT (UFH); anti-Xa (LMWH in special cases) |
| Antidote | Protamine sulfate (1 mg/100 units) |
| Safe in pregnancy | Yes - does not cross placenta |
| Dreaded complication | HIT Type II (thrombocytopenia + thrombosis) |
| Treatment of HIT | Stop heparin; start argatroban |
| Long-term risk | Osteoporosis |
| Not effective orally | Large size, negative charge - not absorbed |
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 959-961; Lippincott Illustrated Reviews: Pharmacology, pp. 451-455
Warfarin according to shanbhag
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed. Here is the complete Shanbhag-style presentation of Warfarin:
Warfarin - As per Shanbhag (& KDT Style)
Note: The library does not contain the Shanbhag pharmacology textbook directly. The following is compiled and presented in the Shanbhag/KDT teaching format using Lippincott Illustrated Reviews: Pharmacology and Katzung's Basic & Clinical Pharmacology (16th ed.) - both follow the same Indian pharmacology curriculum framework.
1. Introduction
Warfarin is an oral anticoagulant belonging to the coumarin group (4-hydroxycoumarin derivatives). It is an indirect, slow-acting anticoagulant that acts by antagonizing vitamin K. Named after the Wisconsin Alumni Research Foundation (WARF), it is one of the most widely used anticoagulants globally and is the standard oral anticoagulant in the Indian pharmacology curriculum.
Other coumarins: acenocoumarol (nicoumalone), phenprocoumon, dicoumarol.
2. Chemistry
- Warfarin is a racemic mixture of R- and S-enantiomers
- S-warfarin is 3-5x more potent than R-warfarin
- Both are metabolized by CYP450 (S by CYP2C9, R by CYP1A2 and CYP3A4)
- Structural analog of vitamin K - this is the basis of competitive antagonism
3. Mechanism of Action
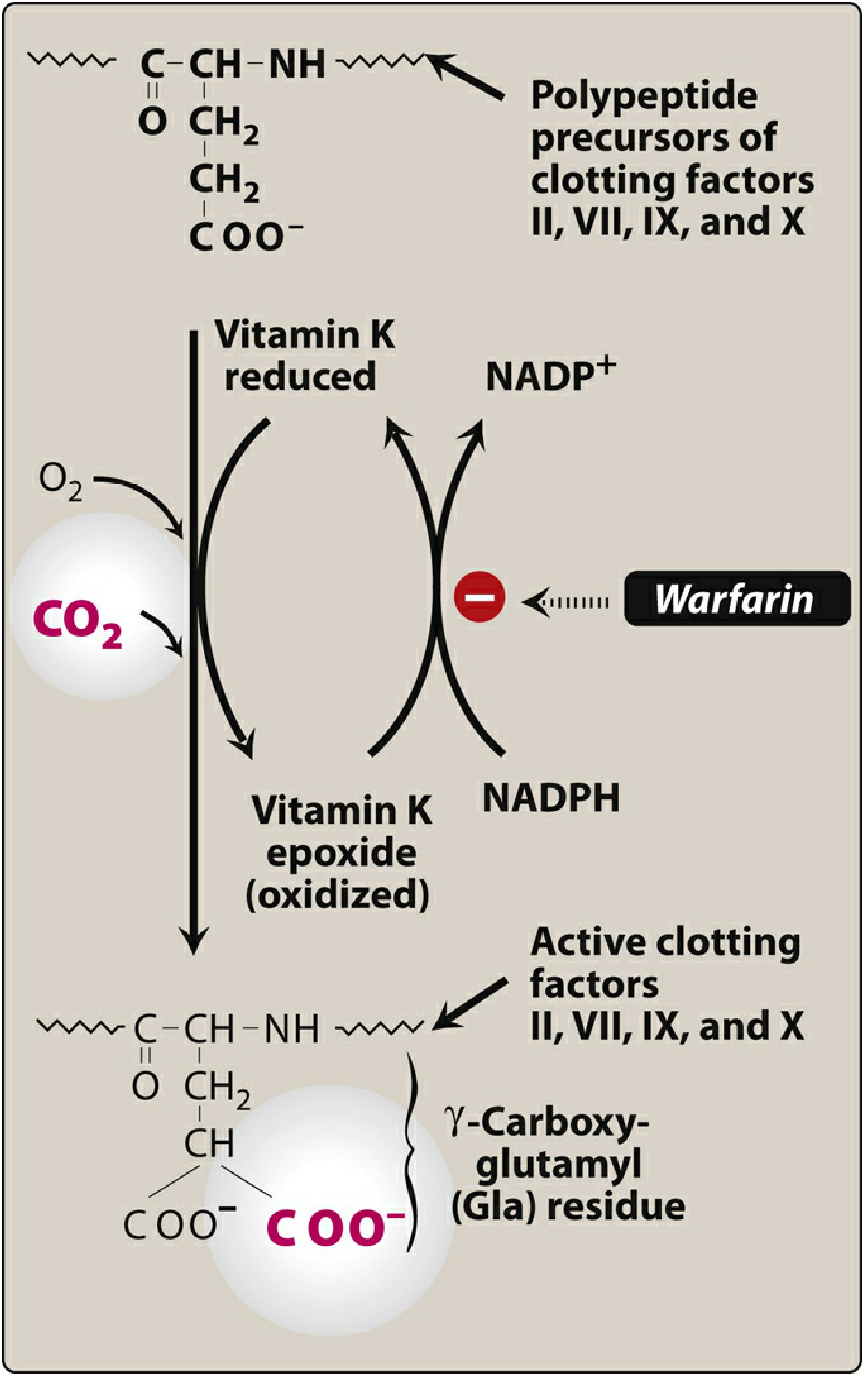
Figure: Warfarin blocks vitamin K epoxide reductase (VKORC1), trapping vitamin K in its inactive epoxide form. This prevents gamma-carboxylation of clotting factor precursors, producing biologically inactive factors.
Step-by-step:
- Clotting factors II, VII, IX, X (and anticoagulant proteins C and S) require vitamin K as a cofactor for their synthesis in the liver
- During synthesis, vitamin K-dependent carboxylase converts glutamic acid (Glu) residues to gamma-carboxyglutamic acid (Gla) residues on these factors
- Gla residues are essential - they bind Ca²+ ions, which allows the factors to bind to platelet membranes and become active
- During this carboxylation, vitamin K is oxidized to vitamin K epoxide (inactive)
- Vitamin K epoxide reductase (VKORC1) normally regenerates active (reduced) vitamin K from the epoxide
- Warfarin inhibits VKORC1 - trapping vitamin K in the epoxide form → no regeneration of active vitamin K
- Result: clotting factors produced are incomplete (10-40% activity), with deficient Gla residues - biologically inactive
Factors affected (mnemonic: 1972):
- Factor I (fibrinogen) - NOT affected
- Factors II, VII, IX, X - synthesis inhibited
- Proteins C and S (natural anticoagulants) - also inhibited
4. Why is There a Delay in Action?
- Onset of action is delayed by 8-12 hours (peak effect: 72-96 hours)
- This is because warfarin does NOT destroy already-circulating clotting factors
- It only prevents synthesis of new ones
- The delay equals the time needed to deplete the pool of existing clotting factors
- Half-lives of factors: Factor VII = 6 h (shortest) → Factor II = 60 h (longest)
- Factor VII falls first (shortest t½), so PT/INR rises first
Warfarin Paradox (Important Exam Point!)
- Initially, warfarin also depletes Protein C (t½ ~6 hours, same as factor VII)
- Protein C is a natural anticoagulant
- So early warfarin therapy causes a transient pro-thrombotic (hypercoagulable) state
- This is why heparin must be overlapped with warfarin for 5-7 days when starting warfarin in acute thrombosis
5. Pharmacokinetics
| Feature | Detail |
|---|---|
| Route | Oral (100% bioavailability, well absorbed) |
| Onset | 8-12 hours (peak effect 72-96 hours) |
| Protein binding | ~99% bound to plasma albumin |
| Volume of distribution | Small (restricted to plasma due to high protein binding) |
| Half-life | ~40 hours (highly variable between individuals) |
| Metabolism | Liver - CYP2C9 (S-warfarin), CYP1A2/CYP3A4 (R-warfarin) |
| Excretion | Inactive metabolites in urine and feces (conjugated with glucuronic acid) |
| CSF penetration | Minimal (protein-bound, large) |
| Breast milk | Does NOT significantly pass |
| Placental transfer | Freely crosses placenta - TERATOGENIC |
| Genetic variation | CYP2C9 and VKORC1 polymorphisms affect dosing significantly |
6. Uses / Therapeutic Indications
- Atrial fibrillation - prevention of stroke and systemic embolism
- Prosthetic (mechanical) heart valves - prevention of thromboembolism
- DVT and PE - treatment and secondary prevention
- Post-orthopedic surgery (hip/knee replacement) - VTE prophylaxis
- Protein C or S deficiency - secondary prophylaxis
- Antiphospholipid syndrome - prevention of recurrent thrombosis
- Post-MI - in selected patients with mural thrombus
7. Monitoring
- Prothrombin time (PT) - test of the extrinsic pathway (factors VII, X, V, II, fibrinogen)
- Reported as INR (International Normalized Ratio) - standardized PT ratio
- Normal INR: ~1.0
- Therapeutic INR for most indications: 2.0 - 3.0
- Mechanical heart valves / high thrombotic risk: 2.5 - 3.5
- PT should be checked regularly; more frequently when starting or adjusting dose
Why PT and not aPTT?
Warfarin primarily reduces Factor VII (extrinsic pathway), which is detected by PT. aPTT detects intrinsic pathway (used for heparin monitoring).
8. Dosing
- Starting dose: 5-10 mg/day orally
- Maintenance dose: 2-10 mg/day (individualized; average ~5 mg/day)
- Dose adjusted based on INR
- If PT activity < 20% (INR excessively high): reduce or omit dose
9. Adverse Effects
9.1 Bleeding (Most Common and Serious)
- Can occur at any site - GI tract, urinary tract, intracranial
- Risk increases with higher INR
- Management:
- Minor bleeding: withdraw drug or give oral Vitamin K₁ (phytomenadione)
- Major bleeding: IV Vitamin K₁ + fresh frozen plasma (FFP) / prothrombin complex concentrate (PCC)
- Reversal takes ~24 hours even with Vitamin K (time needed to synthesize new factors)
9.2 Teratogenicity (MOST IMPORTANT)
- Warfarin embryopathy (exposure in 1st trimester, especially weeks 6-12):
- Nasal hypoplasia, stippled epiphyses (chondrodysplasia punctata)
- Abnormal bone formation
- CNS abnormalities (2nd/3rd trimester): dorsal midline dysplasia, Dandy-Walker syndrome
- Fetal hemorrhage
- WARFARIN IS ABSOLUTELY CONTRAINDICATED IN PREGNANCY
- Use heparin or LMWH instead (does not cross placenta)
9.3 Skin Necrosis
- Occurs in first 1-2 weeks of therapy
- Seen in patients with hereditary Protein C deficiency
- Warfarin rapidly depletes Protein C → thrombosis in skin microvasculature → necrosis
- Sites: breast, fatty tissues, buttocks, thighs, intestine
- Prevented by: starting with heparin overlap; using low initial doses
9.4 Purple Toe Syndrome
- Rare complication
- Painful, blue-tinged discoloration of toes
- Caused by cholesterol microemboli from disrupted atherosclerotic plaques
- Paradoxically occurs in patients on warfarin
9.5 Other
- Alopecia (hair loss)
- Skin rashes
- GI disturbances (nausea, diarrhea)
10. Drug Interactions (Highly Tested!)
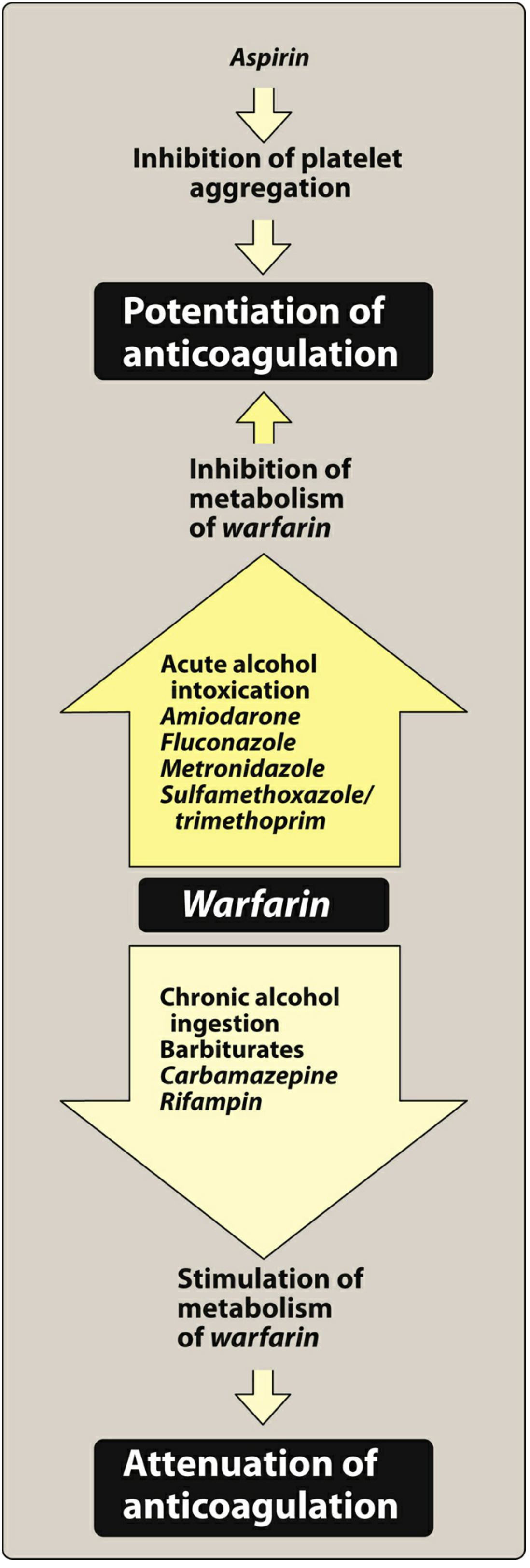
Figure: Drugs that potentiate warfarin (increase INR/bleeding risk) vs. drugs that attenuate warfarin (decrease INR/thrombosis risk)
Drugs that INCREASE warfarin effect (increased bleeding risk):
| Mechanism | Drugs |
|---|---|
| CYP2C9 inhibition (↓ warfarin metabolism) | Amiodarone, fluconazole, metronidazole, co-trimoxazole, acute alcohol, isoniazid, omeprazole |
| Inhibit platelet aggregation (additive) | Aspirin, NSAIDs, clopidogrel |
| ↓ Vitamin K synthesis (gut flora killed) | Broad-spectrum antibiotics |
| ↑ Catabolism of clotting factors | Thyroxine (hyperthyroidism) |
| Displace warfarin from albumin | Sulfonamides, chloral hydrate |
| ↓ Vitamin K absorption | Cholestyramine (at different times), mineral oil |
Drugs that DECREASE warfarin effect (thrombosis risk):
| Mechanism | Drugs |
|---|---|
| CYP2C9 induction (↑ warfarin metabolism) | Rifampicin (most potent), barbiturates, carbamazepine, chronic alcohol, griseofulvin, phenytoin |
| Provide Vitamin K | Green leafy vegetables (spinach, broccoli), vitamin K supplements |
| ↓ Absorption of warfarin | Cholestyramine (if given together) |
Key mnemonics for inducers (reduce warfarin): "BCRG-P" - Barbiturates, Carbamazepine, Rifampicin, Griseofulvin, Phenytoin
11. Contraindications
- Pregnancy (absolute)
- Active bleeding or high bleeding risk
- Severe hepatic disease
- Severe hypertension (risk of hemorrhagic stroke)
- History of warfarin-induced skin necrosis (Protein C deficiency)
- Recent neurosurgery, eye surgery
- Patient non-compliance (critical - requires regular monitoring)
- Hemorrhagic stroke
12. Antidote - Vitamin K₁ (Phytomenadione)
- Mechanism: Provides exogenous vitamin K to overcome the competitive inhibition by warfarin and regenerate active vitamin K for clotting factor synthesis
- Route: Oral (for minor over-anticoagulation) or slow IV infusion (for major bleeding)
- IV is preferred for serious bleeding - acts within 6-12 hours
- Caveat: Reversal takes ~24 hours (time needed to synthesize new clotting factors)
- Too much Vitamin K makes the patient refractory to warfarin for days (if long-term anticoagulation is still needed)
- For immediate reversal (life-threatening bleeding): Fresh Frozen Plasma (FFP) or Prothrombin Complex Concentrate (PCC) + Vitamin K
13. Warfarin vs Heparin - Key Comparison (High-Yield)
| Feature | Warfarin | Heparin |
|---|---|---|
| Class | Coumarin (Vitamin K antagonist) | Sulfated mucopolysaccharide |
| Route | Oral | Parenteral only (IV/SC) |
| Onset | Delayed (8-12 hours; peak 72-96 h) | Immediate (IV) |
| Mechanism | Inhibits Vit K-dependent synthesis of II, VII, IX, X | Potentiates AT-III → inactivates IIa, IXa, Xa |
| Monitor | PT/INR | aPTT |
| Protein binding | 99% (albumin) | Extensive, variable |
| Placental transfer | Yes - teratogenic | No - safe in pregnancy |
| Antidote | Vitamin K₁ (+ FFP/PCC for urgent) | Protamine sulfate |
| Thrombocytopenia | No | Yes (HIT) |
| Osteoporosis | No (long-term) | Yes (UFH > LMWH) |
| Use in pregnancy | Contraindicated | Drug of choice |
| Drug interactions | Extensive (CYP450) | Fewer |
| Therapeutic window | Narrow - requires monitoring | Narrow - requires monitoring |
14. Summary - High-Yield Points for Exams
| Point | Detail |
|---|---|
| Class | Coumarin; oral anticoagulant |
| Mechanism | Inhibits VKORC1 → blocks gamma-carboxylation of factors II, VII, IX, X (and Proteins C & S) |
| Delayed onset | 8-12 h (peak 72-96 h) - depletes existing factors |
| Monitor | INR (therapeutic range 2-3 for most) |
| Antidote | Vitamin K₁ + FFP/PCC |
| CONTRAINDICATED in | Pregnancy (warfarin embryopathy) |
| Skin necrosis | Due to early Protein C depletion |
| Potentiated by | Amiodarone, metronidazole, fluconazole, aspirin, antibiotics |
| Antagonized by | Rifampicin (most potent inducer), barbiturates, carbamazepine |
| Purple toe syndrome | Cholesterol emboli - rare |
| Why bridge with heparin? | Early hypercoagulability due to rapid Protein C depletion |
Sources: Lippincott Illustrated Reviews: Pharmacology, pp. 458-461; Katzung's Basic & Clinical Pharmacology, 16th ed., pp. 962-965
Directly acting oral anticoagulant according to shanbhag
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content on all DOACs. Let me compile the full Shanbhag-style answer.
Directly Acting Oral Anticoagulants (DOACs) - As per Shanbhag Style
Also called NOACs (New/Novel Oral Anticoagulants) or TSOACs (Target-Specific Oral Anticoagulants). The library does not contain the Shanbhag textbook directly; this is presented in the standard Shanbhag/KDT Indian pharmacology curriculum format using Lippincott Illustrated Reviews: Pharmacology and Katzung's Basic & Clinical Pharmacology (16th ed.).
1. Introduction
DOACs are a newer class of oral anticoagulants that directly inhibit specific activated clotting factors - either thrombin (Factor IIa) or Factor Xa - without requiring a cofactor like antithrombin III. They were developed to overcome the limitations of warfarin (narrow therapeutic window, need for monitoring, multiple drug/food interactions, delayed onset).
2. Classification
DIRECTLY ACTING ORAL ANTICOAGULANTS (DOACs)
│
├── Direct Thrombin Inhibitors (Factor IIa inhibitors)
│ └── Dabigatran etexilate (Pradaxa)
│
└── Direct Factor Xa Inhibitors
├── Rivaroxaban (Xarelto)
├── Apixaban (Eliquis)
├── Edoxaban (Savaysa/Lixiana)
└── Betrixaban (Bevyxxa)
Mnemonic for Factor Xa inhibitors: "ARED-B" - Apixaban, Rivaroxaban, Edoxaban, (beta) Betrixaban
Suffix rule: All Factor Xa inhibitors end in "-xaban"; the direct thrombin inhibitor ends in "-gatran"
Suffix rule: All Factor Xa inhibitors end in "-xaban"; the direct thrombin inhibitor ends in "-gatran"
3. Site of Action in the Coagulation Cascade
Intrinsic pathway Extrinsic pathway
↓ ↓
Factor IXa + VIIIa Factor VIIa + TF
↓
Factor Xa ←──── [APIXABAN, RIVAROXABAN, EDOXABAN]
↓
Prothrombin (II) → Thrombin (IIa) ←──── [DABIGATRAN]
↓
Fibrinogen → Fibrin → CLOT
DOACs act downstream at specific single targets in the coagulation cascade, unlike heparin (which potentiates AT-III to inhibit multiple factors) or warfarin (which blocks synthesis of multiple factors).
4. DABIGATRAN
4.1 Mechanism of Action
- Prodrug: Dabigatran etexilate → converted to dabigatran (active form) by plasma esterases after oral absorption
- Active drug is a direct, competitive inhibitor of thrombin (Factor IIa)
- Inhibits both free thrombin AND clot-bound thrombin (advantage over heparin, which cannot inactivate clot-bound thrombin)
- Does NOT require antithrombin as cofactor
4.2 Pharmacokinetics
| Feature | Dabigatran |
|---|---|
| Prodrug | Yes (dabigatran etexilate) |
| Oral bioavailability | 3-7% (low - but clinically effective) |
| Protein binding | ~35% (low) |
| Half-life | 12-17 hours |
| Metabolism | Esterases (NOT CYP450) |
| Excretion | Primarily renal (80%) |
| P-glycoprotein substrate | Yes (important for drug interactions) |
| Food effect | Take with food to reduce GI side effects |
| Renal impairment | Accumulates - dose reduction required; avoid if CrCl <15 mL/min |
4.3 Therapeutic Uses
- Stroke prevention in non-valvular atrial fibrillation (NVAF) - primary indication
- Treatment of DVT and PE (after 5-7 days of initial parenteral anticoagulant)
- Prevention of recurrent DVT/PE
- VTE prophylaxis after hip or knee replacement surgery
- Contraindicated in mechanical prosthetic heart valves and bioprosthetic valves
4.4 Dose
- AF stroke prevention: 150 mg twice daily (CrCl >30 mL/min)
- Reduced dose: 75 mg twice daily (CrCl 15-30 mL/min)
- No monitoring required (routine)
4.5 Adverse Effects
- Bleeding - major adverse effect
- GI side effects - most common and distinctive: dyspepsia, abdominal pain, esophagitis, GI bleeding (due to tartaric acid capsule used to enhance absorption)
- Take with food or full glass of water to reduce GI irritation
- Higher bleeding risk in: elderly (>75 years), renal failure
- No HIT, no osteoporosis
4.6 Antidote
- Idarucizumab (Praxbind) - humanized monoclonal antibody Fab fragment
- Binds dabigatran with very high affinity, neutralizes its effect
- Dose: 5 g IV (for life-threatening bleeding or urgent surgery)
- Also: dialysis can remove dabigatran (low protein binding)
4.7 Monitoring
- Routine monitoring NOT required
- If needed: Thrombin time (TT) or Ecarin Clotting Time (ECT) can reflect drug effect
- aPTT is prolonged but not reliably quantitative
5. RIVAROXABAN
5.1 Mechanism of Action
- Direct, competitive inhibitor of Factor Xa (both free and prothrombinase complex-bound Xa)
- Inhibits Factor Xa in the final common pathway, preventing conversion of prothrombin to thrombin
- Does NOT require antithrombin as cofactor
5.2 Pharmacokinetics
| Feature | Rivaroxaban |
|---|---|
| Oral bioavailability | High (>80%) with food (reduced without food at higher doses) |
| Protein binding | ~92-95% (albumin) |
| Half-life | 5-9 hours (young adults); increased in elderly/renal impairment |
| Metabolism | CYP3A4/5, CYP2J2 |
| Excretion | 1/3 unchanged in urine; remainder as metabolites in urine + feces |
| P-gp substrate | Yes |
| Food effect | Higher doses (15 mg, 20 mg) must be taken with food |
| Renal impairment | Dose reduction for CrCl 15-50 mL/min (AF); avoid <15 mL/min |
5.3 Therapeutic Uses
- Stroke prevention in NVAF
- DVT and PE treatment
- VTE prevention after hip/knee replacement
- Reduction of cardiovascular events in coronary artery disease (CAD) - 2.5 mg BD + aspirin
- Prevention of thrombotic events in peripheral arterial disease (PAD)
- Prevention of recurrent DVT/PE
5.4 Dose
- DVT/PE treatment: 15 mg twice daily x 3 weeks, then 20 mg once daily
- AF: 20 mg once daily with evening meal
- VTE prophylaxis (hip): 10 mg once daily for 35 days
- VTE prophylaxis (knee): 10 mg once daily for 12 days
- No routine monitoring
5.5 Adverse Effects
- Bleeding - major adverse effect
- Less GI side effects than dabigatran
- Liver enzyme elevation (rare)
- Use with caution in hepatic impairment
6. APIXABAN
6.1 Mechanism of Action
- Direct, selective inhibitor of Factor Xa (free and bound Xa)
- Same mechanism as rivaroxaban, but different pharmacokinetic profile
6.2 Pharmacokinetics
| Feature | Apixaban |
|---|---|
| Oral bioavailability | ~50% |
| Protein binding | ~87% |
| Half-life | ~12 hours |
| Metabolism | CYP3A4 (primary); CYP1A2, 2C8, 2C9, 2C19 (minor) |
| Excretion | ~27% renal; remainder biliary/fecal |
| P-gp substrate | Yes |
| Food effect | Can be taken with or without food |
| Renal impairment | Dose reduction with 2 of 3 criteria: age ≥80, weight ≤60 kg, Cr ≥1.5 mg/dL |
6.3 Therapeutic Uses
Same as rivaroxaban:
- Stroke prevention in NVAF
- DVT/PE treatment and prevention
- VTE prophylaxis post-orthopedic surgery
- Reduction of recurrent DVT/PE
6.4 Dose
- AF: 5 mg twice daily (2.5 mg BD if dose reduction criteria met)
- DVT/PE treatment: 10 mg twice daily x 7 days, then 5 mg twice daily
6.5 Adverse Effects
- Bleeding - lowest risk of major bleeding among DOACs (based on ARISTOTLE trial data)
- GI side effects less common than dabigatran
7. EDOXABAN
7.1 Mechanism of Action
- Direct Factor Xa inhibitor
7.2 Pharmacokinetics
| Feature | Edoxaban |
|---|---|
| Oral bioavailability | ~62% |
| Half-life | 10-14 hours |
| Metabolism | Hydrolysis (minimal CYP) |
| Excretion | Primarily unchanged in urine |
| Food effect | Not significantly affected |
| P-gp substrate | Yes |
7.3 Therapeutic Uses
- Stroke prevention in NVAF
- DVT/PE treatment and prevention (after initial 5-10 days of parenteral anticoagulant)
7.4 Dose
- AF / VTE: 60 mg once daily (30 mg once daily for dose reduction)
8. Antidote for Factor Xa Inhibitors
- Andexanet alfa (Andexxa) - recombinant modified Factor Xa "decoy" molecule
- Competes with native Factor Xa for binding to the inhibitor
- Rapidly reverses anti-Xa effect of apixaban and rivaroxaban
- FDA-approved for life-threatening bleeding
- Low dose: 400 mg IV bolus at 30 mg/min → 4 mg/min infusion for 120 min
- High dose: 800 mg IV bolus → 8 mg/min infusion for 120 min
- 4-factor Prothrombin Complex Concentrate (PCC) - used as alternative
- No specific antidote for edoxaban; andexanet alfa and PCC are used
9. Comparison of All DOACs
| Feature | Dabigatran | Rivaroxaban | Apixaban | Edoxaban |
|---|---|---|---|---|
| Target | Factor IIa (thrombin) | Factor Xa | Factor Xa | Factor Xa |
| Prodrug | Yes | No | No | No |
| Bioavailability | 3-7% | >80% (with food) | ~50% | ~62% |
| Half-life | 12-17 h | 5-9 h | ~12 h | 10-14 h |
| Dosing | Twice daily | Once daily (most) | Twice daily | Once daily |
| Renal excretion | 80% (highest) | ~33% | ~27% | ~50% |
| CYP metabolism | No (esterases) | CYP3A4 | CYP3A4 | Minimal |
| P-gp substrate | Yes | Yes | Yes | Yes |
| Food requirement | With food (GI SE) | Higher doses with food | Not required | Not required |
| Antidote | Idarucizumab | Andexanet alfa / PCC | Andexanet alfa / PCC | Andexanet alfa / PCC |
| GI side effects | Most common | Less | Less | Less |
| Renal caution | Most (80% renal) | Moderate | Least | Moderate |
| Monitoring | Not required | Not required | Not required | Not required |
| Liver metabolism | Minimal | Yes (CYP3A4) | Yes (CYP3A4) | Minimal |
10. Advantages of DOACs over Warfarin
| Feature | DOACs | Warfarin |
|---|---|---|
| Route | Oral | Oral |
| Onset | Rapid (2-4 hours) | Delayed (72-96 hours) |
| Monitoring | Not required (fixed dose) | Required (INR) |
| Food interactions | Minimal | Extensive (Vitamin K foods) |
| Drug interactions | Fewer | Extensive (CYP450) |
| Therapeutic window | Wider, predictable | Narrow, unpredictable |
| Reversal agents | Specific antidotes available | Vitamin K (slow) + FFP/PCC |
| Use in AF | Yes (non-valvular only) | Yes (including valvular) |
| Mechanical heart valves | Contraindicated | Preferred |
| Pregnancy | Contraindicated | Contraindicated |
| Renal failure | Caution/contraindicated | Safer (hepatic metabolism) |
| Bridging required | No | Yes (with heparin) |
11. Common Contraindications for ALL DOACs
- Pregnancy and lactation (all are teratogenic / insufficient safety data)
- Mechanical prosthetic heart valves (warfarin preferred - DOACs inferior, especially dabigatran)
- Severe renal failure (CrCl <15-30 mL/min, drug-dependent)
- Severe hepatic failure (impairs metabolism + coagulopathy)
- Active major bleeding
- Valvular atrial fibrillation (rheumatic MS) - warfarin preferred
12. Drug Interactions (Common to DOACs)
All DOACs are P-glycoprotein (P-gp) substrates, and factor Xa inhibitors are also CYP3A4 substrates:
Drugs that INCREASE DOAC levels (bleeding risk):
- P-gp inhibitors: Amiodarone, verapamil, dronedarone, clarithromycin, ketoconazole, itraconazole
- CYP3A4 inhibitors (Xa inhibitors): Same azoles, HIV protease inhibitors
Drugs that DECREASE DOAC levels (thrombosis risk):
- P-gp/CYP3A4 inducers: Rifampicin, carbamazepine, phenytoin, phenobarbitone, St. John's wort
13. Summary - High-Yield Points for Exams
| Question | Answer |
|---|---|
| Only oral direct thrombin inhibitor | Dabigatran |
| Prodrug among DOACs | Dabigatran |
| DOAC with highest renal excretion | Dabigatran (80%) - most affected by renal failure |
| DOAC with lowest renal excretion | Apixaban (~27%) - safest in renal failure |
| DOAC that must be taken with food (higher doses) | Rivaroxaban |
| GI side effects most common with | Dabigatran |
| Antidote for dabigatran | Idarucizumab |
| Antidote for Xa inhibitors | Andexanet alfa |
| DOAC contraindicated in mechanical valves | All DOACs (especially dabigatran) |
| Monitoring test for DOACs | None routinely; TT/ECT for dabigatran if needed |
| DOAC safe in valvular (rheumatic) AF | None - use warfarin |
| DOAC approved for CAD/PAD in addition to AF | Rivaroxaban (2.5 mg BD) |
| Suffix for all direct thrombin inhibitors | -gatran |
| Suffix for all Xa inhibitors | -xaban |
Sources: Lippincott Illustrated Reviews: Pharmacology, pp. 461-464; Katzung's Basic & Clinical Pharmacology, 16th ed., pp. 964-968
Methyl alcohol poisoning according to shanbhag pharmacology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a thorough Shanbhag-style answer. Here it is:
Methyl Alcohol (Methanol) Poisoning - As per Shanbhag Style
The library does not contain the Shanbhag textbook directly. This is presented in the standard Shanbhag/KDT Indian pharmacology curriculum format, compiled from Katzung's Basic & Clinical Pharmacology (16th ed.), Goodman & Gilman's Pharmacological Basis of Therapeutics, and Tintinalli's Emergency Medicine.
1. Introduction
Methyl alcohol (methanol, wood alcohol, CH₃OH) is a colorless, flammable liquid with physicochemical properties similar to ethanol but with entirely different and far more dangerous toxicity. It is a common cause of mass poisoning outbreaks - particularly when illicitly mixed into country liquor or consumed as a substitute for ethanol.
Sources of exposure:
- Illicit/adulterated liquor (most common cause in India)
- Industrial solvents, paint removers, shellac, varnish
- Antifreeze, windshield-washing fluids
- "Canned heat" (Sterno) products
- Accidental ingestion; occupational inhalation or skin absorption
Lethal dose: As little as 8-10 mL (1 tablespoon) can cause blindness; 30 mL can be fatal. However, individual susceptibility varies widely.
2. Metabolism - The Key to Understanding Toxicity
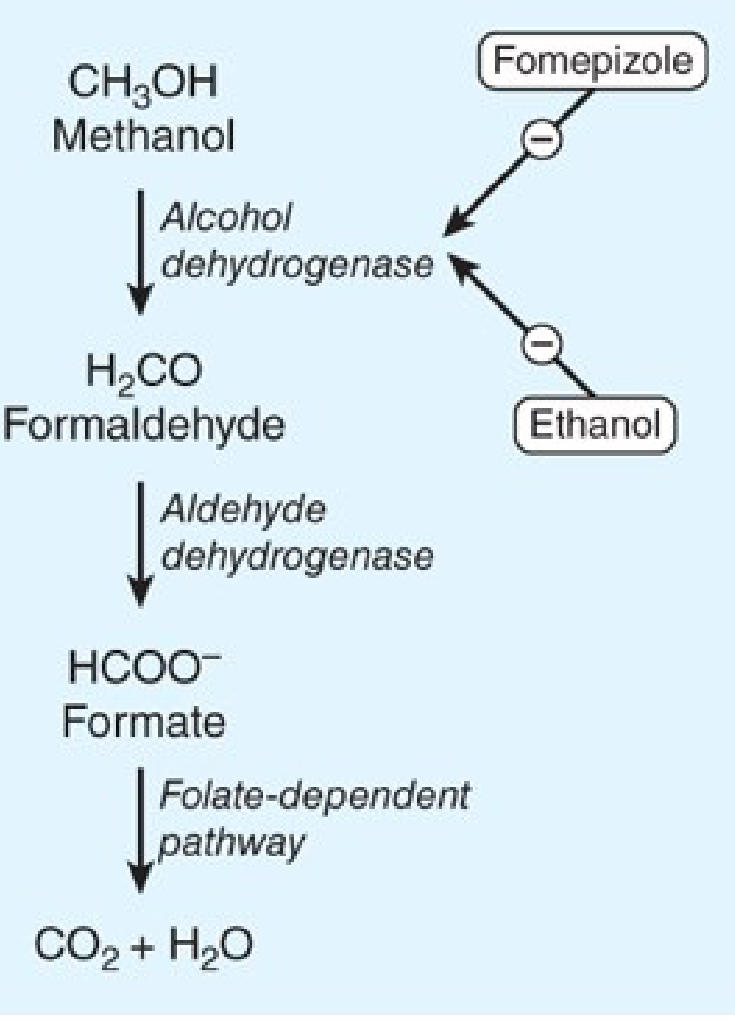
Figure: Methanol → Formaldehyde (by ADH) → Formate/Formic acid (by ALDH) → CO₂ + H₂O (folate-dependent). Fomepizole and ethanol competitively inhibit ADH, blocking toxic metabolite formation.
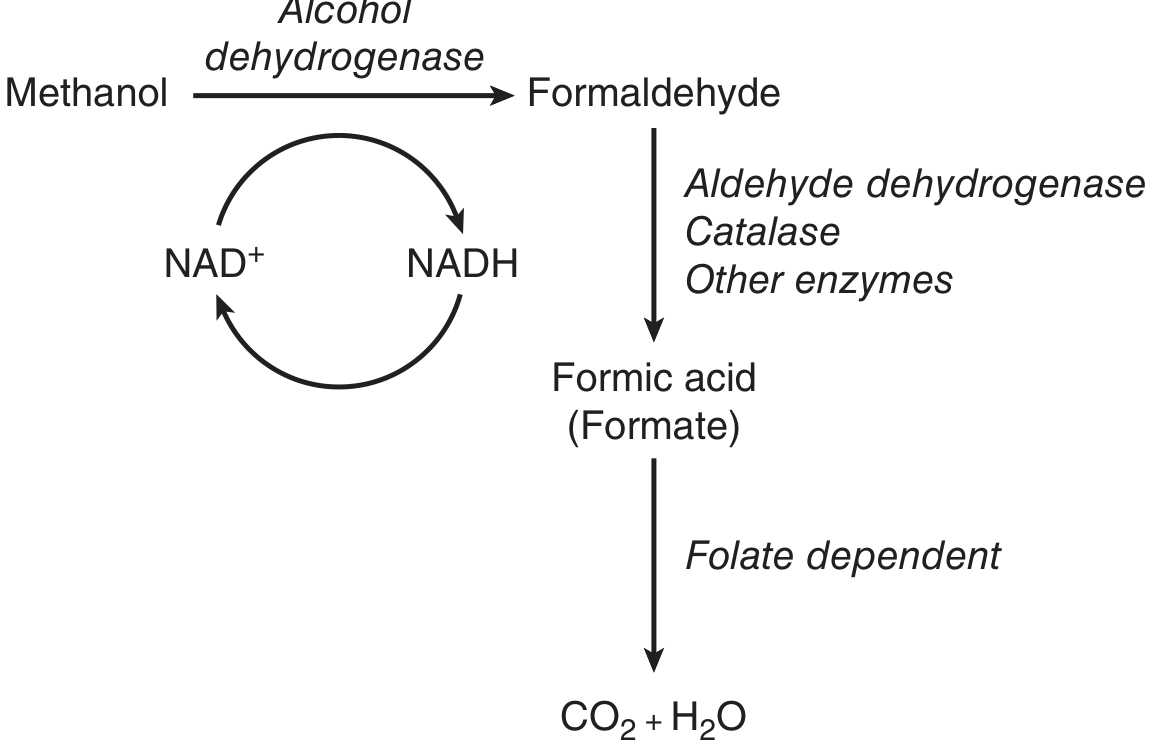
Step-by-step metabolism:
CH₃OH (Methanol)
↓ Alcohol Dehydrogenase (ADH) + NAD⁺
H₂CO (Formaldehyde)
↓ Aldehyde Dehydrogenase (ALDH) / Catalase
HCOO⁻ (Formic acid / Formate) ← THE TOXIC METABOLITE
↓ Folate-dependent pathway (THF)
CO₂ + H₂O (harmless end products)
Critical points:
- Methanol itself has LOW toxicity - it is only a mild inebriant
- Toxicity is ENTIRELY due to its metabolites - formaldehyde and especially formic acid
- Humans are uniquely susceptible because formate is cleared slowly (folate-dependent clearance is limited)
- Conversion of methanol to toxic metabolites is slow (6-30 hours) → explains the characteristic latent period between ingestion and onset of serious symptoms
- Co-ingestion of ethanol delays toxicity (ethanol competitively occupies ADH, slowing methanol metabolism)
3. Why is Formic Acid so Toxic?
Formic acid (formate) is the primary mediator of all serious toxicity:
- Inhibits cytochrome c oxidase (Complex IV in mitochondria) → blocks oxidative phosphorylation → histotoxic hypoxia
- This drives anaerobic metabolism → lactic acidosis
- The increased NADH/NAD⁺ ratio (from ADH reaction) also favors conversion of pyruvate → lactate → worsens lactic acidosis
- The resulting acidosis (↓pH) further worsens formate toxicity:
- Acidemia favors the undissociated formic acid form (over formate ion)
- Undissociated formic acid crosses membranes more readily → enters retina, optic nerve, and brain
- Lower pH also increases tubular reabsorption of formate → prolongs elimination
- Optic nerve and retinal ganglion cells are especially sensitive → characteristic ocular toxicity
Net result: Severe high-anion-gap metabolic acidosis + optic nerve/retinal injury + CNS depression
4. Clinical Features
4.1 Latent Period (6-24 hours)
After ingestion, methanol causes only mild, transient inebriation - far milder than equivalent dose of ethanol. The patient may appear almost asymptomatic during this period while metabolites are accumulating.
- Duration shortened if: large dose ingested, no co-ingestion of ethanol
- Duration prolonged if: ethanol co-ingested (ethanol competes with methanol for ADH)
4.2 Stages of Toxicity
Stage 1: Initial inebriation (0-6 hours)
- Mild euphoria, drunkenness (weaker than ethanol)
- Nausea, vomiting, gastritis, abdominal pain
- Headache, dizziness
- Elevated osmolal gap (methanol itself contributes to osmolality before metabolism)
Stage 2: Latent period (6-24 hours)
- Relative asymptomatic interval
- Methanol being metabolized to formic acid but clinical signs not yet obvious
Stage 3: Toxic phase (12-48 hours)
| System | Features |
|---|---|
| Visual (most characteristic) | Blurred vision, photophobia, "snowstorm vision" (like looking through snow), scotomas → blindness (permanent if untreated); papilledema, fixed dilated pupils (mydriasis) = ominous sign |
| CNS | Headache, vertigo, confusion, seizures, coma |
| Metabolic | Severe high-anion-gap metabolic acidosis (HAGMA), Kussmaul breathing (compensatory hyperventilation) |
| GI | Nausea, vomiting, abdominal pain, pancreatitis |
| CVS | Tachycardia, hypotension, shock (late and severe) |
| Renal | Oliguria, renal failure (late) |
| Respiratory | Tachypnea (compensation), respiratory failure (late) |
| Odour | Formaldehyde odour on breath/urine (in severe cases) |
Poor prognostic signs:
- Bradycardia
- Prolonged coma
- Seizures
- Severe resistant acidosis (pH <7.0)
- Fixed dilated pupils
5. Diagnosis
5.1 Laboratory Findings
| Investigation | Finding |
|---|---|
| Serum methanol | Elevated (>20 mg/dL = treat; >50 mg/dL = hemodialysis) |
| Arterial blood gas (ABG) | Metabolic acidosis, low pH, low HCO₃⁻, low pCO₂ (compensatory) |
| Anion gap | Elevated (HAGMA) - due to formate + lactate |
| Osmolal gap | Elevated early (methanol raises serum osmolality); Gap = measured - calculated osmolality; normal <10 |
| Serum formate | Elevated (best correlate of toxicity, but not widely available) |
| Blood glucose | May be low (hypoglycemia) |
| Serum lactate | Elevated |
| Fundoscopy | Optic disc hyperaemia, papilledema, retinal oedema |
| CT head | Bilateral putamen necrosis (basal ganglia haemorrhage), subcortical white matter damage |
5.2 Diagnostic Formula (for exam)
- Osmolal gap = Measured serum osmolality - Calculated osmolality
- Calculated osmolality = 2[Na] + [glucose/18] + [BUN/2.8]
- Elevated osmolal gap early + elevated anion gap later = classic pattern of methanol/toxic alcohol poisoning
6. Treatment
Step 1: General Supportive Measures (ABC)
- Airway - secure airway, intubate if necessary (respiratory depression, coma)
- Breathing - supplemental oxygen, ventilatory support
- Circulation - IV fluids, vasopressors for shock
- Gastric lavage - only if within 1-2 hours of ingestion (methanol absorbed rapidly)
- Monitor blood gases, electrolytes, renal function, visual acuity regularly
Step 2: Correct Metabolic Acidosis
- IV Sodium Bicarbonate (NaHCO₃)
- Alkalinization serves a dual purpose:
- Corrects acidosis
- Converts formic acid → formate ion (ionized form) → less membrane-permeable → cannot enter CNS/retina as easily → reduces ocular and CNS toxicity
- Also increases renal excretion of formate (ionized form not reabsorbed as readily)
Step 3: Inhibit Toxic Metabolite Formation (THE KEY TREATMENT)
The goal is to block ADH, preventing conversion of methanol to formaldehyde and formic acid.
A. Fomepizole (4-methylpyrazole) - PREFERRED ANTIDOTE
- Mechanism: Potent competitive inhibitor of alcohol dehydrogenase (ADH)
- Blocks methanol → formaldehyde → formic acid conversion
- Route: Intravenous infusion
- Dose:
- Loading dose: 15 mg/kg IV
- Then: 10 mg/kg every 12 hours x 4 doses (48 hours)
- Then: 15 mg/kg every 12 hours (because fomepizole induces its own CYP450 metabolism after 48 hours)
- Continue until serum methanol <20-30 mg/dL
- During hemodialysis: administer every 4 hours (dialysis removes fomepizole)
- Advantages: Safe, predictable, no CNS depression, no monitoring of serum levels required
- Adverse effects: Burning at infusion site, headache, nausea, dizziness (mild and transient)
- Do NOT combine with ethanol (fomepizole prolongs ethanol half-life)
B. Ethanol - ALTERNATIVE (when fomepizole unavailable)
- Mechanism: Ethanol has 10-20x higher affinity for ADH than methanol → competitively displaces methanol from ADH → methanol cannot be metabolized to toxic products → methanol eliminated unchanged by lungs and kidneys
- Route: IV (5% ethanol in 5% dextrose) or oral (whisky/brandy - 40% ethanol)
- Target blood ethanol level: 100-150 mg/dL (must be maintained continuously)
- Loading dose (oral): ~0.6 g/kg (e.g., 1 mL/kg of absolute alcohol)
- Maintenance: 0.1-0.2 g/kg/hour (adjust based on serum ethanol monitoring)
- Disadvantages:
- CNS depression, hypoglycemia (especially in children)
- Difficult to titrate, requires frequent monitoring
- Unreliable in alcoholic patients (high tolerance → faster clearance)
- Cannot be used with fomepizole
- During hemodialysis: ethanol is also dialyzed → dose must be increased
| Feature | Fomepizole | Ethanol |
|---|---|---|
| Affinity for ADH | High, predictable | Moderate |
| CNS depression | None | Significant |
| Monitoring required | Not needed | Serum levels (frequent) |
| Hypoglycemia | No | Yes |
| Availability | Limited (expensive) | Readily available |
| Preferred | Yes | Alternative when fomepizole unavailable |
Step 4: Remove Methanol and Toxic Metabolites
Hemodialysis - INDICATIONS (Any one of the following):
- Serum methanol >50 mg/dL
- Severe metabolic acidosis (pH <7.15-7.2)
- Visual symptoms or signs of optic nerve injury
- Renal failure
- Clinical deterioration despite other treatment
- Large ingestion with rising osmolal gap
Why dialysis works: Methanol and formate are both small, water-soluble molecules that are efficiently cleared by hemodialysis. Also dialyzes fomepizole/ethanol (dosing must be adjusted).
Step 5: Folinic Acid (Leucovorin) or Folic Acid
- Formate is cleared by the folate-dependent one-carbon metabolism pathway
- Folate administration may enhance formate elimination by providing the cofactor for this pathway
- Folinic acid (leucovorin) 1 mg/kg IV (up to 50 mg) every 4-6 hours
- May be of benefit in enhancing formate clearance; simple and safe to administer
Step 6: Treatment of Ocular Involvement
- No specific treatment for formate-induced optic nerve damage once established
- Early ADH inhibition and alkalinization are the primary preventive strategies
- Ophthalmology consultation
7. Summary of Treatment Algorithm
METHANOL POISONING SUSPECTED
↓
1. SUPPORTIVE: ABC, IV access, O₂
2. CORRECT ACIDOSIS: IV Sodium Bicarbonate
3. INHIBIT METABOLISM:
→ Fomepizole (preferred) 15 mg/kg IV loading
→ OR Ethanol (if fomepizole unavailable) - target 100-150 mg/dL
4. CONSIDER HEMODIALYSIS if:
→ Methanol >50 mg/dL
→ Severe acidosis, visual symptoms, renal failure
5. FOLINIC ACID - to enhance formate elimination
6. MONITORING: ABG, electrolytes, visual acuity, serum methanol levels
8. Mechanism of Ethanol as Antidote - Detailed (Shanbhag Favourite)
| Step | What Happens |
|---|---|
| 1 | Both ethanol and methanol are substrates for ADH |
| 2 | Ethanol has ~10-20x greater affinity for ADH |
| 3 | When ethanol is present at adequate levels, ADH is occupied by ethanol |
| 4 | Methanol cannot access ADH → not metabolized to toxic formaldehyde/formate |
| 5 | Methanol is excreted unchanged via lungs (exhaled) and kidneys (slow but non-toxic) |
| 6 | Ethanol itself is metabolized harmlessly to acetaldehyde → acetate → CO₂ + H₂O |
| 7 | This buys time for hemodialysis to remove accumulated methanol |
This is also why patients who consume alcohol (ethanol) regularly have a delayed or attenuated course of methanol toxicity - their ADH is already occupied.
9. High-Yield Summary Table
| Feature | Methanol Poisoning |
|---|---|
| Also called | Methyl alcohol / Wood alcohol |
| Toxic metabolites | Formaldehyde → Formic acid (formate) |
| Primary toxic metabolite | Formic acid |
| Mechanism of toxicity | Formate inhibits cytochrome c oxidase → histotoxic hypoxia + lactic acidosis |
| Characteristic symptom | Visual disturbance - "snowstorm vision" → blindness |
| Acid-base disturbance | High anion gap metabolic acidosis |
| Early lab finding | Elevated osmolal gap |
| Late lab finding | Elevated anion gap |
| Latent period | 6-30 hours (while metabolites accumulate) |
| Lethal dose | ~30 mL |
| Blindness dose | ~8-10 mL |
| Preferred antidote | Fomepizole (ADH inhibitor) |
| Alternative antidote | Ethanol (competitive ADH inhibitor) |
| Target ethanol level | 100-150 mg/dL |
| Dialysis indication | Methanol >50 mg/dL, severe acidosis, visual symptoms |
| Adjunct treatment | Sodium bicarbonate + Folinic acid |
| Death from | Respiratory arrest |
| Key CT finding | Bilateral putamen necrosis |
| Difference from ethanol | Causes blindness, severe acidosis; NOT just intoxication |
Sources: Katzung's Basic & Clinical Pharmacology, 16th ed., pp. 632-633; Goodman & Gilman's Pharmacological Basis of Therapeutics, pp. 541; Tintinalli's Emergency Medicine, pp. 1268-1270
This is a shared conversation. Sign in to Orris to start your own chat.