Explain pneumonia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pneumonia"[MeSH Terms] AND "diagnosis AND treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have everything needed for a thorough, well-sourced answer. Here it is:
Pneumonia
Definition
Pneumonia is an infection of the lung parenchyma that leads to consolidation of the normally air-filled alveoli. It can be caused by bacteria, viruses, mycobacteria, mycoplasma, and fungi. Systemic viral infections (influenza A/B, measles, varicella) can also precipitate secondary bacterial pneumonia.
- Textbook of Family Medicine 9e, p. 321
Epidemiology
- Pneumonia and influenza account for over 1 million hospital admissions per year in the United States, with an in-hospital mortality rate of 3.3%.
- Aggregate hospital charges exceed $35 billion per year.
- In children, bacterial pathogens cause only 10-30% of all infectious pneumonias; Streptococcus pneumoniae has historically been the most common bacterial cause, though this is declining with universal vaccination.
Classification
Pneumonia is primarily classified by the setting in which it is acquired:
| Type | Definition | Common Pathogens |
|---|---|---|
| Community-Acquired (CAP) | Acquired outside a hospital/institution | S. pneumoniae, Mycoplasma, Chlamydia, Legionella, influenza |
| Hospital-Acquired (HAP) | Develops ≥48 h after hospital admission | Gram-negative rods (Pseudomonas, Klebsiella), Staphylococcus aureus (including MRSA) |
| Ventilator-Associated (VAP) | Develops ≥48-72 h after endotracheal intubation | Multi-drug-resistant gram-negatives, MRSA |
| Aspiration Pneumonia | Aspiration of oropharyngeal/gastric contents | Anaerobes (Peptostreptococcus, Bacteroides), gram-negatives |
| Opportunistic Pneumonia | In immunocompromised hosts | Pneumocystis jirovecii (PCP), Cryptococcus, Aspergillus, CMV |
Patients in nursing homes or with prolonged hospitalization are at high risk for colonization with gram-negative organisms and multidrug-resistant (MDR) bacteria.
Pathophysiology
- Inoculation: Pathogens reach the lower respiratory tract via inhalation, aspiration of oropharyngeal secretions, or hematogenous spread.
- Inflammatory response: The innate immune system responds with cytokine release, neutrophil recruitment, and exudate formation in the alveoli.
- Consolidation: Alveoli fill with inflammatory cells, fluid, and debris, replacing air - this is what appears as opacification on chest X-ray and produces the clinical findings of consolidation.
- Resolution or complication: In most cases, the lung returns to normal. Complications include parapneumonic effusion, empyema, lung abscess, bacteremia, and ARDS.
Clinical Presentation
The presentation depends on the causative organism:
Typical (Bacterial) Pneumonia
- Rapid onset of high fever, rigors, productive cough (purulent or blood-streaked sputum), pleuritic chest pain, dyspnea
- Physical exam: decreased breath sounds, dullness to percussion, egophony over the affected lobe
- WBC markedly elevated (>15,000 × 10³/mm³) with neutrophilia
- Classic example: pneumococcal lobar pneumonia
Atypical Pneumonia
- Smoldering onset with low-grade fever, non-productive ("dry") cough, myalgias, headache, fewer constitutional symptoms
- Patchy or interstitial infiltrates on CXR ("walking pneumonia")
- Caused by Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophila, and respiratory viruses
In Children
-
Malaise, cough, chest pain, tachypnea, intercostal retractions
-
Tachypnea disproportionate to the degree of fever is the earliest clue in children
-
Viral pneumonia: less toxic appearance, low-grade fever, wheezing
-
Bacterial pneumonia: high fever, chills, dyspnea, acutely ill appearance
-
Textbook of Family Medicine 9e, p. 321-322
Diagnosis
Chest X-Ray
The cornerstone of diagnosis. Findings:
- Lobar/segmental consolidation - typical bacterial (e.g., pneumococcal)
- Patchy bilateral infiltrates - atypical organisms or viral
- Interstitial pattern - Mycoplasma, viral, PCP
- Pleural effusion if parapneumonic effusion or empyema has developed
Laboratory
-
CBC: leukocytosis with left shift in bacterial; normal or low in viral/atypical
-
Blood cultures: positive in 10-15% of hospitalized CAP patients; important for guiding targeted therapy
-
Sputum Gram stain and culture: most useful when collected before antibiotics
-
Urine antigens: available for S. pneumoniae and Legionella - results available within the ED timeframe
-
PCR panels (e.g., BioFire): rapidly identify a wide variety of bacterial and viral pathogens; particularly useful in outbreak settings (e.g., SARS-CoV-2)
-
Procalcitonin: helps distinguish bacterial from viral etiology
-
ROSEN's Emergency Medicine, p. 976
Severity Assessment - PSI / CURB-65
The CURB-65 score is widely used to determine the need for hospitalization:
| Criterion | Points |
|---|---|
| Confusion | 1 |
| Urea >7 mmol/L (BUN >20 mg/dL) | 1 |
| Respiratory rate ≥30/min | 1 |
| Blood pressure <90 systolic or ≤60 diastolic | 1 |
| Age ≥ 65 years | 1 |
- Score 0-1: Outpatient treatment
- Score 2: Consider hospital admission
- Score 3-5: Hospitalization; score ≥4 consider ICU
Severe CAP Criteria (ATS/IDSA)
Patients with any one major criterion (need for invasive mechanical ventilation, or septic shock requiring vasopressors) or three or more minor criteria are classified as severe CAP and should be admitted to the ICU.
Treatment
Outpatient CAP (Adults)
| Clinical Setting | Regimen |
|---|---|
| Previously healthy, no antibiotics in last 3 months | Amoxicillin 1g PO three times daily x7 days or Doxycycline 100 mg PO twice daily x7 days |
| Comorbidities (chronic cardiac, lung, liver, or renal disease) or recent antibiotics | Amoxicillin/clavulanate + azithromycin or Respiratory fluoroquinolone (levofloxacin 750 mg daily x5 days) |
Note: Macrolide monotherapy is no longer routinely recommended for CAP unless local pneumococcal resistance is <25%. Most areas in the US do not meet this threshold.
Inpatient CAP (Non-Severe)
- Beta-lactam (ceftriaxone, ampicillin-sulbactam, or ceftaroline) + macrolide (azithromycin)
- OR respiratory fluoroquinolone monotherapy (levofloxacin or moxifloxacin)
Severe CAP / ICU
- Beta-lactam + macrolide or beta-lactam + fluoroquinolone
- Add vancomycin or linezolid if CA-MRSA is suspected (necrotizing pneumonia, post-influenza, sepsis in a young healthy adult)
Hospital-Acquired / Ventilator-Associated Pneumonia
-
Broader coverage targeting MDR gram-negatives and MRSA
-
Piperacillin-tazobactam, cefepime, or carbapenem + vancomycin or linezolid
-
ROSEN's Emergency Medicine, p. 977-979
Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion / Empyema | Complicates ~30-40% of streptococcal pneumonia; requires drainage if infected |
| Lung abscess | Typically due to aspiration or Staphylococcus; cavitating lesion on CXR |
| Bacteremia | Occurs in 10-15% of cases; worsens prognosis |
| ARDS | Severe alveolar injury; high mortality |
| Sepsis/Septic shock | Systemic inflammatory response to infection |
| Metastatic infection | Meningitis, endocarditis, septic arthritis (especially with bacteremia) |
Prevention
- Annual influenza vaccine: all persons ≥6 months; especially those >50 years, chronic lung disease, diabetes, immune dysfunction
- Pneumococcal vaccine (PCV/PPSV23): recommended for all adults ≥65; revaccinate with PPSV23 after 10 years if first dose was given before age 65
- Smoking cessation (smoking is a major risk factor for CAP)
- Infection control and hand hygiene in hospitals (HAP/VAP prevention)
Quick Summary Table
| Feature | Typical Pneumonia | Atypical Pneumonia |
|---|---|---|
| Onset | Abrupt | Gradual |
| Fever | High, with rigors | Low-grade |
| Cough | Productive, purulent | Dry, non-productive |
| WBC | Markedly elevated | Normal/mildly elevated |
| CXR | Lobar consolidation | Patchy, bilateral, interstitial |
| Examples | S. pneumoniae, Staph. aureus | Mycoplasma, Legionella, viruses |
Sources: Textbook of Family Medicine 9e | ROSEN's Emergency Medicine | Murray & Nadel's Textbook of Respiratory Medicine | Goldman-Cecil Medicine
COPD
Reading File
Finding Sources
Searching PubMed
"pulmonary disease, chronic obstructive"[MeSH Terms] AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, detailed content from multiple authoritative textbooks. Let me compile the full answer.
Chronic Obstructive Pulmonary Disease (COPD)
Definition
COPD is a common, preventable, and treatable disease characterized by persistent, progressive airflow limitation that is not fully reversible with bronchodilator therapy. The obstruction reflects an abnormal inflammatory response of the lung to noxious particles or gases, most commonly cigarette smoke. It encompasses two overlapping conditions - emphysema and chronic bronchitis - that typically coexist.
- Chronic bronchitis is defined clinically: a persistent productive cough for at least 3 consecutive months in at least 2 consecutive years.
- Emphysema is defined pathologically: abnormal, permanent enlargement of air spaces distal to the terminal bronchioles, with destruction of alveolar walls.
COPD is the third most common cause of death in the United States and accounts for over $40 billion per year in direct and indirect health care costs.
Etiology and Risk Factors
| Risk Factor | Notes |
|---|---|
| Cigarette smoking | Overwhelmingly the dominant cause; accounts for ~85-90% of cases |
| Air pollution | Indoor (biomass fuel combustion), outdoor particulates |
| Occupational exposure | Dust, fumes, chemical vapors (coal mining, construction) |
| Alpha-1 antitrypsin (AAT) deficiency | Genetic cause; suspect if COPD onset before age 45 or in a non-smoker |
| Respiratory infections | Recurrent childhood infections reduce lung development |
| Airway hyperresponsiveness | Even without full asthma phenotype |
Any patient developing COPD without significant smoking history or before age 45 should be screened for alpha-1 antitrypsin deficiency.
Pathophysiology
Emphysema
- Cigarette smoke activates neutrophils and macrophages in the alveolar walls
- These cells release proteases (especially elastase, MMP-12) that destroy the elastic connective tissue of alveolar walls
- The resulting loss of elastic recoil leads to:
- Air trapping and static lung hyperinflation
- Collapse of small airways on expiration (dynamic airway collapse)
- Increased lung compliance, barrel chest
- Two subtypes:
- Centriacinar (centrilobular): Most common; smoking-related; upper lobe predominance; destruction around respiratory bronchioles
- Panacinar (panlobular): Seen in alpha-1 antitrypsin deficiency; uniform destruction of acinus; lower lobe predominance
Chronic Bronchitis
- Toxic inhalants trigger mucus hypersecretion from:
- Hyperplasia of submucosal mucus glands (Reid index >0.4)
- Goblet cell metaplasia in small airways
- Ciliary dysfunction reducing mucociliary clearance
- Small airway inflammation and fibrosis causes obstructive bronchiolitis - the main site of airflow limitation
- Results in hypoxemia and hypercapnia (V/Q mismatch)
- Persistent infection (especially H. influenzae) perpetuates inflammation
Dynamic Hyperinflation
In moderate-to-severe COPD, the increased ventilatory demand of exercise combined with insufficient expiratory time causes air trapping. End-expiratory lung volume (EELV) fails to return to baseline, causing:
-
Reduced inspiratory reserve volume
-
Inspiratory muscle weakness and increased work of breathing
-
Neuromechanical uncoupling (effort >> tidal volume response)
-
This is the primary driver of dyspnea and exercise intolerance in COPD
-
Fishman's Pulmonary Diseases and Disorders, p. (block 7)
Gas Exchange Abnormalities
COPD causes V/Q mismatch - perfused alveoli that are poorly ventilated dilute oxygenated blood, reducing arterial PO₂. The classic ABG pattern in a severe COPD patient:
-
PaO₂: markedly reduced (~60 mmHg)
-
PaCO₂: may be elevated (type 2 respiratory failure) in bronchitic phenotype, or low if hyperventilating
-
Compensatory polycythemia over time (chronic hypoxemia stimulates EPO)
-
Costanzo Physiology 7th Edition
Clinical Presentation
Symptoms
- Dyspnea on exertion - the hallmark symptom; slowly progressive over years
- Chronic productive cough - especially morning sputum
- Wheeze - particularly during exacerbations
- Fatigue, exercise intolerance, weight loss in advanced disease
Physical Examination
| Sign | Mechanism |
|---|---|
| Barrel chest (increased AP diameter) | Static lung hyperinflation |
| Pursed-lip breathing | Creates back-pressure to prevent airway collapse on expiration |
| Use of accessory muscles | Increased work of breathing |
| Hyperresonance on percussion | Air trapping |
| Decreased breath sounds | Loss of lung tissue |
| Prolonged expiration | Airflow obstruction |
| Central cyanosis | Hypoxemia |
| Clubbing | Consider if present - suggests alternative diagnosis (e.g., bronchiectasis, lung cancer) |
"Pink Puffer" vs "Blue Bloater" (Classic but Simplified)
| Feature | Emphysema ("Pink Puffer") | Chronic Bronchitis ("Blue Bloater") |
|---|---|---|
| Body habitus | Thin, cachexic | Obese |
| Cyanosis | Absent or late | Present (central) |
| Cough | Minimal | Prominent, productive |
| PaCO₂ | Normal or low | Elevated |
| PaO₂ | Near normal at rest | Reduced |
| CXR | Hyperinflation, flattened diaphragm | Increased bronchovascular markings |
| Cor pulmonale | Late | Early |
In practice, most patients have a mixed phenotype.
Diagnosis
Spirometry (Gold Standard)
COPD is confirmed by post-bronchodilator spirometry showing:
- FEV₁/FVC ratio < 0.70 (obstructive pattern)
- FVC may be reduced but FEV₁ is disproportionately reduced
- The obstruction is NOT fully reversible (<12% and <200 mL improvement after bronchodilator)
A restrictive pattern (low FVC with normal FEV₁/FVC) points to an alternative diagnosis (fibrosis, CHF, sarcoidosis).
GOLD Severity Classification (Based on Post-Bronchodilator FEV₁)
| GOLD Grade | FEV₁ (% predicted) | Severity |
|---|---|---|
| GOLD 1 | ≥80% | Mild |
| GOLD 2 | 50-79% | Moderate |
| GOLD 3 | 30-49% | Severe |
| GOLD 4 | <30% | Very Severe |
The GOLD grading correlates strongly with exacerbation frequency and 3-year mortality (moderate COPD: 11% 3-year mortality; very severe COPD: 24%).
ABCD Assessment (Symptom + Exacerbation Burden)
Combines spirometry grade with:
- Symptom burden: CAT score ≥10 or mMRC ≥2 = more symptomatic
- Exacerbation history: ≥2 exacerbations/year or ≥1 hospitalization = high risk
This gives groups A, B, E (formerly C/D) to guide therapy escalation.
Additional Investigations
- Chest X-ray: Hyperinflation (flattened diaphragms, increased retrosternal space, hyperlucency); useful to exclude other diagnoses
- HRCT: Identifies emphysema distribution, bronchiectasis, or ILD
- ABG: For patients with FEV₁ <50% or clinical signs of hypoxemia/hypercapnia
- Alpha-1 antitrypsin level: Screen when indicated
- 6-Minute Walk Test: Functional limitation; <149 m indicates severe impairment
- ECG/Echocardiogram: Assess for cor pulmonale and right ventricular dysfunction
Differential Diagnosis (GOLD Guidelines)
| Condition | Distinguishing Features |
|---|---|
| Asthma | Early onset, variable symptoms, largely reversible airflow, atopic history |
| CHF | Fine basilar crackles, dilated heart on CXR, restrictive pattern on PFTs |
| Bronchiectasis | Large volumes of purulent sputum, coarse crackles, clubbing, CT shows dilation |
| TB | Infiltrates on CXR, microbiologic confirmation |
| Obliterative bronchiolitis | Younger, non-smoker, history of RA or fume exposure |
- Textbook of Family Medicine 9e, p. 314-316
Management
Non-Pharmacological (Most Important)
- Smoking cessation - the single most effective intervention to slow FEV₁ decline; all smokers must be offered cessation support
- Pulmonary rehabilitation - improves dyspnea, exercise capacity, and quality of life in all symptomatic patients
- Long-term oxygen therapy (LTOT) - for patients with resting PaO₂ ≤55 mmHg (or ≤59 mmHg with cor pulmonale/polycythemia); the only therapy proven to improve survival in COPD; use ≥15 hours/day
- Vaccination: Annual influenza + pneumococcal vaccine (PPSV23/PCV)
- Nutritional support for underweight patients
- Exercise training as part of rehabilitation
Pharmacological Treatment - Stepwise Approach
Short-Acting Bronchodilators (Rescue)
- SABA (Short-Acting Beta-2 Agonist): Albuterol/salbutamol - for immediate symptom relief
- SAMA (Short-Acting Muscarinic Antagonist): Ipratropium bromide - can be used as alternative or combined with SABA
Long-Acting Bronchodilators (Maintenance - First Line)
All symptomatic patients should receive a long-acting bronchodilator:
- LAMA (Long-Acting Muscarinic Antagonist): Tiotropium is the prototype; highly M3 receptor-selective, once daily; reduces exacerbations and improves lung function
- LABA (Long-Acting Beta-2 Agonist): Salmeterol, formoterol, vilanterol, indacaterol
- For patients remaining symptomatic on one, add the other: LAMA + LABA combination
Inhaled Corticosteroids (ICS)
- Less central than in asthma due to lower efficacy and increased risk of bacterial pneumonia (especially in elderly COPD patients)
- Recommended only for:
- Severe airflow obstruction (GOLD 3-4)
- History of frequent exacerbations (≥2/year)
- Overlap with asthma
- Elevated blood eosinophils (≥300 cells/µL) predict better ICS response
- Biomarker-guided ICS use is now recommended in international guidelines
Combination Triple Therapy
ICS + LABA + LAMA - for patients with frequent exacerbations despite dual bronchodilation, particularly if eosinophils are elevated.
Other Agents
-
Roflumilast (PDE-4 inhibitor): Selective phosphodiesterase-4 inhibitor; reduces exacerbation frequency in severe COPD with chronic bronchitis phenotype; oral once daily
-
Azithromycin (prophylactic): Daily azithromycin significantly reduces exacerbation frequency in patients with ≥2 exacerbations/year; monitor for QTc prolongation and macrolide resistance
-
N-acetylcysteine: Mucolytic; modest benefit in reducing exacerbations
-
Katzung's Basic and Clinical Pharmacology 16e, p. 565-566
Acute Exacerbation of COPD (AECOPD)
Definition
An acute worsening of respiratory symptoms (dyspnea, cough, sputum production or purulence) beyond normal day-to-day variation, requiring a change in medication.
Triggers
- Viral respiratory infections (most common - ~50-70%): rhinovirus, influenza, RSV
- Bacterial infections: H. influenzae, S. pneumoniae, M. catarrhalis; in severe COPD: Pseudomonas aeruginosa
- Air pollution, pulmonary embolism, pneumothorax, cardiac failure
Management of AECOPD
1. Bronchodilators: Intensify short-acting bronchodilators (SABA ± SAMA via nebulizer)
2. Systemic corticosteroids: Prednisolone 40 mg/day for 5 days; reduces treatment failure and speeds recovery
3. Antibiotics: Routinely given because exacerbations frequently involve bacterial infection; active against H. influenzae
- Beta-lactams (amoxicillin/amoxicillin-clavulanate), doxycycline, or azithromycin
- Fluoroquinolones (levofloxacin/moxifloxacin) for severe or frequent exacerbations
4. Controlled oxygen therapy: Target SpO₂ 88-92% (avoid excessive O₂ - risk of hypercapnic respiratory failure due to blunting of hypoxic drive)
5. Non-invasive ventilation (NIV/BiPAP): First-line for acute hypercapnic respiratory failure (pH <7.35, PaCO₂ >6 kPa); reduces intubation and mortality
6. Invasive mechanical ventilation: If NIV fails or contraindicated
Complications
| Complication | Notes |
|---|---|
| Cor pulmonale | Right heart failure from pulmonary hypertension; signs: edema, raised JVP, RV heave. Oxygen is the only therapy that improves this |
| Pulmonary hypertension | Prevalence varies; right heart catheterization is gold standard for diagnosis |
| Respiratory failure | Type 1 (hypoxemic) or Type 2 (hypercapnic + hypoxemic) |
| Secondary polycythemia | Compensatory response to chronic hypoxemia; increases viscosity and thrombosis risk |
| COPD-OSA Overlap Syndrome | ~16% of COPD patients; more severe nocturnal hypoxemia, hypercapnia, higher mortality; CPAP reduces exacerbations and mortality |
| Pneumothorax | Ruptured emphysematous bullae |
| Lung cancer | Shared risk factor (smoking); increased risk independent of smoking history |
| Depression/anxiety | Highly prevalent; substantially impacts quality of life |
- Murray & Nadel's Respiratory Medicine
Prognosis
- The BODE index (BMI, Obstruction, Dyspnea, Exercise capacity) is a validated predictor of mortality - superior to FEV₁ alone
- Each AECOPD accelerates FEV₁ decline and worsens long-term prognosis
- FEV₁ decline in COPD is ~50 mL/year (vs. ~25 mL/year normally), though cessation of smoking dramatically slows this
- 3-year mortality: Moderate COPD (GOLD 2) ~11%; Very Severe (GOLD 4) ~24%
Summary: Key Points
| Definition | Irreversible obstructive airflow limitation; FEV₁/FVC <0.70 post-bronchodilator |
| Cause | Smoking (#1), air pollution, AAT deficiency |
| Pathology | Emphysema (elastase destruction of alveoli) + Chronic bronchitis (mucus gland hyperplasia) |
| Hallmark symptom | Progressive dyspnea on exertion |
| Diagnosis | Spirometry (post-bronchodilator FEV₁/FVC <0.70) |
| Severity | GOLD 1-4 based on FEV₁ % predicted |
| First-line therapy | Smoking cessation + long-acting bronchodilator (LAMA or LABA) |
| Only mortality benefit | Smoking cessation, long-term oxygen therapy (when indicated) |
| Exacerbation treatment | SABA/SAMA, systemic steroids, antibiotics, controlled O₂, ± NIV |
Sources: Robbins & Kumar Basic Pathology | Fishman's Pulmonary Diseases and Disorders | Katzung's Basic and Clinical Pharmacology 16e | Murray & Nadel's Textbook of Respiratory Medicine | Textbook of Family Medicine 9e | Costanzo Physiology 7th Edition
Ambu bag
Reading File
Finding Sources
Finding Sources
Searching the Web
Ambu bag bag-valve-mask device components technique clinical use
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I have the diagram and full Miller's Anesthesia content. Now I have everything needed for a comprehensive answer. Let me compile it.
Ambu Bag (Bag-Valve-Mask / Manual Resuscitator)
What Is It?
An Ambu bag - formally called a bag-valve-mask (BVM) device or self-inflating manual resuscitator - is a hand-held device used to deliver positive-pressure ventilation to a patient who is not breathing adequately or at all. "Ambu" is an eponym from Ambu A/S, the Danish company that first developed it in 1937 (short for "Artificial Manual Breathing Unit").
It is one of the most essential emergency devices in medicine - found on every crash cart, in every ambulance, in every operating theatre, and used during CPR, pre-hospital emergencies, transport, and as backup whenever a mechanical ventilator fails.
- Miller's Anesthesia 10e, p. 2355
Components
The BVM has several distinct parts, each with a specific function:
| Component | Function |
|---|---|
| Self-inflating reservoir bag | Compressible silicone/rubber bag; automatically re-expands after each squeeze, drawing in air or oxygen |
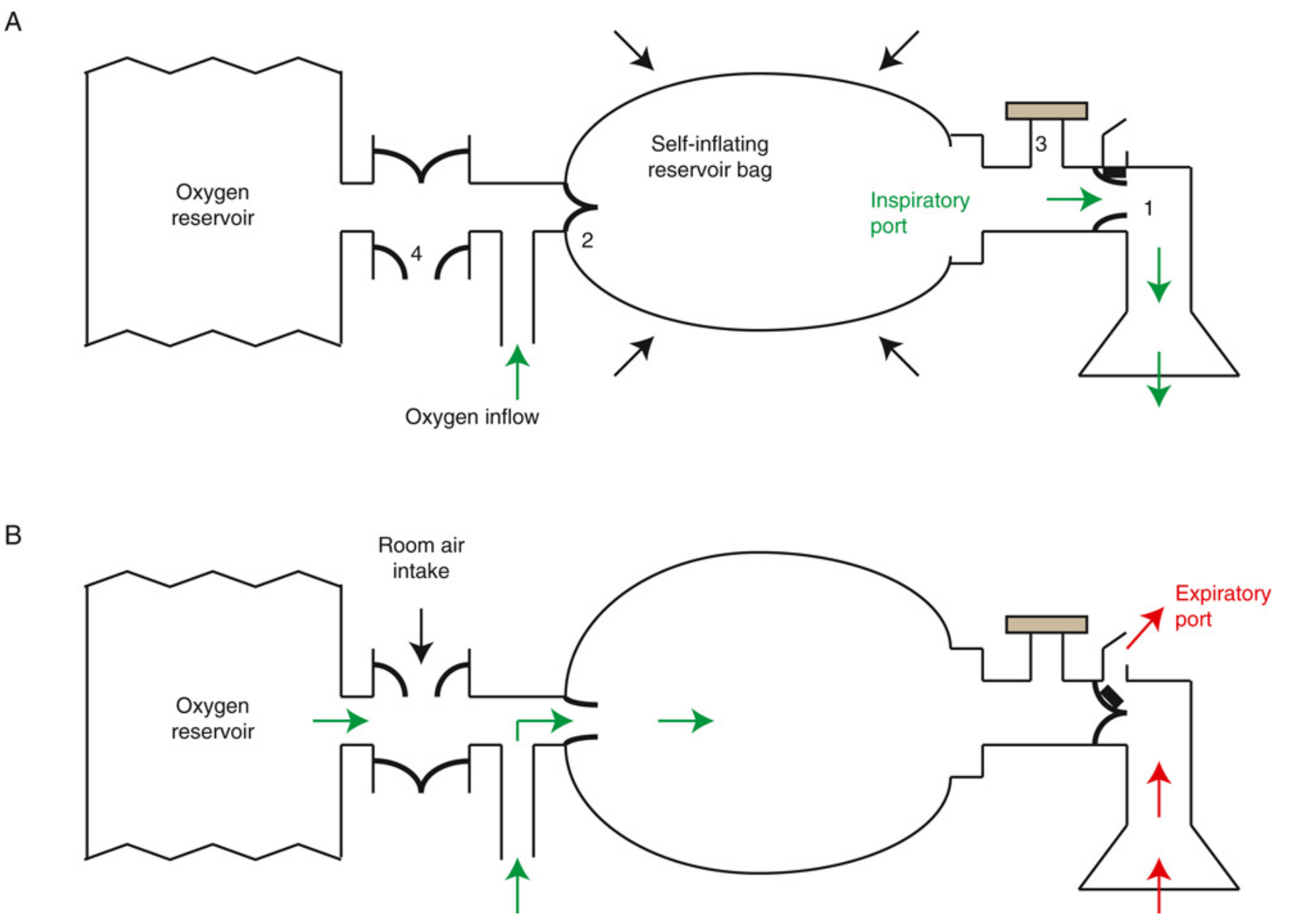
| Non-rebreathing valve (T-valve) | Directs gas flow: opens to patient during inspiration, closes and vents exhaled gas to atmosphere during expiration - prevents re-breathing of CO₂ |
| Bag inlet valve | One-way valve that allows the bag to refill with oxygen/air between compressions |
| Face mask | Silicone cushioned mask in various sizes (infant, pediatric, adult); creates a seal over mouth and nose |
| Oxygen reservoir | A collapsible bag or corrugated tube attached to the back of the bag; stores supplemental O₂ between squeezes, enabling delivery of near 100% FiO₂ |
| Pop-off valve (pressure-relief valve) | Limits peak inspiratory pressure (PIP) to 45 cm H₂O in pediatric/infant devices (ISO standard), preventing barotrauma; has an override |
| Oxygen inlet port | Connects to an external oxygen supply via tubing |
Gas Flow - How It Works
During inspiration (squeezing the bag):
- The non-rebreathing valve opens the inspiratory port
- Compressed gas from the bag flows into the patient's airway
- The expiratory port is simultaneously blocked
During expiration (releasing the bag):
- The inspiratory port closes
- The expiratory port opens, venting exhaled gas to the atmosphere (NOT back into the bag)
- The bag re-inflates by drawing in oxygen from the reservoir or room air
This one-way valve design means the patient never re-breathes exhaled CO₂ - a critical safety feature.
Oxygen Delivery
| Configuration | FiO₂ Delivered |
|---|---|
| No oxygen attached (room air only) | ~21% |
| Oxygen connected, without reservoir bag | ~40-60% |
| Oxygen connected at 10-15 L/min, with reservoir bag | ~90-100% |
The oxygen reservoir is essential for delivering high-concentration oxygen. Without it, oxygen is diluted by room air drawn in during bag re-inflation.
Sizes
| Size | Patient | Bag Volume |
|---|---|---|
| Neonatal | Premature/newborn | ~240 mL |
| Infant | <1 year | ~450 mL |
| Pediatric | 1-8 years | ~500 mL |
| Adult | >8 years | ~1600 mL (deliver only 400-600 mL per squeeze) |
Technique
1-Person Technique: The E-C Clamp
Used when only one rescuer is available:
- Position the patient: Head tilt-chin lift (or jaw thrust if c-spine injury suspected) to open the airway
- Select correct mask size: Should cover nose and mouth without pressure on the eyes
- Form the E-C clamp with the non-dominant hand:
- C: Thumb and index finger form a "C" shape, pressing down on the mask
- E: Remaining three fingers (middle, ring, little) form an "E" shape along the mandible, lifting the jaw upward into the mask
- Squeeze the bag with the dominant hand - one hand squeeze for adults, two-finger squeeze for neonates
- Watch for chest rise - this confirms effective ventilation
- Release the bag - allow passive exhalation
2-Person Technique (Preferred)
- One person uses both hands to maintain the mask seal (two-handed E-C grip)
- Second person squeezes the bag
- Produces better seal, more effective ventilation - strongly preferred in clinical settings
Key Ventilation Parameters
| Parameter | Recommendation |
|---|---|
| Tidal volume (adult) | 500-600 mL (visible chest rise; avoid over-ventilation) |
| Rate (adults with pulse) | 1 breath every 5-6 seconds (10-12 breaths/min) |
| Rate (CPR with advanced airway) | 1 breath every 6 seconds (10/min); asynchronous with compressions |
| Rate (CPR without advanced airway) | 30:2 compression-to-breath ratio |
| Rate (infants/children) | 12-20 breaths/min |
| Inspiratory time | ~1 second per breath |
Clinical Indications
- Cardiopulmonary arrest - during CPR when no airway has been placed
- Apnea - from any cause (drug overdose, anesthesia, drowning, trauma)
- Respiratory failure - as bridge before intubation
- Pre-oxygenation before intubation (3-5 minutes of 100% O₂ to maximize apnea tolerance)
- Patient transport - when mechanical ventilator unavailable
- Back-up device - if anesthesia machine ventilator or O₂ supply fails (required on every anesthesia workstation)
- Post-extubation - temporary support if patient fails to maintain adequate ventilation
- Neonatal resuscitation - at delivery
Hazards and Complications
| Complication | Cause | Prevention |
|---|---|---|
| Gastric insufflation | High pressures pushing air into esophagus | Use appropriate tidal volume; avoid excessive force; consider cricoid pressure |
| Aspiration | Gastric inflation leading to regurgitation | Correct technique; consider nasogastric tube in prolonged use |
| Barotrauma (pneumothorax) | Dangerously high inspiratory pressures | Use pop-off valve; one-hand squeeze technique; avoid aggressive squeezing |
| Hypoxia | Inadequate mask seal, poor technique | Two-person technique; check for chest rise |
| Hyperventilation | Excessive rate or volume | Monitor rate; avoid over-squeezing |
| Valve failure | Stuck or blocked non-rebreathing valve | Pre-use check; regular equipment inspection |
| Increased work of breathing | Resistance from non-rebreathing valve | For spontaneously breathing patients, minimise mask time; valve adds inspiratory resistance |
Key point from Miller's Anesthesia: "Dangerously high inspiratory pressures may be generated if the operator is untrained, uncareful, or if valve failure occurs. High pressures may lead to barotrauma or gastric insufflation."
Contraindications / Special Considerations
- Suspected cervical spine injury: Use jaw thrust instead of head tilt-chin lift; do not hyperextend neck
- Facial trauma: May make mask seal impossible; consider alternative airway (LMA, supraglottic airway)
- Facial hair: Impairs mask seal; use more gel/pressure or consider alternative
- Tracheostomy patients: Use appropriately sized pediatric mask directly over stoma, or use a speaking valve adapter
- COVID-19 / airborne infection: BVM creates aerosol; use a viral filter at the mask-patient junction; consider avoiding BVM when intubation is planned
Pre-Use Check (Checklist)
Before every use, verify:
- Bag re-inflates after squeezing (valve functioning)
- Mask seal is intact (no cracks)
- Oxygen reservoir attached and flowing
- Pop-off valve present (pediatric devices)
- All connections are secure
- Correct mask size selected for patient
BVM vs. Other Airway Adjuncts
| Device | Advantages | Limitations |
|---|---|---|
| BVM | No equipment skill required; immediate; portable | Requires continuous effort; seal may be difficult; gastric insufflation risk |
| LMA (laryngeal mask) | Hands-free; better seal; less gastric inflation | Training required; not definitive airway |
| Endotracheal tube | Definitive airway; protects from aspiration | Skill-intensive; can fail; complications with insertion |
Sources: Miller's Anesthesia 10e (Self-Inflating Manual Resuscitators, p. 2355-2357) | Medscape BVM Technique
This is a shared conversation. Sign in to Orris to start your own chat.